Tibia Lengthening and Deformity Correction With a Multiplanar External Fixator
Collin J. May
Operative Indications
The use of a multiplane external fixator for distraction osteogenesis is a powerful tool to address limb deformity and limb-length differences in pediatric patients.
Preoperative Planning/General Considerations
The goal of corrective surgery for limb deformity is a normal mechanical axis (of the involved bone and the limb overall) with joint lines that are parallel to the floor and limb lengths that are equal
Determining the osteotomy level, the degree of correction, the timing and rate of correction, and avoidance of injury to vital structures are all key aspects of the preoperative plan
Principles of external fixator stability are of critical importance in distraction osteogenesis. Stability increases with larger pin diameters, greater pin spread (on each side of osteotomy), increased pin number, and pins in multiple planes. Fine wires should be spread as close to 90° as anatomically possible, and at least 60° is preferable
Proper pin/wire insertion technique is critical to minimize the risk of postoperative infection. This includes placement of half-pins on subcutaneous bone borders (if possible), adequate skin incisions for pin placement, use of sharp drill bits (flutes of drill should be cleaned between uses) and irrigation to prevent thermal necrosis, and use of soft tissue protector when drilling to prevent soft tissue injury
Pins/wires should remain 15 mm from knee joint and 10 mm from ankle joint to avoid intracapsular placement
Half-pin diameters of 5 mm or 6 mm are preferred in the lower limb (but pin diameter should not exceed 1/3 the diameter of the bone). Pins with hydroxyapatite (HA) coating adhere better to bone and may lead to less frequent loosening and pin-site infection
Analysis of Deformity
A standing hips-to-ankles radiograph with patellas forward is the workhorse image for assessing coronal plane deformity and limb-length. Full-length lateral images of the limbs with the knee in maximal extension is helpful for assessment of sagittal plane deformity if present
Radiographs are assessed for mechanical axis, joint angles (mechanical or anatomic), magnitude of deformity or length difference, localization of the apex of the deformity, and visualization of any planned correction (Figure 25.1)
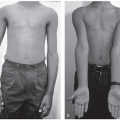
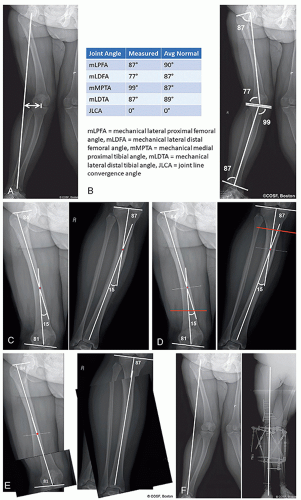 Figure 25-1 ▪ Preoperative deformity planning for a skeletally mature patient with genu valgum. A, Mechanical axis (line drawn from center of femoral head to center of ankle joint) passes lateral to midline suggesting valgus alignment of the limb. The distance to the midline is measured as the mechanical axis deviation (MAD as noted by bi-directional arrow). B, Frontal plane measurements of patient’s mechanical joint angles. Note both distal femur and proximal tibial angles are creating a valgus deformity. C, Normal anatomic joint angles applied to femur and tibia, respectively, to determine the apex of the deformity for each bone. D, Level of osteotomy determined (red line) as well as bisector of obtuse angle at the apex (dashed line). Note that osteotomy performed away from deformity apex will result in necessary translation of bone to ensure alignment of mechanical axes. Hinge point for correction should be along correction bisector line. E, Simulated correction at level of planned osteotomy to correct axis as indicated by dashed line and red dot. Note translation of bone fragments given osteotomy away from apex of deformity. F, Preoperative and postoperative radiographs showing normalized mechanical axis after deformity correction. (Courtesy of Children’s Orthopaedic Surgery Foundation.) |
Equipment
Multiplane external fixator devices are available from multiple manufacturers and generally are comparable in their ability to achieve the goals of stable fixation and accurate correction. For the purposes of this chapter, we will discuss ring fixators, though monolateral and hybrid options exist
Drill
Osteotome
Sagittal saw
4.5 mm cannulated screw set
Examination
A comprehensive physical examination should be performed, including neurologic assessment, Gait evaluation, and limb examination standing, supine, and prone for rotational and angular limb deformity as well as limb-length discrepancy. Presence of joint contractures should be noted, as these will impact radiographic assessment of limb-length differences
Positioning
Supine
Bump under ipsilateral hip to prevent leg from externally rotating
Leg elevated a few centimeters on folded sheets or blanket platform to raise above other lower limb for easier access to medial side
Nonsterile tourniquet applied to thigh (for use during approach to osteotomy but lowered before drilling bone to avoid thermal necrosis)
C-arm and fluoroscopic image intensifier should be placed on the opposite side of the patient as the operative limb (surgeon will need to place initial fine wire(s) from lateral to medial)
Surgical Approach
Osteotomy of the tibia is performed through a midline longitudinal incision overlying the metadiaphyseal crest of the tibia, approximately 4 to 5 cm in length. Osteotomy of the fibula is typically performed in the distal 1/3 of the fibula, and at least 8 to 10 cm above the tibiofibular syndesmosis through a 2 to 3 cm lateral longitudinal incision.
Technique in Steps
This procedure is performed under general anesthesia. Careful consideration should be given regarding use of regional anesthesia due to the potential risk of postoperative compartment syndrome and the need to intraoperatively monitor for nerve stimulation during placement of fine wires. Similarly, paralytic agents should be avoided (or should have worn off) when placing fine wires around the knee to monitor for peroneal nerve stimulation
Ring selection
Ring size can be preoperatively templated, based on the soft tissue shadow of the anteroposterior (AP) and lateral x-rays of the leg (Figure 25.2)
Appropriate size rings should be confirmed intraoperatively prior to placement to ensure that rings do not impinge on soft tissue around the full circumference of the leg (ring should remain at least 2 cm from the skin surface to account for postoperative swelling)
A two-thirds ring is typically chosen at the proximal tibia to allow knee flexion beyond 90° (due to posterior opening), and full rings are used in the tibial shaft and distal tibia
Proximal and distal rings can be different sizes
Fibula osteotomy
Osteotomy of the fibula is necessary to allow for appropriate tibial lengthening and deformity correction. For most proximal tibial osteotomies, the fibula osteotomy is distal to the tibial osteotomy in the middle to distal 1/3 of the bone. Osteotomy should be performed at least 8 to 10 cm above the syndesmosis
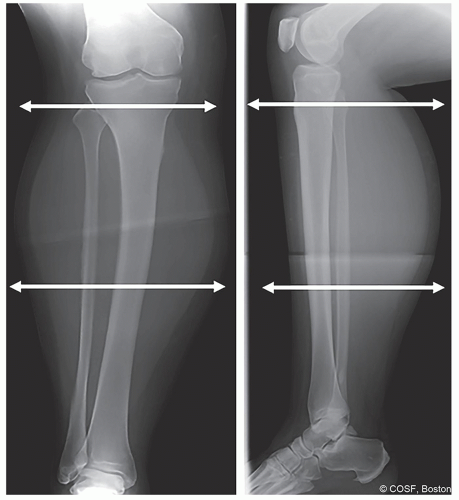
Figure 25-2 ▪ Preoperative radiograph (anteroposterior [AP] and lateral) used to measure soft tissue shadow for sizing of tibial rings as noted by directional arrows. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
Osteotomy should be performed in an oblique plane. Orientation of this plane is important when rotational or angular correction is planned. For correction of external tibial torsion, the cut orientation is proximal-anterior to distal-posterior. For correction of internal tibial torsion, the obliquity should be proximal-posterior to distal-anterior (Figure 25.3)
Steps
Longitudinal incision 2 to 3 cm in length overlying the course of the fibula
Blunt dissection onto lateral compartment is performed, paying close attention to avoid injury to either superficial peroneal or sural nerves (depending on relative anterior or posterior location of incision, respectively)
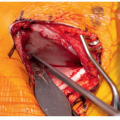
Fascia is opened, and peroneal musculature is retracted anteriorly. Fibula periosteum is exposed and incised longitudinally. Periosteum is elevated, and small blunt Hohmann retractors are placed in the subperiosteal plane anterior and posterior to the bone (adequate protection of the soft tissue is critical; as significant bleeding can occur from the interosseous veins or arteries if injured)
A 2.5 mm drill is utilized to make a series of drill holes laterally, which are fanned in the appropriate plane posteriorly, anteriorly, and medially
An osteotome is utilized to complete the cut
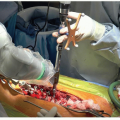
Mobility of the proximal and distal fragments must be confirmed by visualizing translation under fluoroscopy (Figure 25.4)
The wound is irrigated and closed in layers
Syndesmosis screw
In cases of limb-lengthening or significant limb deformity correction, fixation of the fibula proximally and distally is necessary. Proximal fixation is provided by initial fine wire through the
fibula head attached to the proximal ring of the fixator. Distal fixation is through the syndesmosis screw
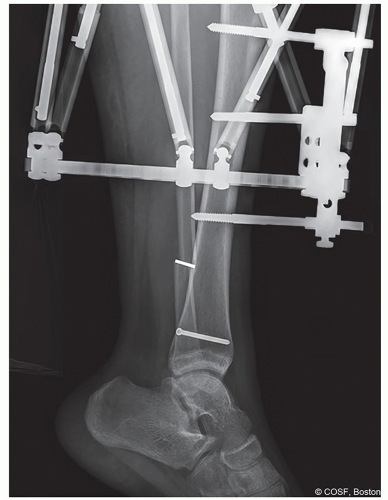
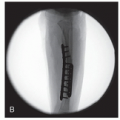
Figure 25-3 ▪ Postoperative lateral radiograph showing obliquity of fibular osteotomy (white line). (Courtesy of Children’s Orthopaedic Surgery Foundation.)
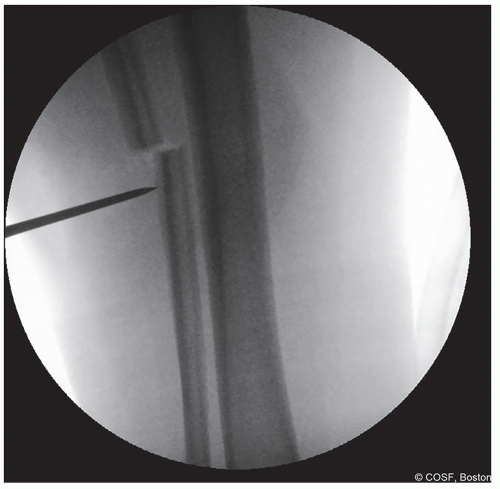
Figure 25-4 ▪ Intraoperative anteroposterior (AP) fluoroscopic image demonstrating displacement of the fibular fragments with an osteotomy to ensure that the fibula osteotomy is complete. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
For most adolescent and adult patients, we prefer to use a single 4.5 mm cannulated screw through three cortices (for small children, smaller cannulated screws or fine wire attached to the distal ring can be utilized)
Steps
Guidewire from the 4.5 mm cannulated screw set is placed from lateral to medial parallel to the joint line at approximately 2 to 5 cm above the joint at the level of the syndesmosis (Figure 25.5)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree