Fig. 23.1
Freeze the hose before the procedure or grab it in your hands until frozen in order to avoid freezing the patient or nearby personnel
23.2.2 Edema as Complication
Edema following cryosurgery is en expected event. There are several factors relevant to predicting its severity: (1) individual susceptibility, (2) age, (3) anatomical location, and (4) skin type. Special care should be taken in certain areas. One example is the penile foreskin: if there is a need to treat multiple lesions (i.e., condyloma) or one large plaque (i.e., Bowen’s disease), it should be done by sectors, one side at a time, to avoid severe edema that might cause paraphimosis in uncircumcised males. This iatrogenic entrapment of the penis can become a urological emergency. To avoid this potential complication, it is best to plan the procedure in several sessions.
Care should also be taken to remove rings (like wedding rings) if treating lesions in fingers (like warts or myxoid cysts). The presence of the ring can cause a tourniquet effect when the finger becomes edematous after a cryosurgical procedure on a finger (Fig. 23.2). Post-cryosurgical edema responds very little to steroid medication; therefore, precautions should be taken in advance.

Fig. 23.2
Remove rings before freezing to avoid tourniquet effect
23.2.3 Bleeding
In deep freezing or in previously curetted areas, bleeding can be a possible complication. Sometimes it can be a consequence of an underlying medical condition [6]. Once a lesion is curetted or shaved (for skin biopsy), small vessels are exposed. Topical hemostatic treatments are mandatory before freezing to avoid blood splashing (if spraying technique is going to be used) or blood contact with the probe and eventual sticking to the surface. Even when these precautions are taken, vessels dilate with thawing and occasionally bleed profusely immediately after complete thawing. One common mistake is to cover the treated area when it is still frozen and send the patient home without checking on possible post-thawing bleeding. It is thus essential that proper hemostasis be performed.
In deep freezing such as in skin cancers or vascular tumors, thick scabs can form which occasionally maintain small vessels from bleeding. Once removed (either intentionally or by accident), these vessels can start bleeding. In most cases, this bleeding is superficial and easily controlled just by pressing with gauze over the area; however, occasional profuse bleeding occurs. This is the reason why crust removal should be avoided on vascular tumors. For other lesions, it should be performed by someone with experience and the capacity to stop an eventual bleed. Hemostatic solution can suffice but occasionally electrocoagulation or even ligation of the vessel with a suture is required.
23.2.4 Pain and Syncope
Cryosurgery can cause pain. The degree of pain will depend on personal sensitivity to cold, personal pain threshold, skin type, depth of freezing, and previous pain experiences. Superficial freezing is anesthetic; as freezing continues, so does discomfort and eventually pain. During thawing pain is usually more intense than during freezing due to edema on nerve endings. This delay in the pain sensation has to be kept in mind in order to avoid having the patient leave the office before it commences; otherwise, there is a risk of feeling an unexpected (for the patient) pain sensation and the risk of syncope.
Syncope is not an exclusive event of a cryosurgical procedure: in fact, it can occur in certain patients who move too quickly from lying to standing position, particularly if he/she has been tense during the lying position. This can be avoided by changing position very slowly and allowing a few minutes between lying, sitting, and standing.
Pain sensation of cryosurgical procedures in the temple, parietal, or even frontal regions can cause headaches that last from minutes to hours and can be intense particularly in deep freezing.
23.2.5 Insufflation of Subcutaneous Tissue
A previous curettage or draining of a cystic lesion can leave an opening in the skin and exposure of subcutaneous tissue. If an open cryosurgery is performed, LN can be insufflating inside the tissue. Crepitance can be felt (heard and/or palpated). It is usually not painful nor poses any danger to the patient. It reabsorbs spontaneously. To avoid it, either probe freeze or restrain the LN with a firmly placed cone.
23.2.6 Permanent Changes in Pigmentation
Depending on the skin type and the anatomical area and the depth of the procedure, cryosurgery can leave transient or permanent discoloration of the skin. Hypopigmentation is the most common color change and it is usually temporal. However, hypopigmentation can be permanent, especially when treating skin cancers or in superficial freezing in sun-exposed areas (Fig. 23.3). The latter occurs because skin reepithelialization occurs with preservation of the original skin color which contrasts with the pigmented sun-damaged skin, which is usually discolored. The newly regenerated skin looks hypopigmented in comparison to the surrounding skin. This should be explained previously to the patient in order to avoid false expectations. Hypopigmentation can occasionally repigment in the center (Fig. 23.4) and gradually extend toward the periphery. In skin types 3 or more, light freezing can be the cause of hyperpigmentation which occasionally improves with time (Fig. 23.5). For cosmetic procedures (like in lentigines), treat a hidden area first and wait a few weeks to see the result before attempting to treat large areas. Treatment of skin cancer in very visible areas (like the nose) should be avoided in darker skin types.



Fig. 23.3
Hypopigmentation from multiple cryosurgical procedures in a patient with sun damage
Fig. 23.4
Hypopigmentation can occasionally repigment in the center
Fig. 23.5
Hyperpigmentation at the periphery of lesions (seborrheic keratosis) treated with cryosurgery
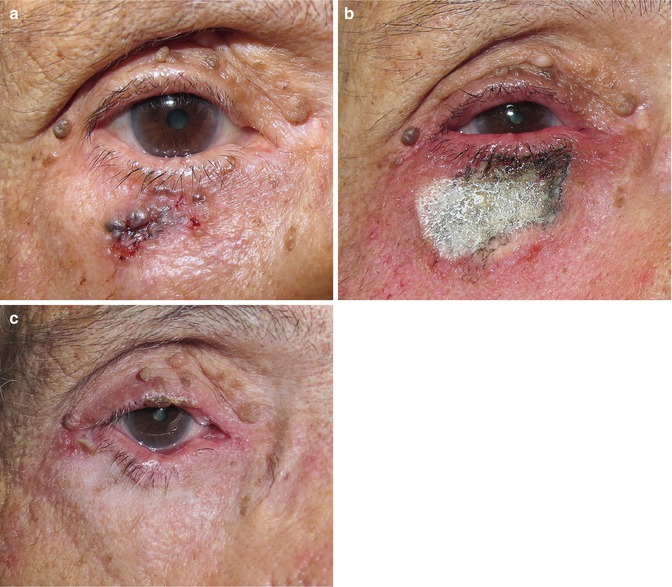
23.2.7 Retraction Caused by Freezing Next to Orifices
Secondary healing in the lower lid (Figs. 23.6a–c and 23.7) or next to the nostrils can cause ectropion or nostril notch. Retraction can improve with time. Whenever a tumor has destroyed part of the tissue matrix, then a nonaesthetic scar is inevitable (Fig. 23.8a, b). A presurgical photograph is of utmost importance as presurgical graphic record of the area; the patient should have realistic expectations of the cosmetic outcome.