Fig. 3.1
Mechanism of cryodestruction. A direct cell damage by intracellular lysis, B direct cell destruction by extracellular dehydration, C vascular occlusion and damage, D inflammatory damage necrosis, necroptosis, E silent cell absorption – apoptosis
The direct damage contributes to cell necrosis, release of intracellular contents, and extracellular matrix damage, leading to activation of the short-lived, nonspecific innate immune response and significant inflammation. The direct cell injury resulting necrosis is typical at short distances from the center of the cryogenic lesion where the lower temperatures achieved. Temperatures of approximately −20 °C have been suggested for adequate tissue destruction; however, it is worthwhile to note that malignant cells may be more resistant to cryoinjury and require lower temperatures [16, 17]. Current standards recommend tissue temperatures of 50 °C to −60 °C degrees for effective ablation of malignant tissue [15, 16].
Within higher, sublethal, temperature ranges, cryoablated cells in malignant tissues such as in human colon carcinomas have been shown to undergo apoptosis instead of necrosis [18]. Markers for apoptosis can be observed in cells 4 h after freezing. The percent of apoptotic colon carcinoma cells is maximized at −25 °C with approximately 28 % of cells demonstrating elevated apoptosis markers. Colder temperatures result in lower apoptotic rates likely secondary to a shift towards the mechanism of cell injury described previously, namely, a predominantly cryolytic type of cell death and tissue necrosis (Fig. 3.1). It is important to note that cell death by apoptosis is the primary mechanism of cryoablation in the peripheral zone of the cryogenic lesion (away from the center of cryolesion), given the inherent higher temperatures found away from the source of freezing. Also notable is that apoptotic cell death does not induce an inflammatory response as seen during necrosis. The balance between apoptosis and necrosis may play an important role in whether a tumor undergoing cryoablation is destroyed or not or whether strong immune response towards the tumor has been induced or not. Furthermore the release of endogenous “danger signals” (fragments of DNA, RNA, hyaluronan products, long CpG sequences, high-mobility group protein B1 (HMGPB1) or amphoterin, TNF-alpha, IFN-alpha, IL-6, IL-1β, heat shock protein (HSP), uric acid, ATP, UTP) has significant proinflammatory properties thus contributing to immune stimulation [19]. Activation of TNF-alpha and binding of FAS-ligand produces necroptosis of the affected cells which is also immune mediated and associated with inflammation in comparison to apoptosis where the death of the cells is silent, with minimal or no inflammation. The apoptotic cell death is main mechanism of tumor-cell turnover to suppress inflammation and avoid protective immune response.
Indirect cell damage also occurs after cryoablation due to the damaging effects of ice crystals on the wall of blood vessels and the lining endothelium. After thawing and reperfusion of affected vessels, platelets become activated causing thrombus formation and subsequent local tissue ischemia. The vascular stasis results in further tissue damage post cryoablation. Furthermore, indirect damage occurs due to immunological response that follows an initial inflammatory response secondary to cryosurgery (Table 3.1). This process of immune system activation is studied by cryoimmunology and is discussed in detail in the following sections along with the development of protective immune response.
Table 3.1
Mechanisms of cell death and tissue injury after cryosurgery
Direct injury | Indirect injury |
|---|---|
Extracellular matrix ice crystal formation | Thrombus formation |
Intracellular osmotic dehydration | Vascular stasis and ischemia |
Enzymatic conformational changes | Innate and adaptive immune system-driven injury |
Intracellular ice crystal formation and cell bursting |
3.3 Cryosurgery-Induced Inflammatory Response and Immune Activation
The cornerstones of cryoimmunology can be described as processes involving inflammation and immune attack against damaged target tissue that follow local cryoablation. As described previously, extracellular and intracellular antigens are released after cryosurgery secondary to membrane disruption and cell death. Furthermore, extracellular matrix releases preformed inflammatory cytokines initiating a strong immediate inflammatory response. For instance, studies have demonstrated that levels of IL-1β, IL-6, and TNF-α are elevated after cryoablation of large hepatic metastases [20–22]. IL-12 and IFN-γ have also been detected shortly after freezing [1]. Prostate tumor cell gene expression of several cytokines implicated in stimulating immunity, such as IL-2, IL-15, IL-12p40, IL-18, and TNF-α, was demonstrated to increase after cryoablation. Cells including neutrophils, macrophages, and lymphocytes are recruited by the ongoing inflammatory process and add to the cytokine milieu by secreting other inflammatory mediators marking the activation of the innate immune response [23–25]. Cell infiltration including APCs and T cells may be mediated by the expression of proteins such as heat shock protein-70 (HSP 70) from tumors undergoing cell death [26]. As quickly as within a few hours after cryosurgery, polymorphonuclear (PMN) leukocytes are also recruited to the lesion site and infiltrate the area. Their migration peaks after 3 days and occurs along with an increasing macrophage infiltration that peaks at 7 days [27]. NK cell activity was also shown to increase in a mammary adenocarcinoma mouse model after cryoablation [1].
Following innate immunity activation, the acquired immune response begins with the actions of antigen-presenting cells (APCs). APCs, namely, macrophages and dendritic cells (DCs), engulf the antigens released by cryoablation and present them to T cells via major histocompatibility complex (MHC) Class I and II. A cytotoxic and humoral response follows with APC presentation of antigen to lymphocytic cells. Dendritic cells loaded with antigens now migrate to lymph nodes where they undergo maturation, becoming efficient APCs able to prime naïve antigen-specific T cells. They upregulate their maturation gene expression including IL-1, Fas, CDKN1A, ostoprotegrin, and CXCR4, as well as their expression of immunostimulatory cytokines including IL-1β, IL-12p40, IL-15, TNF-α, and IFN-γ. DC maturation estimated by flow cytometric measurement of the surface marker CD86, a ligand that participates in T cell priming, was shown to increase eightfold after freezing prostate cancer cells. Moreover, the expression of class-II MHC, which is a required component of antigen presentation and activation of T cells, was doubled [28].
As APCs present antigens to naïve helper T cells (Th) in the presence of IL-12, T-cell differentiation into Th-1 cells occurs. Th1 cells release IL-2, IL-12, IFN-γ, TNF-α, and GM-CSF, which in turn participate in activating cytotoxic (CD8) T cells. B-cell proliferation and differentiation into antibody-producing cells also occur upon expression of IL-4 by naïve helper T cells, resulting in T-cell differentiation into Th-2 cells. Th-2 cells express IL-4 and IL-5 cytokines promoting B-cell differentiation into antibody producing cells. The afore-described cascade of events marks the initiation of the adaptive arm of the immune response triggered by cryoablation. This response is specific against the antigens derived from cryoablated cells, possibly priming systemic antitumor activity. The specific CD8 T cells now contribute not just to a killing of the primary tumor, but are also carried by circulation to bind to distant foci of metastatic tumor, resulting in antitumor-specific response and killing of tumor cells by necroptosis (Fig. 3.2).
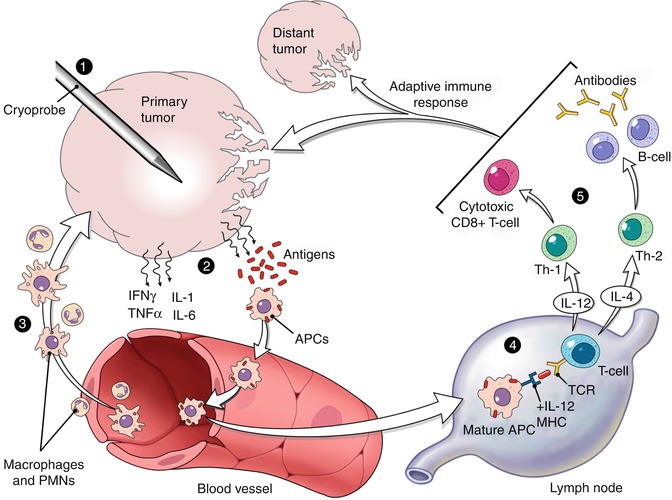
Fig. 3.2
Inflammation and immune activation upon cryoinjury. 1 tumor cryodestruction, 2 antigen and cytokine release, 3 inflammation with polymorphonuclear cells, macrophages, and antigen-presenting cells (APC) stimulation, 4 development of the immune response both humoral and cellular in tumor-associated lymph nodes, priming of the cytotoxic T cells, 5 effective immune response – killing of the primary tumor and distant disease
3.4 Cryoablation and Tumor Microenvironment
Tumor survival and progression are partly due to their ability to evade the host immune system. Tumor microenvironments appear to modulate immune response by regulating immune cell phenotype and function both locally and systemically. The knowledge and control of tumor microenvironment are becoming as important as knowledge and control of cancer cells. For instance, patients with progressing hepatocellular carcinoma (HCC) have been demonstrated to have increasing levels of peripheral CD4 + CD25+ cells, detected by flow cytometry [29]. CD4 + CD25+ cells are some of the best described T-regulatory cells (Treg) that downregulate the immune system. Increases in Treg cell levels have also been shown in other cancers including gastric, lung, pancreatic, and breast cancers [30]. It has been speculated that the response to cryoablation may vary depending on tumor type and the level of Treg cells present. For instance, patients’ HCC response after cryoablation with argon-helium cryoprobes to freezing temperatures of −135 °C appeared to be dependent on the quantities of circulating CD4 + CD25+ Treg cells prior to treatment. Patients with HCC regression after cryoablation showed significantly decreased Treg frequency by flow cytometry. In contrast, patients with HCC progression and recurrence showed increased Treg cells. Treg frequencies were approximately 6.9 % in early-stage HCC, 8.8 % in intermediate-stage HCC, 10.3 % in advanced-stage HCC, and 13.4 % in terminal-stage HCC. These results indicate the role of immune downregulation in tumor survival, even after therapy. Furthermore, immune-inhibitory cytokines like TGF-β, IL-10, and PG E2 also contribute to suppression of cytotoxic immune response. These data may also help explain why cryoablation is at times ineffective in treating certain tumors, since cytotoxic T-lymphocyte may take at least 6 h to kill one tumor cell in tumor microenvironment (Fig. 3.3a, b), while on the contrary B cell in the healthy lymph node takes less than 60 min to kill the tumor cell [31]. In addition, tumors recruit myeloid-derived suppressor cells (MDSC) from the bone marrow transforming them to tumor-associated macrophages (TAM), thus blocking and suppressing antitumor immune response and enhancing tumor survival. It is likely that adjunctive therapy may be necessary to obtain the full potential of antitumor effects of cryoablation.
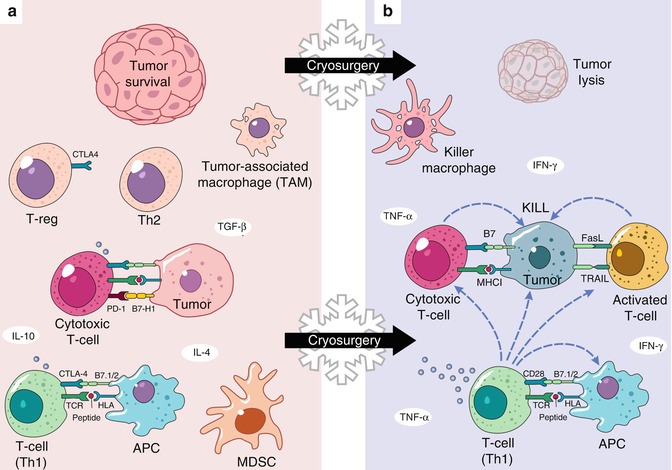
Fig. 3.3
(a, b) Tumor microenvironment switch induced by cryosurgery. (a) Tumor survival. Th-2 – immune-inhibitory microenvironment. (b) Tumor lysis. Th-1 immunostimulatory microenvironment. Abbreviations: MDSC myeloid-derived suppressive cells, APC antigen-presenting cells, CTLA-4 cytotoxic T-lymphocyte antigen 4, PD1 programmed cell death receptor 1, TCR T-cell receptor, HLA major histocompatibility complex
Other studies have suggested that cryodestruction may counteract the tumor microenvironment anti-immune activity. The immunological response to cryoablation in a renal cell cancer animal model demonstrated higher IFN-γ to IL-4 levels suggesting an increase in Th-1:Th-2 ratio and demonstrating the interplay between inflammatory cytokines and activation of the immune system after cryosurgery. The increase in Th-1 to Th-2 ratio opposes the anti-immune response effects of renal cell carcinoma (RCC) previously shown [32].
Sabel and colleagues have elegantly demonstrated how rate of freeze could affect the resulting immune response after cryoablation of 4T1 breast carcinoma in balb/C mice [33]. Two weeks after inoculation of mice with the tumor cells, the animals were divided into four groups (control, surgical resection group, and low- and high-freeze group). High-freeze technique used argon cryoprobe for 30 s and duty cycle of 100 %, while low-freeze technique used the same probe, but with duty cycle of 10 % for several minutes. One week later, high-freeze group demonstrated significant reduction in CD4 + CD25+ T-regulatory cells in examined tumor lymph nodes, while the number of cytotoxic CD8+ cells was not significantly affected. Both, low-freeze group and surgery group had dramatically higher Treg levels, producing more immunosuppression and increased levels of lung metastases in the latter. Furthermore, the cytotoxic CD8 T-cell responses to exposure to tumor cells in vitro were almost tripled in the high-freeze group in comparison to low freeze, surgery, and control. Specific evidence of antitumor activity following cryoablation is discussed in more detail in the following section. We can now emphasize that cryoablation apart from direct and indirect tumor cell damage may also contribute significantly to a change from tumor-supportive (Th-2) tumor microenvironment to tumor-suppressive one with Th-1 predominance (Fig. 3.2).
3.5 Cryosurgery-Induced Primary and Metastatic Antitumor Activity
The formation of specific antibodies against cryoablated tissue antigens was demonstrated many decades ago. Early experiments with cryoablation of the rabbit benign prostate, seminal vesicle, and bulbourethral glands showed that autoantibodies specific to these tissues could be isolated from the serum of respective animals. These antibodies did not react with other autologous tissues such as the kidney, liver, or thyroid and did not recognize human-derived tissues, demonstrating the specificity of the antibodies for the cryoablated tissue [34]. Autoantibody formation was detected as early as within 7–10 days of cryoablation, suggesting that at least period of 2 weeks should be allowed for the first attempts to detect the immune response. The same study also explains the lack of the immune response detection in sera analyses performed earlier in the immediate post-freezing period [1]. These data inspired more research exploring the generation of immune system-targeted therapy against malignant tissues with cryosurgery. Cryoablation of prostate cancer has become increasingly popular in urological oncology and has shed light into the widespread potential applications of cryoimmunology as primary or adjuvant therapy for cancer. The reports of cryosurgery of prostate tumor demonstrated that antibodies specific to prostate cancer antigens were found in the serum after the procedure [35]. Interestingly, despite increased antibody levels, actual secondary tumor growth and tumor histology were unchanged. Several other reports have suggested similar contradictory data in regard to the actual efficacy of tumor regression after cryotherapy and are discussed in more detail in a separate section later in this chapter. However, most of the investigators at the time were not able to measure the level of actual cellular/cytotoxic immune response, which would be more specific for immune-mediated tumor destruction.
Later studies, where better immunological assays became available and more controlled and precisely measured cryodestruction feasible, have demonstrated impressive benefits of cryosurgery for cancer treatment in human patients. A retrospective study comparing the effects of targeted cryoablation of prostate cancer and control therapies including brachytherapy, external beam radiation, or 3-dimensional conformal radiation demonstrated that cryosurgery resulted in equal or superior disease free rates [36]. The mean follow-up time was 5.3 years, and the outcome measures were prostate-specific antigen (PSA)-based cutoffs. No serious complications were reported and only minimal morbidity was observed.
Patients with nonmetastatic prostate cancer have also been treated using a percutaneous approach to cryoablation [37]. Biopsy of treated tissue after percutaneous cryotherapy showed elevated levels of TNF-α and IFN-γ as well as increased Th-1:Th-2 ratio. A significant increase in peripheral blood mononuclear cells was also shown along with increased cytolytic activity of cytotoxic T-lymphocytes against autologous prostate cancer cells. This activity was specific to prostate tissue. It is prudent to note, however, that despite evidence of immune system activation, this approach was not sufficient to prevent cancer relapse. Moreover, the level of differentiation of the prostate tumor cells also plays a role in the effectiveness of cryosurgery. More differentiated tissue proved to be associated with advantageous survival in patients [38], since the capacity for proliferation decreases in cells as they mature and differentiate.
Some of the rationale for the limited effectiveness of cryosurgery in eradicating tumors may be explained by the expression of inhibitory T-cell coreceptor CTLA-4. CTLA-4 binds B-7 at the surface of APCs. Their interaction inhibits T-cell activation by reducing the expression of IL-2. CTLA-4 is the target of a recently FDA-approved antibody drug, ipilimumab, which can diminish this immune-inhibitory process and allow a more robust response. Given the potential to enhance the antitumor effects of thermal ablation, the adjuvant use of ipilimumab along with cryotherapy was demonstrated in a recent study [39]. A mouse model of primary prostate cancer treated with combination of cryoablation and ipilimumab was utilized showing that the growth of secondary tumors seeded at distant sites after initial thermal ablation of the primary tumor (also known as tumor rechallenge) was slowed and tumor rejection was triggered. The secondary tumors were found to be highly infiltrated by CD4+ T cells as well as CD8+ T cells and relatively less T-regulatory cells. This cessation in growth was not observed after cryoablation alone. These results are promising and suggest augmentation of antitumor immunity with combination therapy. Another possible mechanism of tumor survival is activation PD-1 (programmed cell death) receptor on active T and B cells which blocks their activity when stimulated by tumor cells produced ligands PD-L1/PD-L2. Thus, the binding of PD-1 receptor has profound immunosuppressive properties and is crucial for tumor survival [40]. Promising new studies are now on the way in metastatic melanoma with new PD-1 inhibitor lambrolizumab [41], which could also serve as a potential adjuvant to cryodestruction in selected cases.
Many other types of cancers have been targeted using cryoimmunology. For instance, tumors created by human melanoma cell lines that were xenografted in mice and treated with cryoablation were evaluated for necrosis-induced recruitment of inflammatory cells and induction of immune-mediated activity [27]. After freezing, congestion, edema, and endothelial cell activation were detected, as well as a polymorphonuclear leukocytes infiltration into the tumor. Antibodies against the tumor cells were also detected.
Related posts:
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Role of Reflectance Confocal Microscopy in Cryosurgery
Role of Reflectance Confocal Microscopy in Cryosurgery
 Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
Cryobiopsy, Cryoanesthesia, and Cryoanalgesia
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


