Types of warts
Common term
Specific term
Common warts
Verruca vulgaris
Flat (plane) warts
Verruca plana
Filiform warts
Periungual warts
Plantar warts
Verruca plantaris
Butcher’s warts
Kissing warts
Mosaic plantar warts
Anogenital warts
Condyloma acuminata
Table 9.2
The most common subtypes of HPV causing warts
HPV subtypes causing warts | |
|---|---|
Wart type | HPV subtype |
Common | 1,2,4,57 |
Plantar | 1,2,4,57 |
Mosaic | 2 |
Plane | 3,10 |
Oral | 6,11,32 |
Anogenital | 6,11,16,18,31,33,35,55,56,58 |
Table 9.3
How to differentiate a plantar wart from a corn
Plantar wart | Corn |
|---|---|
On any part of the sole of the foot | Over pressure points |
Thrombosed capillaries | No vascular structures |
More tender when squeezed | More tender when pressed |
Well demarcated (white ring) | Poorly demarcated |
More common in young people | More common in those >50 years old |

Fig. 9.1
A “warty”-looking growth on a 56-year-old woman’s hand that was a squamous cell carcinoma in situ
Apart from anogenital warts, which are a risk factor for cervical cancer, most warts are harmless and 60 % clear spontaneously within 2 years without any treatment, especially in children and immunocompetent adults [1]. However, sometimes warts can continue to grow and spread to other parts of the body. The most common indication to treat warts is for cosmetic or comfort reasons. Warts in children are probably best left untreated unless they are particularly unsightly (i.e. warts on the face) or pain (i.e. large plantar warts). Doctors often underestimate the amount of embarrassment patients suffer with their warts, especially if they are on exposed areas (hands or face) (Fig. 9.2) and/or the patient is working with the public or is a food handler. There are many unanswered questions about the simple common wart. Why do some people appear to be immune, while other apparently healthy individuals can be plagued by persistent and recurrent warts?

Fig. 9.2
Multiple hand warts
Patients with a depressed immune system (poorly controlled diabetes, HIV, chemotherapy, lymphoma, transplant patients) are more vulnerable to warts, find it more difficult to clear them and often relapse after treatment (Fig. 9.3). In older patients, particularly if they are immunosuppressed, such as transplant patients, the wart virus may have oncogenic potential and can predispose to skin cancer such as squamous cell carcinomas.

Fig. 9.3
Warts in an immunosuppressed patient
Research into warts and their treatment are scanty and most of what is published is of poor quality and design. A recent Cochrane systemic review of 60 trials on warts showed that 46 (77 %) were classified as low quality, heterogeneity between trials was high and analysis was often inappropriate or misleading [2]. Comparison of different treatments is often difficult to assess, as the exact techniques used for treatment of the warts is not always described.
9.2 Nonsurgical Treatment
The decision to treat warts has to be made on a case-by-case basis according to the experience of the doctor, patient’s preference and the application of evidence-based medicine (Table 9.4). If warts have to be treated (for pain or cosmetic concerns), the first line of treatment is usually with topical treatments with salicylic acid or a traditional cure. Traditional cures probably get their reputation by the fact that most warts will regress and clear spontaneously within time. A placebo has a 27 % success rate [2]. However, one should never underestimate the power of persuasion, wishful thinking and the ability of mind to cure the body.
Table 9.4
Most common treatment modalities used for the treatment of warts
No treatment |
Traditional cure/placebo |
Topical salicylic acid |
Topical glutaraldehyde |
Cryosurgery |
5 % imiquimod |
Topical podophyllotoxin |
3 % formalin soaks |
Monochloroacetic acid crystals embedded in 50 % salicylic acid |
Pulse dye laser |
Photo dynamic therapy |
Curettage and cautery |
Systemic retinoids |
Intralesional bleomycin |
Intralesional interferon |
Intralesional immunotherapy |
There are many over-the-counter topical agents used to treat warts in children and adults. Some of these are keratolytic such as salicylic acid which has a cure rate of up to 75 % if used daily for 12 weeks [3]. Others are verucidal such as glutaraldehyde. There is very little evidence to recommend one over the other. Success in treatment is often more dependent on the enthusiasm and persistence of the patient or parent. Most will work better if applied after paring down the keratin with an emery board or blade every night before applying the gel and continuing the treatment for at least 6–12 weeks. Most patients and parents give up long before this, unless is it clearly outlined to them how to apply the treatment and how long the treatment will take.
The 3 % formalin soaks daily for 6–12 weeks can sometimes help clear mosaic plantar warts. The plantar wart should be pared down nightly with an emery board or file, and then the wart is soaked in a bowl of formalin or cotton wool soaked in formalin for 10–20 min. The surrounding healthy skin can be protected with Vaseline® if necessary.
Monochloroacetic acid crystals embedded in 50 % salicylic acid cream can be helpful in isolated plantar warts, less than 10 mm, in patients who are not suitable for cryosurgery or other topical agents. The cream and crystals are held in place over the wart using a corn plaster and tape for 3 days. It causes a sterile abscess which lifts the wart from the surrounding skin. The abscess needs to be incised and drained (which can be difficult in children), and the plantar wart can be shelled out leaving a clean ulcer which will usually heal in 2–3 weeks.
Photodynamic therapy (PDT) has been used for treating warts, but it is time consuming and expensive, and results are variable.
Pulse dye lasers can be effective when treating warts that are not too bulky. Removing the thick keratin is important before laser treatment, as the light will not penetrate thick dark keratin. Like cryosurgery, this can be painful and may require local anaesthetic. One of the advantages is that there is little or no swelling or blistering; post laser treatment, bruising can last 1 week. It is thought to work by blocking the small feeding capillaries, thus causing an ischemic necrosis.
Intralesional bleomycin or interferon can be an effective treatment for resistant warts but is again expensive, very painful and only available in some hospital dermatology departments.
Intralesional immunotherapy using various antigens such as the MMR (measles, mumps, rubella) vaccine or candida skin test antigen causes a delayed-type hypersensitivity reaction increasing the ability of the immune system to recognise and clear the HPV. This has an 85 % cure rate [4].
9.3 Cryosurgical Treatment
Some patients (or their parents) with unsightly or painful warts do not want to use a cumbersome, uncomfortable, time-consuming treatment with topical agents such as salicylic acid that may only have a 75 % per cent cure rate after 12 weeks [3]. They will often prefer a 10 s treatment with cryosurgery (with local anaesthetic if necessary) with an over 90 % success rate, and the wound usually heals up in 2–3 weeks without scarring (Fig. 9.4a, b).
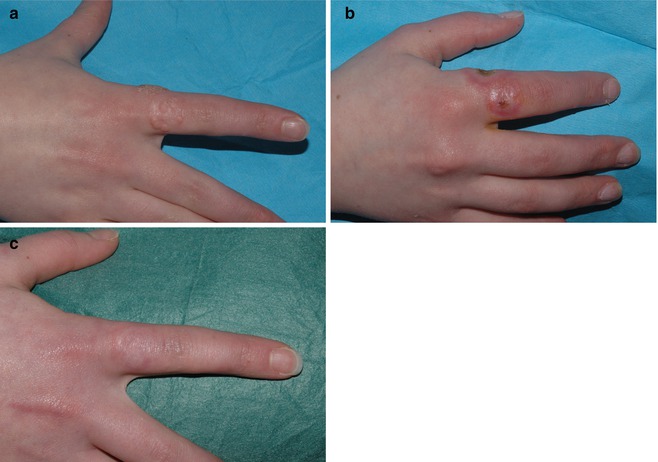
Fig. 9.4
Hand warts (a) before, (b) 1 week and (c) 2 months post cryosurgery
9.3.1 Warts
Cryosurgery is a method of selectively destroying unwanted tissue using cold liquids or gasses. The aim is to cause maximum tissue destruction in the target lesion with minimal collateral damage to the surrounding healthy structures. Cryosurgery does not kill the wart virus; in fact viruses can survive and be preserved in liquid nitrogen. Cryosurgery destroys the cells that are infected with the wart virus by creating intracellular ice crystal formation that ruptures the cell, thus allowing clean, healthy, uninfected cells to take their place. Post cryosurgery, there is a lot of swelling which blocks the small feeding vessels, causing ischaemic necrosis to the frozen area, enhancing cell death. In addition, cryosurgery has the unique action of “cryoimmunostimulation”, whereby some of the wart virus is released from the frozen wart after cryosurgery, presenting the wart to the immune system. This acts like a vaccine, helping the body to fight off the HPV in the treated and sometimes even distant untreated warts. As a personal observation, occasionally patients clear their hand warts spontaneously while being treated for their plantar warts. Patients who have a suppressed immune system are less likely to benefit from “cryoimmunostimulation”. Combining imiquimod (Aldara®) with cryosurgery may enhance this response.
There is only one important rule in cryosurgery: never freeze any lesion unless one is 100 % sure of the diagnosis. If a confident named clinical diagnosis cannot be made do not freeze – take a biopsy or refer the patient for another opinion.
Success in cryosurgery is dependent on four main factors:
Cryogen
Delivery system
Patient selection
Technique
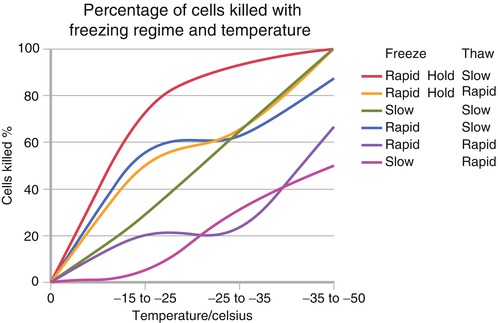
9.3.1.1 Cryogen
Maximum cell destruction is achieved by a rapid freeze, achieving temperatures of less than −40 C at the base of the lesion; a slow thaw; and carrying out at least two freeze-thaw cycles (Fig. 9.5). This can generally only be achieved by using liquid nitrogen which is the coldest (−196 °C), most versatile, cheapest cryogen available (Table 9.5). Over-the-counter cryogens such as home freezers like Wartner®, which contain a mixture of dimethyl ether and propane (DMEP), are much less effective as most only get down to −30 °C at the surface of the wart with a very slow freeze. Handheld medical devices such as the Histofreezer® or the DermaFreeze® also contain DMEP and are equally ineffective and far too expensive per unit cost to make them practical in clinical practice. Most of these devices are limited as they can only apply the cryogen via a bud applicator which is of a predefined shape and size, whereas warts come in all different shapes and sizes. Nitrous oxide gas, while not as cold as liquid nitrogen, can reach −89 °C and can give reasonably good results provided there is meticulous attention to technique.