Fig. 7.1
(a, b) Cryoshaving of a lesion in the nipple done with cryotweezers. (a) The area was cleaned, and the lesion grabbed with frozen cryotweezers. The freezing front was left to advance just to the surface of the skin. (b) Cutting was performed with scissors right at the base at the beginning of the thawing. The patient felt no discomfort
The use of cold to reduce pain or swelling is called cryotherapy. Instead, when low temperatures induce irreversible damage to a tissue, it is called cryosurgery [2]. In cryobiopsy, the freezing is fast and superficial. No tissue destruction occurs.
Another use of cold as analgesia is spot spraying an area where a needle needs to be introduced. By freezing the surface, the patient will not feel the prick of the needle (Fig. 7.2a, b), therefore reducing discomfort and fear; this procedure is especially useful in children and in delicate areas such as the genitals where a needle prick generates a lot of anxiety.
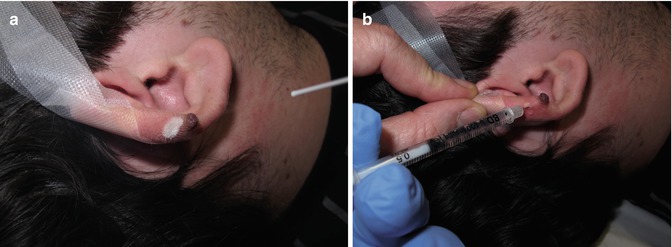
Fig. 7.2
(a) Superficial spray freezing where the needle will prick. (b) Immediate pricking at frozen site
7.2 Histopathologic Evaluation of Cryobiopsy Specimens
The preservation of original components in cells and tissues is necessary for the study and correct interpretation of histopathology changes. Therefore, a correct tissue fixation consists of interrupting degradation processes which appear after cellular death, trying to preserve both tissue structure and composition.
There are two concepts in histopathology that deserve mention: real and equivalent image. A real image of a tissue is the one which shows this tissue when it is still alive. This is an image that cannot be obtained after the fixation process because it is a dynamic feature. On the other hand, an equivalent image is acquired after histopathologic manipulation. This manipulation consists of fixation, inclusion, cutting, and staining. Fixation is the most important step in this complex procedure. As one can see, the main purpose of the histopathologic technique is to strive to have the equivalent image be as similar as possible to the real image.
Fixatives are classified in two distinct groups: (a) fixatives by physical methods and (b) fixatives by chemical methods. In the first case, freezing is employed on a tissue as a method of stopping the autolysis and putrefaction.
In general, when temperature decreases too much, intracellular and extracellular water is crystallized. The key of a successful fixation by tissue freezing lies in freezing and taking the sample as quick as possible. All physiological processes are immobilized in the ice crystals by the quick-freezing methods, and every component of the cells and tissues are maintained in situ at the time of freezing. Thus, ischemic or anoxic effects are minimized [3].
When the tissue specimens are frozen for an extended period of time, the ice microcrystals enlarge, puncturing the membranes of the cells and cellular organelles and causing histopathologic changes. Unlike slow freezing of fixed tissue which affects specimens frozen, for instance, on a cold winter day [4], the rapid freezing of tissue to a temperature below −15 ºC in cryoanesthesia is associated with the uniform production of ice microcrystals within the tissues of the cells and within the extracellular space. When the frozen tissue is thawed slowly, the formation of large vacuoles and circular structures represents artifact vacuolization from nuclear retraction and presence of ice microcrystals secondary to inadequate fixation in formalin [5].
However, the quick freezing of tissue followed by correct fixation in formalin prevents the accumulation of large ice crystals and membrane micropuncture, reducing morphological artifacts and thus avoiding visible tissue defects through the light microscope [6] (Fig. 7.3a, b).
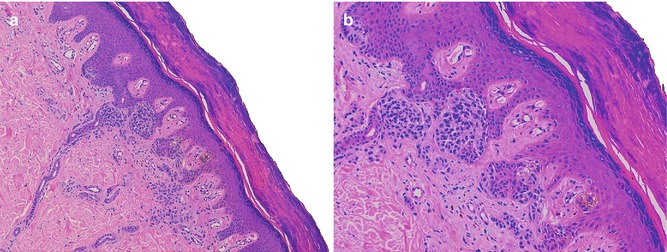
Fig. 7.3
(a, b) Cryobiopsy. Compound melanocytic nevi. Absence of the artifactual changes. Hematoxylin-eosin stained. Original magnification: 1: 100×; 2: 200×
Current studies have also demonstrated that the stability of human epidermal cells to low temperature relates to their stage of differentiation. The epidermal stem cells and transitory cells are more stable than differentiated cells [7].
Our experience is based on the study of 20 cases corresponding to actinic keratosis, melanocytic nevi, basal cell carcinomas, squamous carcinomas, seborrheic keratosis, and pyogenic granulomas. In all of them, the cryobiopsy technique was correctly performed by the same operator with immediate formalin fixation. In order to achieve a more objective evaluation, no information was given to the pathologist about the procedure carried out. In all cases, the material was suitable for histology study, the diagnosis was correct, and no artifacts were described. A second pathologist confirmed the absence of artifacts in all the cases (Fig. 7.4).
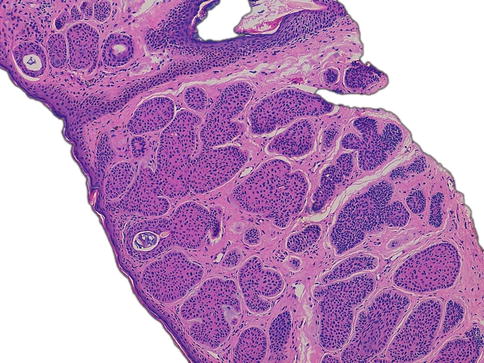
Fig. 7.4
Cryobiopsy. Basal cell carcinoma. Absence of the artifactual changes. Hematoxylin-eosin stained. Original magnification, 100×
The use of cryobiopsy in medicine is not limited to the dermatology field. For example, cryo-needle is used to obtain large histological specimens of high quality from intrathoracic lymph nodes [8].
Related posts:
 Preoperative Care for Cryosurgery
Preoperative Care for Cryosurgery
 Role of Reflectance Confocal Microscopy in Cryosurgery
Role of Reflectance Confocal Microscopy in Cryosurgery
 Theoretical Principles of Immunocryosurgery
Theoretical Principles of Immunocryosurgery
 In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
In Vivo Reflectance Confocal Microscopy Assessment of Wound Induction and Repair of a Skin Injury Produced by Liquid Nitrogen: An Atlas
 Cryosurgery for Warts
Cryosurgery for Warts
 Cryosurgery for Vascular Lesions
Cryosurgery for Vascular Lesions
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


