Author
Year
N
F/U months
NAC excision (%)
Recurrence
Recurrence in NAC
RR (%)
Kissin
1987
20
1
5
Bishop
1990
24
46.8
45.5
3
12
Gerber
2003
61
59
4
1
1.6
Petit
2005
300
12
2
0
0
Gerber
2009
60
101
7
11.7
Paepke
2009
109
34
12
2
0
1.8
Procedures continued to evolve into total skin-sparing or nipple skin-sparing mastectomy, defined as a mastectomy that removes the breast and nipple–areolar complex while preserving the entire skin envelope of the breast, including the skin overlying the nipple–areolar complex [9]. The glandular tissue beneath the nipple–areolar complex is removed with the mastectomy specimen taking care to leave only the skin of the nipple and areola in place.
The progression of the nipple skin-sparing mastectomy described by Sufi et al. in 2000, and termed the “envelope mastectomy ,” provides the earliest report of nipple skin-sparing or total skin-sparing mastectomy without leaving the nipple–areola complex intact [10]. The original reported incision was a lazy S in the mid axillary line allowing for the mastectomy, nodal clearance, and latissimus dorsi flap all through one incision. Twelve patients were included in the original study with short-term follow-up of 8.5 months in which there were no recurrences and 92 % cosmesis satisfaction score [10].
A similar procedure termed, nipple-sparing mastectomy (NSM) with immediate reconstruction, preferably with a lateral incision, by Crowe et al in 2004, included 54 NSMs on 44 patients [11]. They excluded patients who had undergone neoadjuvant chemotherapy, had inflammatory breast cancer, Paget’s disease of the nipple, patients whose tumor was greater than 3.5 cm, or centrally located tumors. Intraoperative frozen sections of nipple core biopsies were performed with six specimens positive for invasive cancer, all of which were converted to total mastectomies without preservation of the nipple. Of the 48 NSMs completed, three had partial loss of the nipple–areolar complex, all occurring early in the experience, and all three of these had medial incisions. There was no long-term follow-up mentioned [11].
We coined the term total skin-sparing mastectomy (TSSM) in 2005, in our review of 50 TSSMs performed on 31 patients. An inframammary incision was preferred centered at the mid-clavicular line. Six of the 50 TSSMs required resection of the nipple–areola skin, four due to tumor involvement and two due to skin necrosis. The average cosmetic score was 8.5 on a scale of 1–10 and there were no recurrences after a mean follow-up of 7.9 ± 5.4 months [9].
In addition to oncologic safety of saving the nipple, patients reported improved satisfaction, body image, and psychological adjustment when the nipple–areola complex was preserved during mastectomy [12,13].
A systematic review of total skin-sparing mastectomy (TSSM) evaluating oncologic outcomes and postoperative complications was published in 2013 by Piper et al. [14]. The authors performed a Medline and Cochrane database review resulting in 27 papers. Techniques that allowed tissue to remain below the nipple without removal of the nipple–areola complex were excluded. In terms of oncologic outcomes, 159 (6.4 %) of nipple core biopsies sent for frozen section were positive for tumor leading to resection of the nipple–areola complex, and ultimately a skin-sparing mastectomy. To assess local-regional recurrence , 11 papers were included, all having at least 24 month follow-up, totaling 1467 patients. Overall, forty (2.7 %) of these had recurrences. Of the four studies that included > 5 years of follow-up, the recurrence was 24 of 547 (4.4 %). In terms of postoperative complications, 2 % had complete nipple–areola complex loss due to necrosis and 8.8 % had some degree of loss. Mastectomy skin flap loss, either partial or full thickness, was reported as 9.5 % overall. Of the TSSMs, 81 % underwent 2-stage reconstructions with expanders followed by implants with an overall implant loss rate of 3.9 % [14]. This systematic review demonstrates the oncologic safety as well as an acceptable complication rate of the TSSM [14].
Basis for Oncologic Safety
When considering anatomic application to oncologic principle, most breast tumors develop in the terminal ductal lobular units, which is especially relevant in prophylactic mastectomy. Stolier et al. found that 91 % (29 of 32) nipples examined had no terminal ductal lobular units within the nipple papilla. Terminal ductal lobular units were sparse in the three specimens that identified their presence, and all were located at the base of the papilla [15].
A prospective study published by Benediktsson et al. included 216 patients who had either already undergone a partial mastectomy with findings of positive margins or multicentricity, or had features not amenable to partial mastectomy including tumor size >3 cm or multifocal carcinoma [16]. The surgical technique described leaves a 5 mm thick plate of glandular tissue spanning a 2 cm diameter beneath the nipple to preserve nipple–areola blood supply. All patients had intraoperative frozen sections performed requiring 11 removals of the nipple–areola complex for malignancy. This study represents patients with advanced disease undergoing a nipple-sparing technique including lymph node metastasis in 40.3 % with 29 patients having carcinoma in situ, 72 patients with Stage I disease, 82 patients with Stage II disease, and 33 patients with Stage III disease. Median follow-up was 13 years with all patients followed at least 11.6 years or until death. Disease-free survival was 51.3 % and overall survival was 76.4 % with the frequency of locoregional recurrence of 8.5 % among irradiated and 28.4 % among non-irradiated patients (p = 0.025). Patients that were further monitored after locoregional recurrence were found to have 5-year freedom from a second locoregional recurrence or distant metastasis of 60 % and overall survival of 82 % [16]. This prospective data provides a basis for oncologic safety of the TSSM even with inclusion of locally advanced breast cancer patients.
A recently published systematic review from Huang included 42 studies evaluating the oncologic safety of nipple skin-sparing mastectomy in which it is emphasized that there is need for uniform preoperative selection and standardization of both surgical technique as well as pathological examination of nipple-sparing mastectomy specimens [17]. Locoregional recurrence ranged broadly from 0-24 % among studies, but the majority demonstrated no significant difference in local recurrence, distant metastasis, or overall survival between traditional mastectomy and nipple-sparing mastectomy for the treatment of breast cancer. NAC recurrence rates were between 0 and 3.7 %. They were found to have a good prognosis with removal of the NAC with a 93 % disease-free survival rate at 5 years following the NAC recurrence. It was noted that patients with early local recurrence, defined as <3 years after surgery had 68 % overall survival and late local recurrence had 86 % overall survival (p = 0.03). This large review supports the oncologic safety of nipple-sparing mastectomy , even with the inclusion of studies performing subcutaneous mastectomy as a nipple-sparing technique [17].
Indications for TSSM
Initially, indications for TSSM were small tumors, tumors that were not close to the nipple and those that were not multicentric. With increasing data on the oncologic safety of the TSSM, the inclusion criteria for patients offered TSSM has broadened. We now include those with locally advanced breast cancer, those undergoing neoadjuvant treatments, those requiring radiation, and those who are BRCA gene mutation positive.
Absolute contraindications to TSSM are patients with involvement of the skin, involvement of the nipple–areola complex, inflammatory breast cancer, and known smokers. Consideration of breast size and ptosis should also be included in the decision to offer TSSM in relation to cosmesis. Nipple-sparing mastectomy in patients with significantly ptotic breasts may be difficult to reconstruct and may lack cosmetic appeal. There have now been a variety of methods of tissue rearrangement techniques to improve cosmetic appeal of the nipple-sparing mastectomy technique in patients with large or ptotic breasts.
Incision Choice
Blood supply is an important factor in prevention of nipple ischemia and necrosis, and can be interrupted depending on incision choice. The blood supply to the nipple is derived medially from the internal mammary perforators, and superiorly from the thoracoacromial artery, the vessels to the serratus anterior, and the lateral thoracic artery. Laterally, the blood supply originates from the terminal branches of the 3rd-8th intercostal perforators, and the inferior supply arises from branches of the superior epigastric artery. Unnecessary damage to the peripheral blood supply of the breast envelope may occur if the dissection is carried too far beneath the inframammary fold, lateral to the latissimus dorsi muscle, or over the sternum; therefore, these areas should be avoided [18]. Approximately 60 % of the total breast blood supply is from the robust perforators off of the internal mammary artery, which may explain the increased rate of nipple necrosis when using a medial incision [11].
In depth anatomical evaluation of the nipple was performed by Rusby et al. noting that vascular structures were incorporated in the duct bundle of the nipple, but the majority could be salvaged even when taking a nipple core biopsy (Fig. 6.1) [19, 20]. They noted that when leaving a 2 mm rim of nipple tissue after taking the duct bundle, 50 % of vessels were salvaged while removing 96 % complete duct excision. When leaving a 3 mm rim of nipple tissue after taking the duct bundle, 66 % of vessels were preserved while removing 87 % of ductal structures. Similar vessel densities were found in nipples that had been previously irradiated and those that had not been exposed to radiation. The unknown variables remaining are whether or not the vessels within the nipple exposed to irradiation have normal vasodilatory potential in the face of threatening ischemia to the nipple and how much the nipple is affected by venous congestion after a nipple-sparing mastectomy [19].
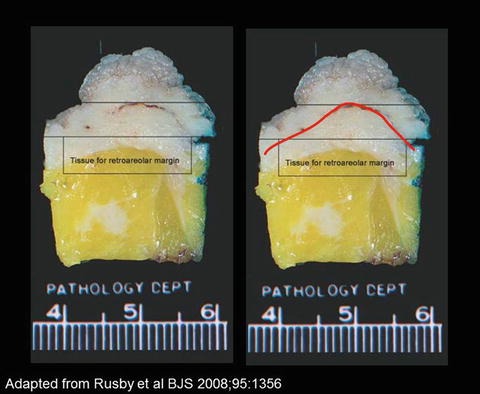
Fig. 6.1
The skin is indicated by the red line (adapted from Rusby), the desired plane of dissection to remove the nipple–areola complex from the nipple–areola
The TSSM can be accomplished through a variety of incisions as we have previously published [21]. Our initial experience with TSSM utilized incision variability, including the inframammary incision, radial and axillary incisions, and incisions through previous scars, but we now find preference in the vertical infra-areolar incision due to consideration of cosmetic result and blood supply to the nipple. A previous incision may be used if adequate exposure is possible to obtain through the same incision. In patients who will require removal of the nipple–areola complex and overlying skin, a lollipop incision with extension towards the inframammary fold was preferred allowing excellent exposure and the best projection for reconstructive purposes. This is true especially for patients with a positive intraoperative nipple core biopsy where the vertical infra-areolar incision can be extended to a lollipop incision to include removal of the involved nipple–areola. An inverted T incision may allow for the best projection of the breasts when encountering patients with pendulous breasts or a significant amount of ptosis.
We have typically avoided the medial incision so as not to disrupt the abundant blood supply to the nipple from the internal mammary perforators as was demonstrated in Crowe’s experience [11]. In addition, reconstruction with implants is extremely difficult through a medial incision. The vertical infra-areolar incision is our incision of choice when possible as it does not disrupt the nipple–areola skin, is well hidden on the underside of the breast, and preserves all vascular flow to the nipple resulting in fewer complications than with our initial cohort where the inframammary incision was used more commonly [21].
Stolier and colleagues reported on 82 nipple-sparing mastectomies with 87 % of those performed through a 6 o’clock radial incision [18]. These authors found the inframammary incision to be problematic for access to the internal mammary vessels for autologous reconstruction and found access to the nipple dissection to be more difficult, which is the critical portion of the case for long term outcomes. However, there were no occurrences of flap loss or of nipple–areola complex necrosis in the entire group, regardless of incision [18].
Technique
Intraoperative subareolar injection of unfiltered technetium-99 m sulfur colloid is performed after induction of anesthesia [23]. Klimberg, Rubio, and colleagues found that subareolar injection is as accurate as peri-tumoral injection in localization of the sentinel lymph node [22]. Subareolar injection also avoids the necessity of image guidance for nonpalpable lesions in order to perform peri-tumoral injection as well as the avoidance of radioactive zone overlap in tumors of the upper outer quadrant of the breast [22]. Our results of 775 intraoperative Tc-99 injections support the subareolar injection as an accurate method for sentinel lymph node biopsy. We were successful with localization of the sentinel lymph node in 98.6 % (419/425) cases of subareolar tracer injected alone, 94.8 % (326/344) of those with dual injection of Tc-99 and Lymphazurin, and 100 % (6/6) in those with a dermal injection [23]. We no longer use blue dye in the breast during TSSM due to previous experience with skin flap necrosis and permanent skin staining at the injection site.
However, we have initiated routine use of axillary reverse mapping (ARM) with injection of blue dye below the subcutaneous tissue of the upper, inner arm volar surface in all patients undergoing sentinel lymph node biopsy or axillary dissection. We do exclude patients with renal insufficiency and those with allergies to various makeup products since there is frequently a similar component of blue dye contained in many cosmetic products. Our most recently reported data evaluated 360 patients who underwent sentinel lymph node biopsy (SLNB) and/or axillary lymph node dissection (ALND) . Crossover occurred in 4 % of patients where the sentinel node was also the blue node, and the remaining 96 % of sentinel nodes were hot, but not blue. Blue lymphatics were visualized in 80 of 237 (33.7 %) SLNB procedures and 93 of 123 (75.4 %) ALND procedures. The lymphedema rate from SLNB with ARM was 1.7 % (4/237) and was 2.4 % (3/123) when using ARM for ALND over an average 12 month follow-up period [24,25]. Regardless of whether one is performing ARM or not, we wish to emphasize that we do not recommend injecting blue dye in the skin of the flap to be preserved as there is an increased necrosis rate at the injection site.
Related posts:
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
 Nipple and Breast Anatomy
Nipple and Breast Anatomy
 The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
 Management of Complications Following Nipple-Sparing Mastectomy
Management of Complications Following Nipple-Sparing Mastectomy
 Techniques to Avoid Nipple and Flap Necrosis
Techniques to Avoid Nipple and Flap Necrosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


