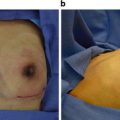
Fig. 12.1
A 42-year-old female with stage 1 right breast cancer who also desired a left prophylactic mastectomy . Preoperative views (a, b, and c) the patient had C-cup-sized breasts without breast ptosis. Postoperative views (d, e, and f) the patient underwent bilateral nipple-sparing mastectomies with prepectoral positioning of a shaped, silicone gel implant (DTI) along with complete implant coverage with ADM. Note, the deficiency of tissue coverage in the upper aspects of the reconstructed breasts. This results from the absence of the pectoralis muscles and is usually treated with autologous fat grafting
Despite the many advantages of prepectoral implant placement, the author still prefers to include the pectoralis muscle in non-NSM implant-based breast reconstruction. However, the author uses complete coverage of the expander or implant with a full sheet of ADM for both NSM and non-NSM. In the circumstance of a non-NSM with a standard mastectomy incision, the pectoralis muscle is positioned overlying the ADM in a vest-over-pants fashion, which allows for the pectoralis muscle to be underlying the mastectomy incision. With an inframammary mastectomy incision, which is preferred with NSM, the pectoralis muscle is not needed for the reconstruction. In this scenario, the prepectoral position is used for the direct insertion of a permanent implant at the time of NSM. However with SSM, utilizing the standard mastectomy incision located on the breast mound, it is essential to position the pectoralis muscle underlying the mastectomy incision. Placement of the pectoralis muscle underlying the standard mastectomy incision is imperative for adequate wound healing. ADM only underlying a standard mastectomy incision leaves the mastectomy incision vulnerable to dehiscence and poor wound healing if it becomes exposed during the healing process.
Although immediate placement of the permanent implant can be less expensive and more convenient, it has some disadvantages when compared with a two-stage approach with placement of the tissue expander at NSM, followed by exchange for a permanent implant, typically 3–6 months later. Other patients who may benefit from a two-staged approach to implant-based breast reconstruction include: patients who may or will receive PMRT, patients with ptotic-shaped breasts (breast ptosis, grade 2 or 3), patients with D-cup-sized breasts or larger who will require a large-sized permanent breast implant (greater than 600 cc), patients with the potential for a close or positive postoperative NAC tumor margin, patients at risk for a nontechnical performed NSM, and those patients who will receive ALND.
A two-staged approach to implant reconstruction with NSM allows for some additional advantages including the ability to fat graft the breast envelope at the second stage (exchange of tissue expander for permanent breast implant). By the time of the second stage, the ADM placed at the first has already integrated into the undersurface of the breast skin envelope. Integration of the ADM into the lower pole breast skin allows for a tissue plane for fat deposition which is not readily available at the time of NSM when a DTI, one-stage approach is used for breast reconstruction .
It is important to understand that a ptotic-shaped, natural-appearing reconstructed breast that is symmetric with the contralateral native breast can be achieved with two-stage breast reconstruction as long as intraoperative saline filling of expanders is performed at the time of insertion. A two-staged approach with NSM also allows for second stage conversion of the reconstruction to a flap if PMRT is found to be required after review of the permanent sections, or to perform so-called, “interval fat grafting ” overlying the tissue expander after PMRT prior to exchange for permanent implant. The author developed interval fat grafting to decrease the risk for implant loss after exchange of a radiated tissue expander for a permanent breast implant. In addition, a two-staged approach to implant reconstruction with NSM, allows for the breast reconstructive surgeon to “wait and see” the reaction of the breast skin envelope to the radiation, and then determine the best definitive method for breast reconstruction (implant, implant and flap, or flap).
Despite some promising studies showing the ADM may reduce capsular contracture in radiated breast reconstructions [5], it is unclear whether it is preferable to radiate the permanent implant or the tissue expander and then exchange for the permanent implant. The author prefers to not radiate the permanent implant, but rather to place a tissue expander with complete ADM coverage and then to radiate the tissue expander . The author then performs interval fat grafting, 3 months after PMRT, and then exchanges for the permanent implant, 3 months after the interval fat grafting procedure. This approach allows for the ADM to fully incorporate into the breast skin prior to permanent implant placement, which may lesson capsular formation and subsequent long-term contracture. This can be especially important in patients who have NSM and will undergo PMRT. Despite the advantages that have been mentioned with a two-stage approach, the risk for infection with 2 separate prosthetic placements is certainly higher, along with a higher associated cost.
With the increasing use of PMRT in conjunction with NSM, it has become critical to understand if ADMs decrease the adverse effects of radiation on implant-based breast reconstruction, specifically, if ADMs decrease the incidence of capsular contracture and the need for reoperation, especially in the setting of PMRT [4]. Early clinical results indicate that ADMs may decrease capsular contracture by decreasing, slowing, or delaying the inflammatory process and pseudocapsule formation around the breast implant [4]. These findings are especially important for patients who have NSM, of which the majority undergo implant-based reconstruction along with an ADM. As more reconstructive breast surgeons gain more clinical experience, the use of NSM in patients that will receive PMRT is becoming only a relative contraindication.
If the assumption is that ADMs decrease capsular contracture, it becomes important to understand how long it takes for the ADM to revascularize into the breast skin envelope. When a permanent implant is placed at NSM along with ADM in patients who will receive PMRT, it is imperative for the surgeon to know if the benefit of the ADM in reducing the inflammatory response and reducing peri-implant capsular formation will be achieved. The timing of delivery of PMRT in relation to the placement of the ADM can vary depending on whether the patient will receive neoadjuvant or adjuvant chemotherapy . It may be that two-stage implant reconstruction, which allows for the permanent implant to be placed after complete integration of the ADM into the skin envelope, especially in the circumstance of neoadjuvant chemotherapy, may offer the greatest benefit. This may be an important consideration in patients who will receive PMRT in whom the risk for capsular contracture is significant.
An important animal study performed a microcirculatory analysis that revealed early ADM angiogenesis at 4 weeks on the breast skin flap surface only, not the tissue expander surface [6] and, a well formed vasculature on both surfaces at 8 weeks. Both surfaces were highly vascularized by 12 weeks. ADM showed complete remodeling and revascularization by 12 weeks after implantation. Therefore, in patients who undergo neoadjuvant chemotherapy , a two-staged implant reconstruction should be considered because the ADM will not be fully integrated into the breast skin prior to PMRT, and the patient may not receive the anti-inflammatory advantages of ADM. In these patients who receive neoadjuvant chemotherapy and subsequent NSM and DTI along with ADM, who then require PMRT, usually 4–6 weeks after surgery, it is unlikely that the ADM will be protective from the adverse effects of radiation on the breast implant. Adjuvant chemotherapy, often administered over a 4- to 6-month period after the surgery, prior to PMRT, should allow adequate time for complete integration of the ADM into the breast skin prior to PMRT. In these patients, the tissue expander is usually exchanged for the permanent breast implant usually 4 months after the completion of PMRT , thereby allowing the patient to potentially benefit from the protective effects of the fully integrated ADM. However, as mentioned above, the author performs an interval fat grafting procedure overlying the radiated tissue expander, and then waits 3 months for the grafted fat and mesenchymal stem cells to lead to neo-angiogenesis and neo-adipogenesis, before exchanging for the permanent breast implant.
Related posts:
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 The Science Behind Fat Grafting and Acellular Dermal Matrices
The Science Behind Fat Grafting and Acellular Dermal Matrices
 The Inframammary Approach to Nipple-Sparing Mastectomy: The UCSF Experience
The Inframammary Approach to Nipple-Sparing Mastectomy: The UCSF Experience
 Management of Complications Following Nipple-Sparing Mastectomy
Management of Complications Following Nipple-Sparing Mastectomy
 The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
 Techniques to Avoid Nipple and Flap Necrosis
Techniques to Avoid Nipple and Flap Necrosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


