Fig. 10.1
Vascular supply anterior chest wall (a) Perforating vessels off of the internal thoracic artery and usual course of the lateral thoracic artery. (b) MRI showing lateral thoracic artery (LTA) and second intercostal perforator (SIP), invasive ductal carcinoma (IDC). (c) MRI showing internal thoracic artery (ITA), LTA, and nipple-areola complex (NAC). (d) MRI showing periareola anastomosis of the LTA and SIP (arrow)

Fig. 10.2
MRI: internal thoracic perforator running through subcutaneous fat
Palmer and Taylor studied the blood supply to the anterior chest wall using dye injection and radiographs [4]. They agreed that the vascular supply indeed originated from the internal and lateral thoracic arteries. They found that periareola vascularization universally originated from either the internal or lateral thoracic artery. They noted that the internal thoracic dominated in 68 % while the lateral thoracic dominated in 20 %. They found the lateral and internal thoracic providing equal contribution in 12 % of cases. They agreed with other authors that there was usually a dominant perforator originating from the internal thoracic artery and noted that the second intercostal perforator was dominant in 60 % of cases.
Van Deventer noted that the internal thoracic perforating arteries 1–4 contributed blood supply to the NAC. Using latex injections in 27 breasts he noted that the third perforator was dominant in 47.5 % of cases compared to 25 % for the second perforator [3]. Furthermore his findings suggested that the blood supply to the NAC came primarily from the internal thoracic artery and to a lesser extent by the anterior intercostal (24.4 %) and the lateral thoracic artery (23.2 %). Importantly, he noted more inconsistency in the blood supply from the lateral thoracic compared to the internal thoracic .
Our own experience would suggest that the second perforator is dominant in a majority of cases (Fig. 10.3). There are, however, a great deal of inconsistencies in which vessels are dominant and are thereby likely to be most important in supplying the NAC. In Fig. 10.4, there are two dominant perforators, one from the fourth intercostal space, 1 from the second. In this instance the perforator from the fourth space appears to be supplying much of the flow to the NAC. We have also noted that the dominant perforator could in some instances differ from side to side in the same patient. In Fig. 10.5, the dominant perforator on the right side originates from the second intercostal space whereas on the left, from the fourth intercostal space.
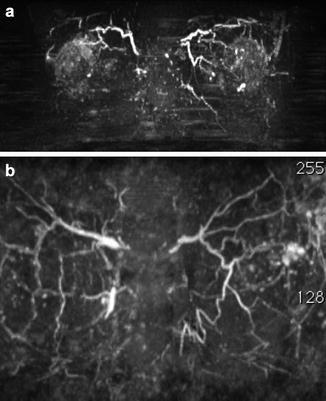
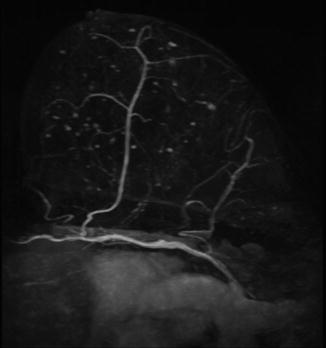
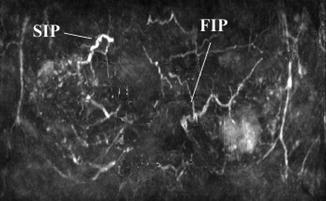
Fig. 10.3
Both (a) and (b) show dominant second intercostal perforators which are commonly the dominate vessels on the anterior chest wall
Fig. 10.4
Two dominate perforators, second and fourth. Fourth appears to be supplying the NAC
Fig. 10.5
Second intercostal perforator is dominant on right, fourth intercostal perforator dominate on left
Incisions
Incisions for nipple sparing mastectomy should meet several criteria. Most importantly, when performed for cancer, the incision should address any cancer-related issues . Commonly, superficial cancers in many instances require removal of overlying skin. Skin excision can frequently be included in the mastectomy incision. In Fig. 10.6a, the cancer is superficial and requires skin excision. Here it is incorporated into a radial incision at the 2:00 position. In Fig. 10.6b, the tumor is at the 6:00 position and can similarly be incorporated into a 6:00 radial incision.
Fig. 10.6
(a) Skin excision incorporated into a lateral mastectomy incision. (b) Skin excision incorporated into a 6:00 vertical incision
Not all cancers are located in positions that can easily be incorporated into standard mastectomy incisions. In Fig. 10.7, the tumor is located in the central upper breast. In this instance if overlying skin excision is required it is suggested that the skin over the tumor be excised through a separate incision and then perform the mastectomy through an incision appropriate for this particular breast type. In this instance a 6:00 radial incision is used to perform the mastectomy.
Fig. 10.7
Tumor location that cannot easily be incorporated into a standard mastectomy incision can be approached by excising skin over the lesion and use a separate incision for the mastectomy
There are other options for dealing with superficial tumors. A small suture can be left in the skin overlying the tumor (Fig. 10.8). The suture is left in place until the final pathology report is available. This allows the breast surgeon to excise the skin or a new margin should the pathology report indicate a close or involved margin. Additionally, one can remove the subcutaneous fibro-fatty layer down to the dermis overlying the tumor, either leaving it attached to the breast specimen or removing it as a separate specimen following mastectomy. Even in these instances one should consider leaving a suture in the overlying skin.
Fig. 10.8
When tumor location is easily determined, a suture is left over the tumor until final pathology report is available. This will allow easy access in case of a positive margin
In patients with cancers lying deeper in the breast parenchyma or in patients undergoing risk reduction mastectomy, considerations change. One cannot overemphasize the need for cooperation with the reconstructive surgeon when planning an incision. Both adequate exposure and a good cosmetic outcome are the hallmarks of a good incision. Equally important, the incision needs to be made in such a way as to preserve blood supply to the skin flap. As noted in a prior section much of the vascular supply to the anterior chest wall comes from medial and lateral as opposed to superior and inferior. There is also abundant experience now to suggest that some incisions carry a higher risk of nipple necrosis than others. Whereas incisions that traverse over a quarter of the diameter of the areola give the surgeon wonderful exposure, they are likely to significantly increase the risk of necrosis [5] (Fig. 10.9).
Fig. 10.9
One hundred and eighty degree periareola incisions traversing over 25 % of the areola margin may increase the risk of NAC necrosis
In a great majority of cases, we use one of two incisions; both are radial in orientation [6]. The first is a lateral incision (Fig. 10.10a). We have found that the lateral incision has the lowest incidence of skin edge necrosis and can be applied to a majority of patients. We use lateral incisions in patients who have little or no ptosis and will not require subsequent mastopexy (Fig. 10.10b). For those just beginning to perform nipple-sparing mastectomy, the lateral incision also provides more familiar exposure. Lateral incisions can also be longer than vertical since they can be extended to the anterior axillary line with little diminution in cosmetic outcome (Fig. 10.11). If needed, lateral incisions can also be extended around the areola but again, not more than 25 % of the circumference.

Fig. 10.10
Radial incisions: (a) lateral incision (b) 6:00 vertical incision
Fig. 10.11
Lateral incision with gluteal artery perforator (GAP) flap reconstruction.
The second most commonly employed incision in our series is a 6:00 vertical incision (Figs. 10.10b and 10.12). In our own series of over 900 nipple-sparing mastectomies, vertical incisions were used in approximately 60 % of cases. We use these incisions in most patients with ptotic breasts as they can easily be incorporated into mastopexy incisions at a later date (Fig. 10.13) [7]. Exposure through this incision is variable and is highly dependent on the distance between the nipple-areola complex and the inframammary fold with longer incisions offering better exposure. In those patients with a very short nipple to inframammary fold distance, exposure can be quite difficult and may require slight variations in the incision. There are several alternatives that can be used to increase exposure. The incision can be extended into the areola ending at the base of the nipple. It may seem counterintuitive, but the cosmetic results can be quite good with this approach (Fig. 10.14). Another option is to utilize a “lazy S” incision (Fig. 10.15). One to two centimeters can offer significant improvements in exposure, particularly when the additional length is near the NAC. Finally in those women with ptosis, a triangular incision at the 6:00 position has the advantage of providing a significant increase in exposure even in patients with a short vertical distance; and also provides some ptosis correction and an excellent cosmetic result (Fig. 10.16).

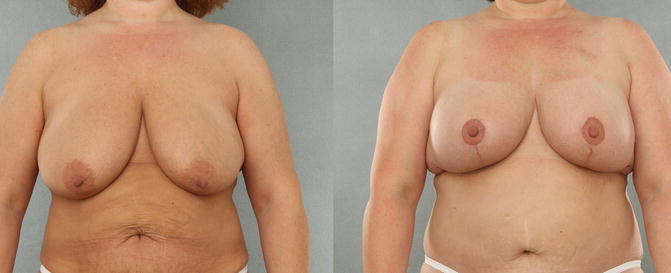

Fig. 10.12
6:00 vertical incision with DIEP flap reconstruction
Fig. 10.13
Patient with grade III ptosis with DIEP reconstruction. Postsurgical mastopexy with improved breast shape and nipple position (From Stolier AJ, Levine EA. Reducing the risk of nipple necrosis: technical observations in 340 nipple-sparing mastectomies. Breast J. 2013 Mar-Apr;19(2):173–9 with permission)
Fig. 10.14
Incision carried through the areola with excellent cosmetic results
Fig. 10.15
Lazy S modification of a 6:00 vertical incision
Fig. 10.16
Triangular modification of a 6:00 vertical incision closes in an L-shape
The third most commonly used incision in our series is an inframammary fold incision [6]. This is clearly the most difficult incision to work through given the longer distance between the upper flap and the inframammary fold. In general, smaller breasts with little ptosis are the most ideal candidates. Also women with wide-based breasts are more suitable than those with narrower teardrop-shaped breasts (Fig. 10.17). With most of the vascular supply to the anterior chest wall coming from medial and lateral, the length of the inframammary fold incision is not critical. It should certainly not extend so medial as to be visible adjacent to the sternum and not so lateral as to interrupt the laterally based blood flow. A well-placed incision can be quite long and provide very good exposure. Despite little interruption in the medial and lateral blood flow to the anterior chest wall, this incision does not offer immunity to skin and nipple necrosis. Using laser Doppler and fluorescein dye Perbeck and Proano evaluated blood flow to mastectomy flaps in 69 patients having either lateral or inframammary fold incisions [8]. They consistently found an area of vascular compromise in an area 2 cm below the NAC in those having an incision in the inframammary fold. This mirrors our own experience with areas of ischemia less likely to develop in the NAC than in the skin just below it.
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
 Nipple and Breast Anatomy
Nipple and Breast Anatomy
 The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
 Management of Complications Following Nipple-Sparing Mastectomy
Management of Complications Following Nipple-Sparing Mastectomy
 Acellular Dermal Matrices: To Use or Not?
Acellular Dermal Matrices: To Use or Not?




Related posts:
Patient Selection and Breast Imaging
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Nipple and Breast Anatomy
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
Management of Complications Following Nipple-Sparing Mastectomy
Acellular Dermal Matrices: To Use or Not?
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
