Fig. 21.1
Oncological and reconstructive criteria for NSM
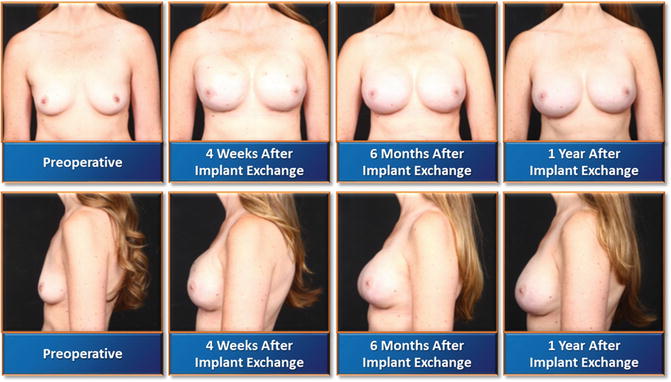
Fig. 21.2
Summary of her mastectomy and reconstruction with 410MF 470 cc silicone implants and fat grafting of the skin envelope with 150 cc of fat on each side
When choosing the incision, the size of the breast and degree of ptosis are the two most important factors. Regardless of the etiology of ptosis, a useful tool for the surgeon is to classify patients by the degree of ptosis present. It is important to clarify with the patient at this time what her goals are in terms of the final appearance of the breast. Regnault’s classification system should be used to grade the extend of ptosis [72, 73]. The amount of preoperative ptosis can be used as a guide to selecting the operation necessary to achieve correction and symmetrization.
The patient in Fig. 21.2 is a good example of an excellent candidate for NSM (Fig. 21.2). On the other hand the patient in Fig. 21.3 is an unclear example for NSM until the nipple to IMF is measured which in her case was 11 cm and therefore she was a reconstructive candidate for NSM (Fig. 21.3). Lastly, the patient in Fig. 21.4 with given asymmetry is an example of how a carefully selected patient who has asymmetry can achieve symmetry following mastectomy and reconstruction (Fig. 21.4). Her candidacy was determined by the measurement of the larger breast as this will play a major role in achieving symmetry postoperatively. Figure 21.5 demonstrates a patient with prior right BCT for medullary carcinoma and a newly diagnosed left triple negative infiltrating ductal carcinoma (Fig. 21.5) Given the nature of her triple negative disease and close proximity of the mass to the nipple, the left nipple will have to be removed and this is demonstrated in Fig. 21.5 with delayed removal of left nipple and simultaneous grafting from the right nipple. In addition, this patient is an example of whether an implant-based reconstruction should be attempted in a patient with prior radiation following lumpectomy. This discussion is beyond the scope of this chapter but the criteria for successful reconstruction depends on where the lumpectomy scar is located. If her lumpectomy scar is in the upper pole of the breast, as seen in Fig. 21.5, and her skin is not scarred down, then an attempt for implant-based reconstruction can be made. However, if the scar is in the lower pole, where the maximum expansion is going to take place, then an autologous vs. latissimus flap and expander should be considered.

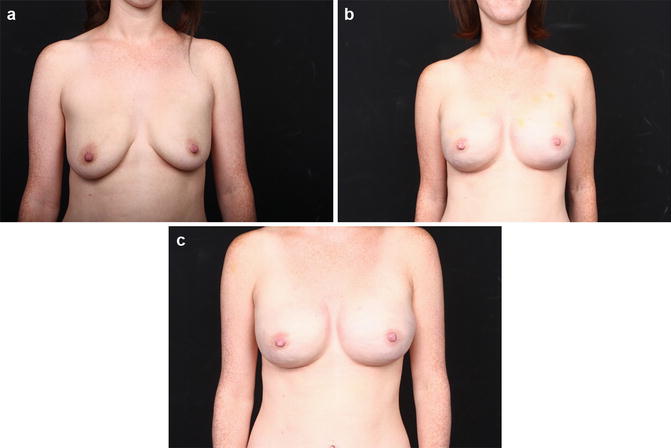
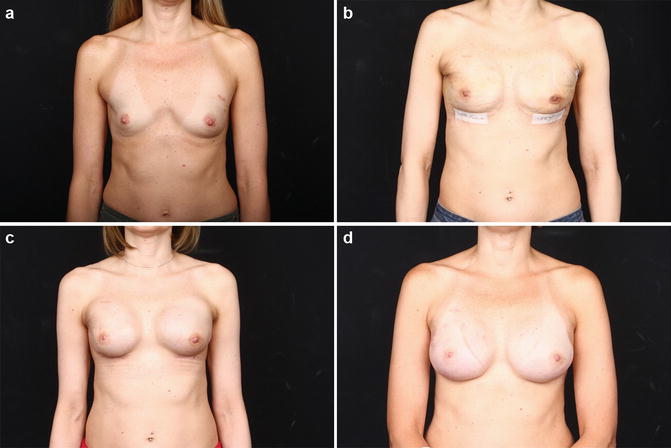
Fig. 21.3
Summary of her mastectomy and reconstruction with 410MF 525 cc silicone implants and fat grafting of the skin envelope with 100 cc of fat on each side
Fig. 21.4
(a) Preoperative patient history patient characteristics : 32 years, 5′4″, 118 lb, BMI: 20.3. Patient history: no prior breast surgery; BRCA+. (b) Three weeks following bilateral breast reconstruction with 410Mx 550 cc silicone implants and fat grafting of the skin envelope with 80 cc of fat on each side. (c) Year following bilateral breast reconstruction with 410Mx 550 cc silicone implants and fat grafting of the skin envelope with 80 cc of fat on each side
Fig. 21.5
(a) Preoperative patient history. Patient characteristics : 48 years, 5′8″, 130 lb, BMI: 20.0. Patient history: preoperative chemotherapy and port placement; prior right BCT for medullary ca of UOQ in 2005; new diagnosis of left invasive ductal carcinoma, stage1A. (b) Two weeks following bilateral nipple sparing mastectomy through IMF incision, with immediate reconstruction with tissue expanders/AlloDerm and injection of Botox. With plan of left nipple removal given the patient has triple negative disease. (c) Four weeks following left nipple removal and nipple grafting from the right side. (d) Year following bilateral breast reconstruction with 410Mx 410 cc silicone implants and fat grafting of the skin envelope with 90 cc of fat on each side
For patients with small and medium sized non-ptotic breasts, an inframammary (IMF) incision can be chosen safely. Lateral mastectomy incisions can also be chosen for NSM, but the risk is that the NAC can be pulled laterally when the scar heals. Surgeons have also used the central vertical incision.
Conclusion
Nipple-sparing mastectomy is evolving and serves as an important option in carefully selected patients. The guidelines stated in this chapter are not intended to replace good clinical judgment but rather to serve as another avenue worth considering. The conscientious preoperative patient selection, multidisciplinary collaboration, pathological analysis of the NAC core, and attention to NSM incision placement is unique for each patient and should be considered carefully.
References
1.
Rankin JS. William Stewart Halsted: a lecture by Dr. Peter D. Olch. Ann Surg. 2006;243(3):418–25.CrossRefPubMedPubMedCentral
2.
Tanis PJ, Nieweg OE, Valdes Olmos RA, Th Rutgers EJ, Kroon BB. History of sentinel node and validation of the technique. Breast Cancer Res. 2001;3(2):109–12.CrossRefPubMedPubMedCentral
3.
4.
5.
Fisher B, Montague E, Redmond C, Deutsch M, Brown GR, Zauber A, et al. Findings from NSABP protocol no. B-04-comparison of radical mastectomy with alternative treatments for primary breast cancer. I. Radiation compliance and its relation to treatment outcome. Cancer. 1980;46(1):1–13.PubMed
6.
7.
Halsted WS. I. The results of radical operations for the cure of carcinoma of the breast. Ann Surg. 1907;46(1):1–19.CrossRefPubMedPubMedCentral
8.
9.
10.
11.
12.
13.
14.
15.
16.
Petit JY, Veronesi U, Orecchia R, Rey P, Didier F, Giraldo A, et al. The nipple-sparing mastectomy: early results of a feasibility study of a new application of perioperative radiotherapy (ELIOT) in the treatment of breast cancer when mastectomy is indicated. Tumori. 2003;89(3):288–91.PubMed
Related posts:
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
 Nipple and Breast Anatomy
Nipple and Breast Anatomy
 Management of Complications Following Nipple-Sparing Mastectomy
Management of Complications Following Nipple-Sparing Mastectomy
 The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
 Techniques to Avoid Nipple and Flap Necrosis
Techniques to Avoid Nipple and Flap Necrosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


