Fig. 17.1
(a, b) Patient with a morpheaform BCC on the earlobe who did not want surgery. A double freeze-thaw cycle was performed. There has been no recurrence after 3 years
Infiltrating, perineural, perivascular infiltration
Metatypical/keratotic
Ill-defined tumors
Previously irradiated skin
High-risk tumors
Micronodular
For SCC: Poor or undifferentiated, basosquamous
In prior radiated skin
Sarcomatoid
Some criteria are not absolute:
Tumors larger than 2 cm: treatment can be done by segmental or fractional cryosurgery (see Chap. 21).
High-risk areas (Fig. 17.2a, b).
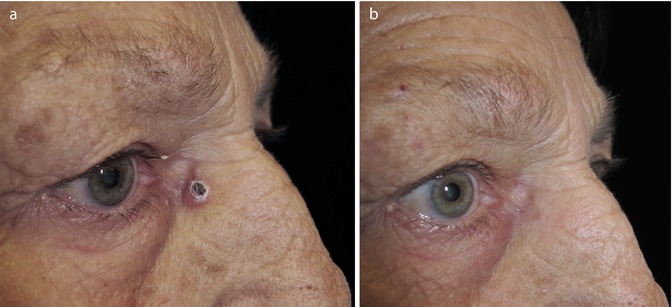
Fig. 17.2
(a) Nodular BCC in the medial canthus. The lesion was treated with two freeze-thaw cycles with a 5 mm flat probe. (b) One year post treatment
Hair-bearing areas: This is not an absolute contraindication if there is no cosmetic concern as to leaving an alopecic scar.
This leaves an immense field of action for cryosurgeons. With proper tumor selection and correct technique, results will be oncologically and cosmetically excellent.
17.2.1.3 What Volume Does the Tumor Have?
Previous knowledge of the tumor volume and shape will help make the best therapeutic decision. There are tumors that have a subepithelial component larger than the surface lesion (iceberg phenomenon). It is of utmost importance to have this knowledge before treating the tumor otherwise there will be a risk of leaving residual cancerous cells. Previous HFUS (high-frequency ultrasound) imaging of the tumor will help rule out admixture tumors. Biopsy is not necessarily capable of making such a distinction because it is dependent on the site where the biopsy has been taken. Recognizing an admixture tumor will help choose the proper technique or combination treatment (i.e., a large superficial basal cell carcinoma with a nodular part can be first treated with topical treatment or other tissue-sparing technique and later be treated for the nodular part).
17.2.2 Patient Selection
17.2.2.1 Is the Patient Willing to Be Treated With Cryosurgery?
Patients must understand what the treatment is about. One simple way is by stating that cryosurgery is a fast and low-risk procedure with a long [10] but minimal postoperative care. Patients and/or caretakers need to know in advance and commit themselves to simple instructions of proper wound caring. Time schedule is important: cryosurgery on a low-risk NMSC can be postponed as required. The anatomical area will determine the time of healing: for the same procedure, the face will heal fast and the legs will heal very slowly.
17.2.2.2 Is the Patient’s Skin Color Adequate for Treatment?
Cryosurgery can be performed in any type of skin. However, skin cancer treatment can leave hypo- or even achromic scars. Therefore, avoid cryosurgery in darker skin types in visible areas like the face.
17.2.2.3 Does the Patient Have Blood-Borne Infections or Debilitating Conditions? Is the Patient of Advanced Age? Does the Patient Have a Fear of Surgical Procedures?
All of these conditions make patients particularly suitable for skin cancer cryosurgery since it is a low-risk procedure that can be performed even on bedridden or wheelchair-bound patients and in a non invasive manner.
17.2.2.4 Multiple Versus Single Lesions
Multiple-lesion patients will benefit from this procedure because numerous lesions can be treated in one session.
17.2.2.5 Anatomical Area
Some areas heal very nicely: nose, earlobes, and eyelids. Others instead may have unaesthetic scars, for example, the middle of the cheek in a young person. Avoid treating malignancies in the legs because the postoperative healing takes very long and the scar can be cosmetically unacceptable. Use cryosurgery in the lower extremities if patients/caretakers are not concerned about time or cosmesis and other options are not available.
17.2.2.6 Damaged Skin
With healing, the new skin is lighter than the surrounding one. In highly dyschromic skin, the cryosurgical scar will stand out, although with time this improves.
17.2.3 Setting
One of the great advantages of cryosurgery is that it does not require special settings in order to be performed. This is a real advantage when dealing with bedridden or wheelchair-bound patients. No strict asepsis is required.
17.2.4 Anesthesia
Freezing skin cancer with double freeze-thaw cycles requires local anesthesia because freezing will be deeper and last longer. Pain is also related are usually better tolerated than in the nose. For patients allergic to anesthetics, cryosurgery can sometimes be their sole option of curative treatment for a skin malignancy. Some patients tolerate the procedure without any local anesthesia.
17.3 Cryosurgical Techniques
17.3.1 One Versus Two Freeze-Thaw Cycles
In skin cancer amenable to cryosurgery, there are some concepts that must be kept in mind.
Cancerous cells are destroyed at approximately −50 ºC. The temperature at the center of the iceball will surely attain values below –50ºC which will cause tumor necrosis. The problem might arise if the freezing front is not allowed to extend so that the appropriate margin also achieves this freezing temperature. For most BCC/SCC, a 4–5 mm margin is mandatory.
Recurrences or incomplete treatment are those that leave viable malignant cells behind, and this happens at the periphery, where temperature has not achieved the required −50 ºC. Therefore, measure the temperature at the periphery of the tumor and not in the center (see Fig. 13.6). The temperature at the periphery will be the same in depth due to the isotherm within this hemispherical ice ball. The lateral ice spread is approximately equal to the depth of freeze [11]. In a study done by our group, we showed that the mean depth of BCC was 1.73 mm by histology and 2.03 by HFUS (high-frequency ultrasound) and the length was 5.39 mm (histology) and 7.59 mm by HFUS [12]. For example, if one treats a BCC of 6 mm with cryosurgery, freezing 4 mm of margin the ice ball will extend 4 mm in depth. This means that one is freezing a safety margin also in depth. This is true as long as (a) the lateral spreading is from the ice ball (from central freezing) and not an artifact of spiral or paintbrushing on the surface and (b) the −50 ºC (killing temperature for cancer cells) is measured at the surface of the lateral spread and not in the center of the lesion.
17.3.2 Technique
Close or probe is the first choice when treating skin cancer. It provides fast freezing that reaches deep into the tissue. Choose a probe that best fits the size of the tumor; when not possible, choose a probe slightly smaller rather than a larger one. This will allow visualization of the lateral extension of the ice ball and avoids overtreating.
Probes need to be placed over surfaces as flat as possible. Irregular surfaces will have “air pockets” separating the tumor from the probe (interphase) that act as insulators. In addition, irregular tumor surfaces many times are caused by excess keratin (mostly seen in squamous cell carcinomas) which is a very bad conductant. Therefore, when probes are to be used, they will require a flat surface to which they can be applied. Finally, some tumors are in areas not easily accessible and a probe cannot be applied to the surface.
As far as the tumor surface is concerned, superficial BCC and some small nodular BCC usually do not pose a problem. For larger lesions, the surface should be flattened down by curettage or simply choose spraying or cryochambers. If curettage has been performed, make sure to leave a blood-free surface before freezing (blood can raise the local temperature) either by using hemostatic solutions or by electrocoagulation (Fig. 17.3a–e). Curetting the tumor down thoroughly and then applying one freeze-thaw cycle has been proposed with excellent results [15]. Remember that if probes have been used on a curette area, it will need to be sterilized (before and after the procedure).

Fig. 17.3
(a) Keratoacanthoma of the dorsum of the left hand. After local anesthesia, spray freezing to the surface of the skin, and shaving. Hemostatic solution was applied. (b) A double freeze-thaw cycle with flat 1 cm probe (c) applied with some pressure until the probe felt fixed to the skin. (d) One month after treatment; (e) 2 months later
After completing a freeze-thaw cycle, probes occasionally get stuck to the surface even if Teflon covered. Do not attempt a forceful detachment because tissue will tear apart. Just allow thawing and gently detach.
When treating tumors on nasal ala, earlobes, or lips, use your finger beneath the tumor to give further support to the probe and to allow you to feel the advance of the freezing front (Fig. 17.4). Once you feel a cold sensation on your fingertip, stop freezing. In earlobes, it is also possible to see the ice “tattoo” (Fig. 17.5).


Fig. 17.4
Close (probe) cryosurgery on a nasal ala. Freezing front is palpated at the tip with the left index finger located inside the nostril
Fig. 17.5
Ice ball tattoo
After completion of the procedure and before covering the lesion, make sure that there has been total thawing and no bleeding is present. With thawing, there is an immediate vasodilation, and covering the lesion without having made sure that there is no bleeding can result in the patient rushing back in later for a wound dressing change.
If the lesion has been curetted, remind the patient that the bullae can have a bloody content.
Open or spray technique is a good option for large tumors for which correct size probes are not available (Fig. 17.6a–c) and for irregular surface tumors for which no curettage is possible or desired. For very large lesions (superficial BCC), it is best to treat by segments (Chap. 21) to avoid a greater depth destruction. For superficial BCC in the truncal area, one freeze-thaw cycle can be sufficient as long as there is certainty that the entire lesion is superficial. Caution should be taken with clinically superficial tumors that in reality are admixture tumors (approximately 30 %) and are the cause of incorrect treatment or technique selection (see Chap. 13 on BCC and high-frequency ultrasound).
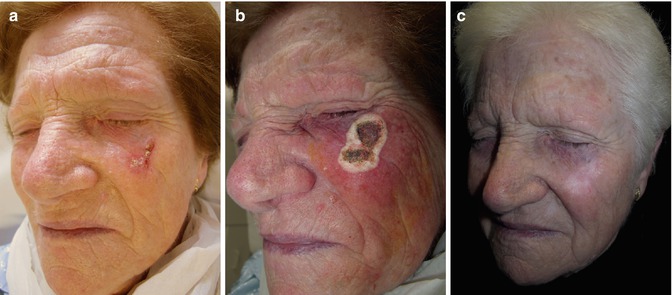
Fig. 17.6
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Role of Reflectance Confocal Microscopy in Cryosurgery
Role of Reflectance Confocal Microscopy in Cryosurgery
 Theoretical Principles of Immunocryosurgery
Theoretical Principles of Immunocryosurgery
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions




(a) Large admixture BCC (superficial and nodular) in the left cheek. (b) Two double freeze-thaw cycles with open (spray) technique; (c) almost 3 years post cryosurgery
Related posts:
Preoperative Care for Cryosurgery
Role of Reflectance Confocal Microscopy in Cryosurgery
Theoretical Principles of Immunocryosurgery
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
Cryosurgery for Warts
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
