This issue of Clinics explores the concept of “preservation” rhinoplasty. At present, this topic is gaining considerable attention. As proponents of preservation suggest, a great number of problems we encounter in rhinoplasty are problems that were not present before the surgery; therefore, they can often be attributable to the deconstruction and reconstruction that took place. Preservation rhinoplasty should be viewed generally as a mindset to limit deconstructive steps in rhinoplasty when possible, understanding that these steps and those to later reconstruct provide the potential to create new problems that did not previously exist.
Key points
- •
“Preservation” refers not only to the dorsum but to any structure preserved for advantage or to avoid an undesired effect.
- •
The interdomal and intercrural ligaments provide the mechanism by which the caudal septum influences tip rotation and projection.
- •
These ligaments also maintain the symmetry of the paired alar cartilages and dome-defining points.
- •
Preservation of the interalar ligaments helps to maintain symmetry of the alar cartilages.
- •
Ligament preservation facilitates tip suspension with control over rotation, projection, and columellar show.
Introduction
This article of Clinics explores the concept of “preservation” rhinoplasty. At present, this topic is gaining considerable attention. But what is meant specifically and generally by “preservation”? The term came to popularity with the specific descriptions of midvault structural preservation for dorsal hump reduction by the push-down and let-down techniques. , These techniques are well characterized in other chapters, but in brief, in these approaches, the interfaces of septum and upper lateral cartilages along the dorsum are maintained while the hump is reduced, thereby “preserving the midvault.” Through this preservation of the dorsum, natural contours can be retained or enhanced, and the internal valves are left undisturbed. In contrast to humpectomy or component reduction of the dorsum, with preservation techniques, the potential sequelae of the act of opening the midvault and subsequently reconstructing it are avoided. ,
“Preservation” does not necessarily apply exclusively to the dorsum though; in general terms, it may be viewed as maintaining a particular structure for a particular desirable advantage rather than deconstructing it. , Many of the most common maneuvers used in rhinoplasty surgery involve deconstruction of structures and relationships with their subsequent reconstruction. As proponents of preservation suggest, a great number of problems we encounter in rhinoplasty are problems that were not present before the surgery; therefore, they can often be attributed to the deconstruction and reconstruction that took place. Rhinoplasty has become confusing and difficult to teach for many reasons. Among them include the complex and intricate methods we use to reconstruct structures and relationships that we ourselves chose to take apart. And often secondarily, we are compelled to use aggressive and/or nonanatomic methods in order to treat iatrogenic problems. In some instances, deconstruction is required in order to make a change pursuant to a goal of the operation; but in other instances, we simply restore structures to their original state. The latter questions the logic behind deconstruction. The concept of preservation suggests that we refrain from unnecessary deconstruction steps in primary rhinoplasty, thereby simplifying procedures to a certain extent and limiting the need for more complex secondary repairs.
Another example of preservation, described herein, pertains to the ligamentous anatomy that coalesces between the medial and middle crurae of the alar cartilages and the caudal septum. In open rhinoplasty, the lower lateral cartilages are routinely separated entirely from one another by dividing ligamentous structures in order to facilitate exposure for subsequent steps. The act itself of dividing the ligaments (“split tip approach”) is a means rather than an end; that is, it is a process-related deconstructive step. In closed rhinoplasty, delivery of the lower lateral cartilages is often combined with full transfixion. In both the split tip and delivery with full transfixion, tip ligaments and their connection to the caudal septum are surgically released. Later, the lower lateral cartilages are reapproximated with sutures to reconstruct the unity of the tip previously provided by the ligaments. In addition, vertical support grafts (eg, columellar strut or septal extension) are placed between the medial crurae to restore, reduce, or enhance projection. In open rhinoplasty and in closed rhinoplasty with a full transfixion incision, there had been consensus that extrinsic structural support via grafting was obligatory because the natural ligamentous support of the tip had been eliminated. However, these particular ligaments—the interdomal and intercrural ligaments—may be kept intact preserved. In doing so, the relationship between the 2 sides is preserved benefiting maintenance of symmetry. The ligamentous construct may then be used to resuspend the tip construct to the caudal septum, recapitulating the natural supportive relationship between these structures. We will investigate the rationale, techniques, and utility for preservation of these ligamentous connections. For clarity, these ligaments will be referenced specifically by name or collectively as the “inter-alar ligaments.”
Discussion
Determinants of Success in Aesthetic Tip Surgery
Surgery of the nasal tip can be incredibly elegant. Baris Cakir, in his recent superb text, analyzes the nasal tip and characterizes it as a set of fine polygonal shapes that form aesthetic angles, contours, surface characteristics, and light reflections. Advanced rhinoplasty surgeons may learn a great deal from these works to refine their techniques to achieve wonderful, artistic forms. However, basic tip surgery begins with only a few critical elements in order to get on base. In every rhinoplasty, the surgeon must deliver on 4 key structural relationships; shortcomings therein provide the basis of the most common causes for tip revision. The 4 critical elements are projection, rotation, dome symmetry, and proper columella show. The surgeon has control over these factors if he/she understands the anatomic influences on them. Typically, we intend to alter or adjust one or more of these structural relationships. In the normal nonoperated state, all of these aesthetic attributes are governed by the intrinsic integrity (including dimensions and strength) of the lower lateral cartilages and the interrelationship of the interdomal and intercrural ligaments with the caudal septum. The tip tripod described by Anderson characterizes tip rotation and projection based on the length and strength of the 2 lateral crurae and the paired medial crurae. A “tripod” is understood conceptually to be a stable/rigid support. But the tip tripod is mobile, not static; in fact, the footplates themselves generally do not articulate with the anterior nasal spine (skeletal base) and neither do the lateral-most extents of the lateral crurae. Yet the tip tripod is not floating freely in space; it is supported, so clearly there is something more to this. As stated by Bitik and colleagues “In the normal nasal anatomy, an anterior septal angle of sufficient height keeps the feet of the medial crua off the anterior nasal spine; the medial crura do not bear a significant load…”. A nonoperated aesthetic tip is supported by ligamentous structures that maintain the relationship between the alar crurae and their positions relative to the caudal septum. These structures are nicely described by Daniel and Palhazi and are summarized to follow.
The Interdomal and Intercrurl Ligaments
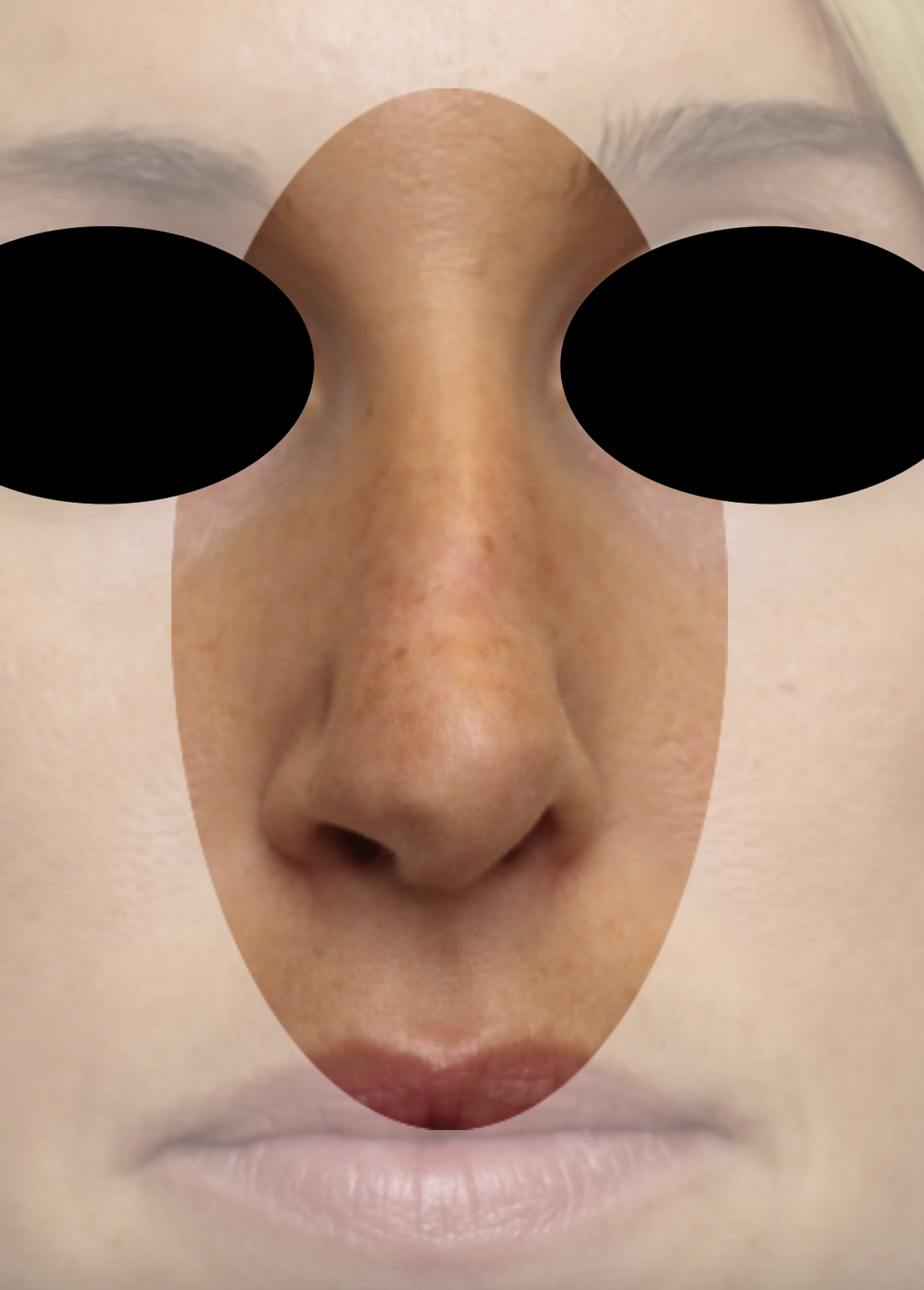
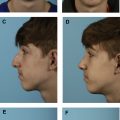
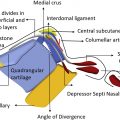
Drs Rollin Daniel and Peter Palhazi published perhaps the most highly detailed monograph of nasal anatomy in rhinoplasty. In it, they describe the form and purpose of the interdomal and intercrural ligaments ( Fig. 1 A-C). The interdomal ligament is a relatively discreet structure that connects the 2 middle crurae along the cephalic junction of the infralobular segment. It does not bind the domes themselves tightly together but maintains a close approximation of the posterior aspects of the middle crurae, permitting an open angle anteriorly to result in 2 separate, but generally aligned, dome-defining points. Therefore, the angle of divergence and the spatial symmetry of the domes are factors that depend on the presence of the interdomal ligament. When it is divided (along with the intercrural ligaments discussed later), as in “split tip” open rhinoplasty these important relationships are no longer supported and must be restored by a reconstructive technique. In order to reestablish the tip in space, the surgeon must reunite 2 separate structures and align the 2 properly not only with respect to the desired effect on projection and rotation, but to each other. Failure to do so would result in asymmetry of the domes ( Fig. 2 ).
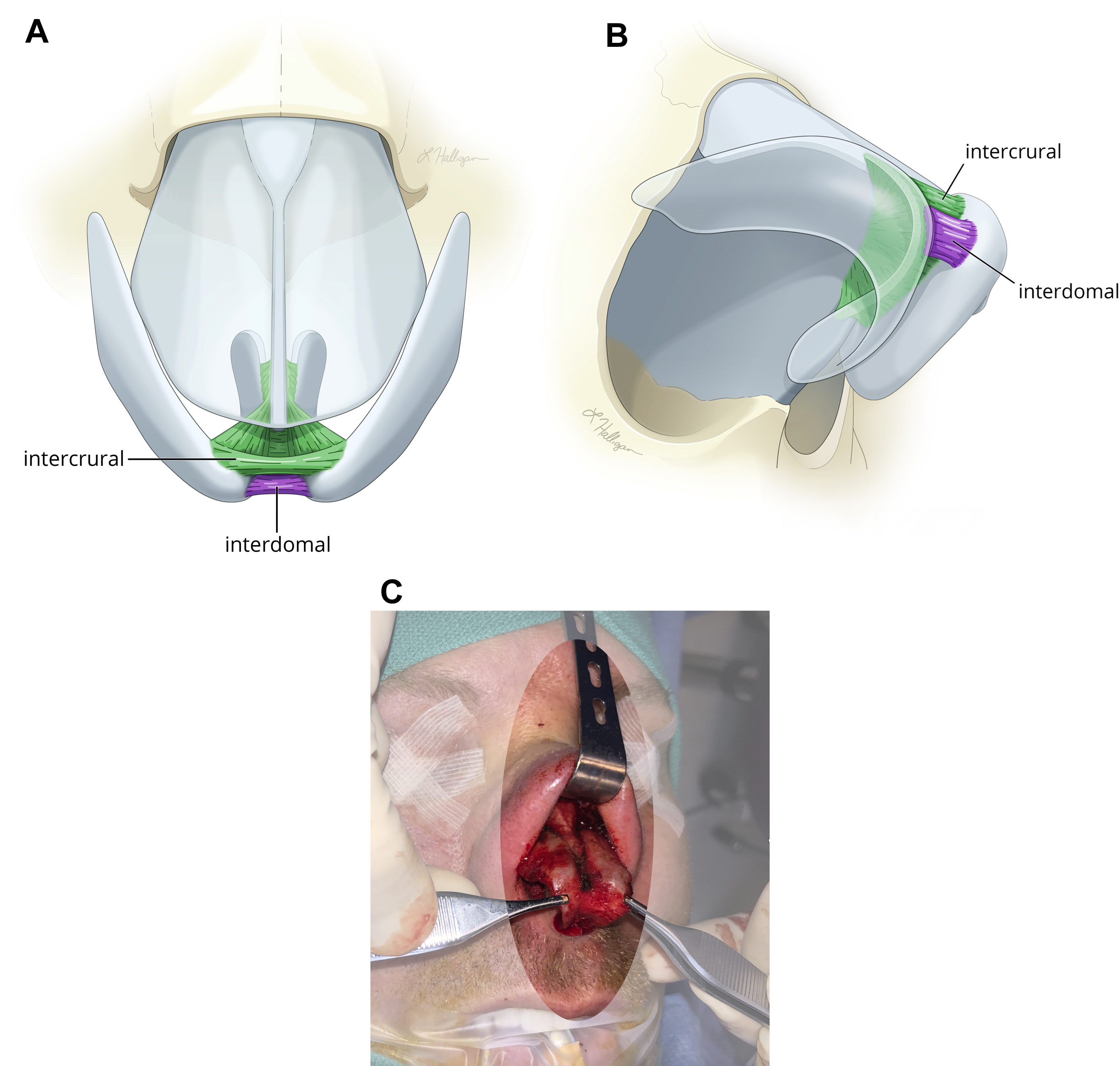
The intercrural ligaments are less frequently discussed, most frequently divided, and disproportionately important relative to our attention to them. These ligaments are much broader than the interdomal ligament, and they reside deep to it. They invest the posterior aspects of the medial and middle crurae over a long segment, wherein the fibers run transversely between the right and left sides. In this fashion, they play a similar but perhaps an even more important role in maintaining the symmetric interdependence between the right and left alar cartilages. The intercrural ligaments also include fibers that run in the anteroposterior plane from the posterior edge of the crurae to coalesce with the mucoperichondrium on each side of the septum. It is this important observation that explains the support relationship of the caudal septal structures to tip projection, and it explains deprojection with a transfixion incision.
The Relationship of the Tip to the Caudal Septum
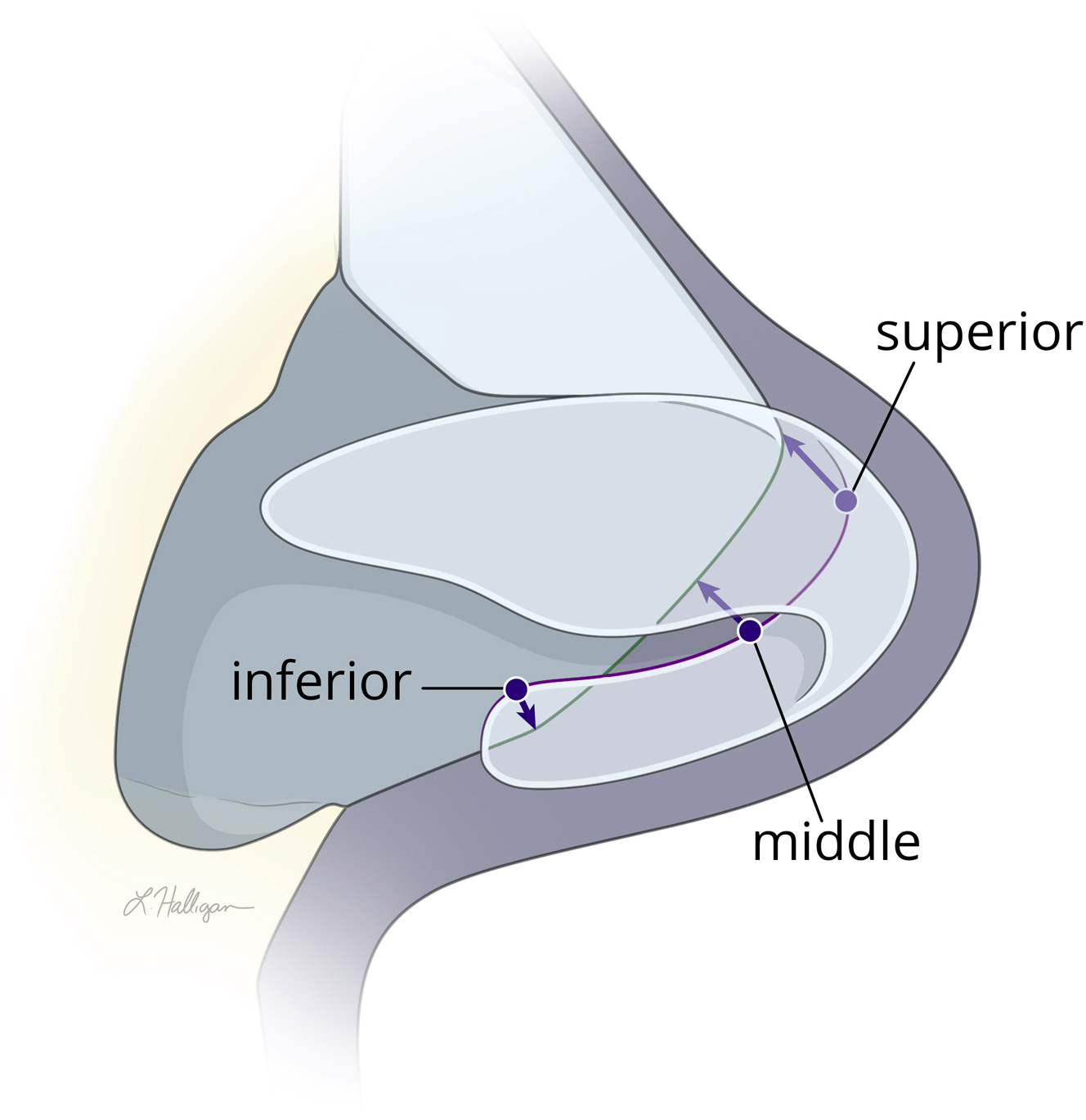
Daniel and Palhazi also characterized the spatial relationships between the alar cartilages and the caudal septum via their cadaveric dissections. Separately and unknowingly, we had undertaken a cadaveric study of 25 specimens to determine these relationships as well. Our studies, which support Daniel and Palhazi, suggest that there are 3 key landmarks along the caudal septum, which are defined ( Fig. 3 ). The anterior septal angle represents the junction between the dorsal and caudal septum and is also the most projecting point along the caudal septal line. The caudal point is the most caudal point along the caudal septum and often corresponds to the midseptal angle. The posterior septal angle is the junction point between caudal septum and the anterior nasal spine. The caudal septum is not situated entirely between the medial crurae—except at the footplates. The medial crurae are normally situated in front of, behind, or abutting the caudal septum at each of the caudal septal landmarks. In our analysis, the posterior edges of the medial crurae were anterior to the caudal septum at the anterior septal angle, (less) anterior or abutting at the midseptal angle, and overlapping the caudal septum at the footplates.
Related posts:
 Preservation Rhinoplasty
Preservation Rhinoplasty
 Incorporating Dorsal Preservation Rhinoplasty into Your Practice
Incorporating Dorsal Preservation Rhinoplasty into Your Practice
 Key Points in Subperichondrial-Subperiosteal Dissection
Key Points in Subperichondrial-Subperiosteal Dissection
 Dorsal Preservation Rhinoplasty
Dorsal Preservation Rhinoplasty
 Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
Piezoelectric Osteotomies in Dorsal Preservation Rhinoplasty
 Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Conventional Resection Versus Preservation of the Nasal Dorsum and Ligaments
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


