Thyroglossal Duct Cysts
Mark Felton
Jugpal S. Arneja
Neil K. Chadha
DEFINITION
The most common congenital midline neck cyst1
Caused by embryological remnants of thyroid gland formation
ANATOMY
These cysts can exist anywhere from the base of tongue to the level of the thyroid gland as they form in remnants of the thyroglossal duct (FIG 1).
75% are at the level of the hyoid bone.
PATHOGENESIS
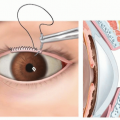
During week 4 of embryological development, the thyroid develops between the 1st and 2nd pharyngeal pouches from floor of the pharynx at the level of the foramen cecum (posterior 1/3 tongue) (FIG 2).
This becomes a bilobed diverticulum and descends through the neck to reach final position anterior to the tracheal cartilages. As it descends through the neck, it leaves a tract.
The tract usually atrophies after 5 to 10 weeks.
Caudal attachment of the tract may remain as the pyramidal lobe of the thyroid.
Failure of the tract to obliterate can lead to cyst formation at any point throughout the tract length (FIG 3).
NATURAL HISTORY
Thyroglossal duct cysts are present at birth but may not be clinically apparent until enlarged secondary to infection.
They present as a midline neck swelling most commonly in childhood and adolescents.
90% present as midline neck swellings only, but infection and formation of a secondary discharging sinus are possible (10%).
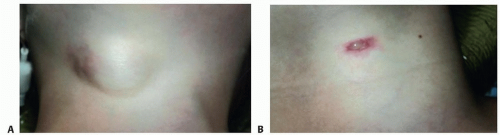 FIG 1 • Clinical photographs of anterior neck showing TGDC. A. Scar tissue is from previous site of infection with skin breakdown. B. TGDC with central discharging sinus. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Midline neck cyst.
May elevate on swallowing and tongue protrusion.
With a history of infection, there may be signs of an abscess or sinus formation with discharge.
IMAGING
Ultrasonography of the neck and thyroid to evaluate the swelling and confirm a normal thyroid is present (FIG 4).
In the absence of a thyroid gland, a thyroglossal duct cyst (TGDC) may contain the only functioning thyroid tissue.
Nuclear imaging in the form of radioactive iodine scan can be used if there is doubt regarding normal functioning thyroid.
Thyroid function blood tests are only required if presence of normal thyroid tissue is in question.
DIFFERENTIAL DIAGNOSIS
Midline dermoid cyst
Sebaceous cyst
Midline branchial cleft cyst
Lymph node
Ectopic thyroid tissue
Laryngocele
Thyroid carcinoma within TGDC
NONOPERATIVE MANAGEMENT
Conservative watchful waiting in children until over age 12 months
Advise there is a risk of infection with possible sinus formation if conservative approach is taken.
Antibiotics with possible aspiration if the cyst becomes infected and forms an abscess. It is not recommended to
incise and drain an infected TGDC because this risks sinus formation with chronic discharge.
Uncommonly infection and inflammation may actually lead to closure of the residual duct and resolution of symptoms.
Theoretical risk of malignant change of thyroid tissue within TGDC if left indefinitely, with less than 1% of excised TGDCs having a primary carcinoma on histology.2
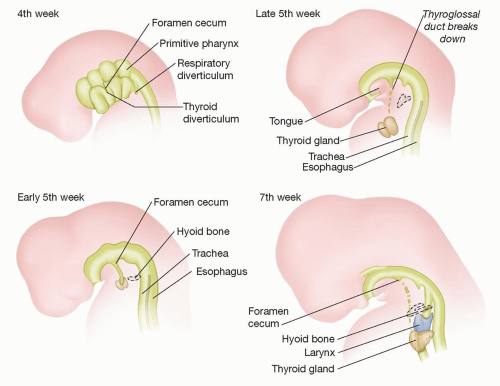 FIG 2 • Thyroid development. |
SURGICAL MANAGEMENT
Preoperative Planning
Review ultrasound scan result to confirm that normal thyroid tissue is present in the usual location.
Examine preoperatively to check that swelling is still present.
Assess ideal level for placement of a transverse incision that will provide exposure from the level of the suprahyoid muscles to the superior border of the thyroid gland for removal of the TGDC (typically approximately midway between the palpable landmarks of the hyoid and upper thyroid notch).
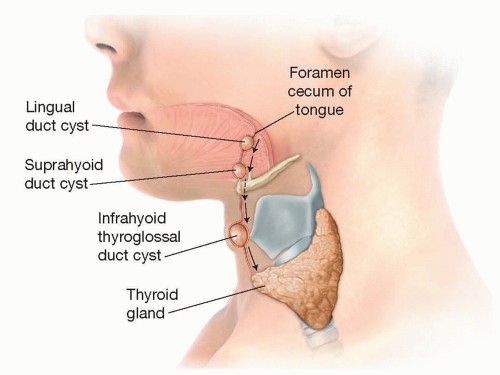 FIG 3 • Pathogenesis of TGDC development. |
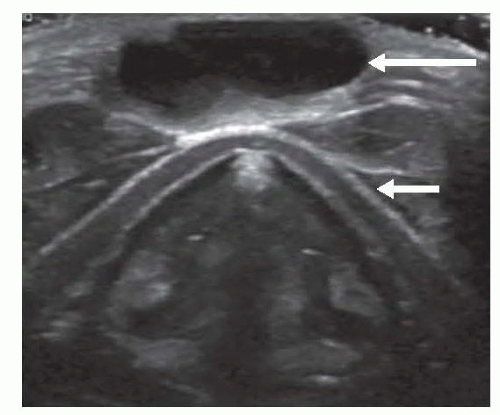 FIG 4 • Ultrasound scan of TGDC (long arrow) overlying thyroid cartilage (short arrow). |
Positioning
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


