Fig. 18.1
This is a 63 year old female with left sided breast cancer (a). She underwent left nipple sparing mastectomy and direct-to-implant reconstruction (b). Her result is shown 1 year following reconstruction with preservation of nipple shape (c)
Partial nipple necrosis risk has been reported at 1.7 % [3]. The area of involvement can be surgically excised generally with primary closure. Larger nipple-areolar complexes are more forgiving, and results may be improved with delayed tattooing. However, nipple malposition may develop due to scar retraction, and in some cases complete excision with delayed nipple reconstruction may achieve a more predictable result. Total nipple necrosis requiring surgical excision is considered a relatively rare complication, but removal rates as high as 4.3–7.4 % in the postoperative period have been reported [7, 10].
Mastectomy Skin Flap Necrosis
Flap elevation in NSM can be successfully performed with sharp or cautery techniques. Skin flap necrosis after mastectomy can occur due to excessive thinning, retraction injury, and/or thermal injury. Reported prevalence ranges from 3 to 20 % [2, 11]. Potential negative consequences of mastectomy skin flap necrosis include delay for receipt of adjuvant chemotherapy and radiation therapy, as well as device infection, exposure, and/or failure. Earlier publications suggested slightly higher skin flap necrosis rates using NSM compared with skin-sparing mastectomy, though these observations likely reflect technical learning curves [12–14].
Management of skin flap ischemia does not differ drastically after NSM compared with conventional skin-sparing mastectomy. Use of indocyanine green with laser angiography may play a role in guiding intraoperative decision making with regard to mastectomy skin flap viability, but the validity of this technique may be compromised if epinephrine-containing tumescent solution is used to facilitate sharp subcutaneous dissection during NSM. Direct-to-implant reconstruction should only be carried out in the absence of marginal mastectomy skin condition; use of a non- or minimally inflated subpectoral expander will allow for greater flexibility in postoperative management. If concern for skin integrity arises postoperatively, expander deflation to accommodate the loss of skin envelope is often necessary to reduce stress and tension on the overlying skin. The use of topical vasodilators (such as nitroglycerin paste) has been described to improve viability of compromised skin, while antibiotic or antibacterial topicals, such as silvadene cream, are often used during the period of demarcation. Systemic antibiotic use varies widely amongst surgeons in this setting. After allowing for a short period of postoperative demarcation, full-thickness skin loss will require debridement and closure in particular in the setting of implant-based reconstruction. Implication for nipple position after excision of necrotic skin represents a unique challenge. In severe cases, excision of the nipple areolar complex with delayed nipple reconstruction may be a preferable option over attempted correction of subsequent malposition.
Management of mastectomy skin flap necrosis and nipple ischemia has traditionally been based on subjective judgment and clinical experience. The SKIN score system has recently been proposed as an externally-validated tool for assessment of severity and extent of mastectomy skin flap necrosis that is correlated with need for reoperative management. Each breast is assigned a letter grade based on depth of skin necrosis (A, no necrosis; B, cyanosis or erythema of skin suggestive of impaired perfusion or ischemic injury; C, partial thickness necrosis with at least epidermal sloughing; D, definitive full-thickness skin flap necrosis) and a numerical score based on the surface area of involvement (1, no necrosis; 2, 1–10 % of breast or nipple-areolar complex skin; 3, 11–30 % breast or nipple-areolar complex skin, or total nipple involvement; 4, >30 % breast or nipple-areolar complex skin). For NSM, the latter numerical score is separately assigned for nipple-areolar skin; thus, the system can be applied to NSM to grade of nipple ischemia. Composite scores were shown to correlate strongly with need for surgical excision [15]. Although such systems do not eliminate the need for clinical judgment, they provide standardized language for comparison of outcomes and algorithms from which treatment plans may be based (Fig. 18.2).

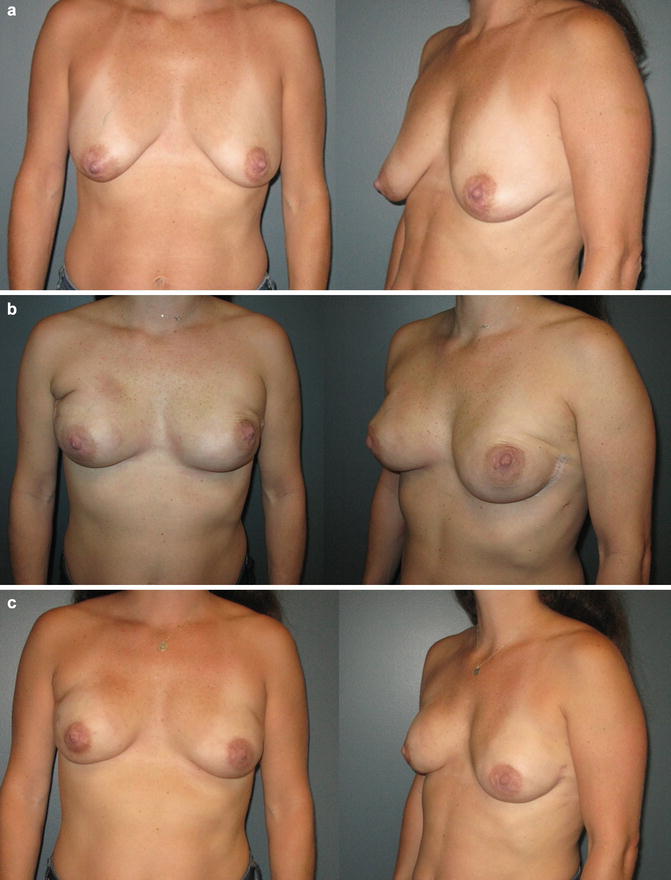
Fig. 18.2
This 45-year-old patient had left-sided breast cancer and underwent bilateral nipple-sparing mastectomies and implant reconstructions. She developed bilateral nipple ischemia and some mastectomy skin ischemia in the early postoperative period. She also likely had a right breast hematoma. This all resolved with local wound care and conservative management. Her result is reasonable symmetry with eventual survival of the nipple-areolar complex
Hematoma/Bleeding
Published prevalence of postoperative bleeding after NSM does not exceed that following skin-sparing mastectomy, but anecdotal evidence suggests that, depending on the incision used, attention to hemostasis in particular areas is critical. For instance, when NSM is carried out via an inframammary fold approach, bleeding can often be encountered in areas of difficult visibility such as the second intercostal internal mammary perforators and the perforating branches toward the clavicular head of the pectoralis major muscle (Fig. 18.3). Hematoma accumulation should be promptly evacuated, as retained blood may facilitate subsequent infectious sequelae and/or capsular contracture. In the authors’ experience, bleeding typically occurs in the subcutaneous plane, and rarely does reoperation require reopening of the subpectoral space. Hemorrhagic complications following NSM are reported to be between 0 and 10 % [3, 4, 8].
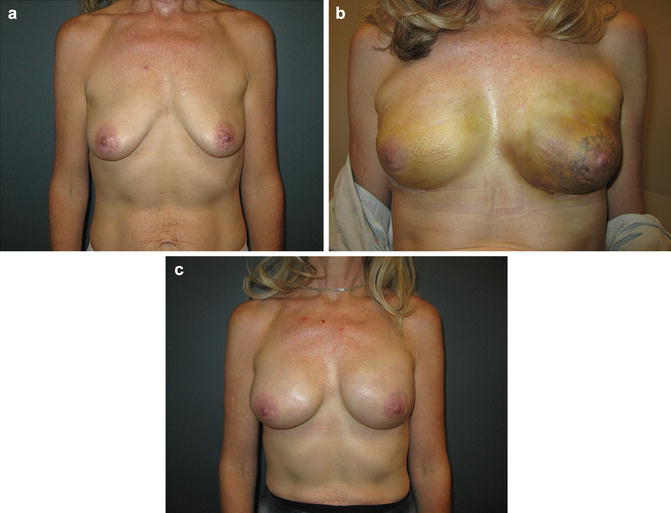
Fig. 18.3
This 36-year-old had a bilateral NSM and implant reconstruction with left breast hematoma. Since it was not expanding and the skin did not feel tight with vascular compromise, a decision was made to watch it conservatively and it resolved with time
Infection
As with skin-sparing mastectomy , surgical site infection threatening reconstructive success, in particular in implant-based reconstruction, remains a point of concern. Even more so than with skin-sparing mastectomy, preferential use of acellular dermal matrix in NSM to allow precise pocket control and implant/expander positioning may contribute to seroma or infectious sequelae, though benefits in lower pole definition, increased initial fill volume, and enhanced device coverage are often thought to outweigh potential downsides. Infection management is not unique to NSM; systemic symptoms and presence of fluid of either serous or purulent quality may dictate clinician judgment with regard to appropriateness of oral or intravenous antibiotic therapy, operative management, and attempted implant replacement or salvage.
Long-Term Complications
Nipple Malposition
In contrast to conventional and skin-sparing mastectomy techniques, immediate reconstruction is a requisite component of successful NSM. Techniques to control nipple position during immediate reconstruction are critical to avoid subsequent malposition, as postoperative malposition is notoriously difficult to correct. Particular attention is needed in cases of higher body mass index, larger breast volume, wider breast base width, ptosis, and anticipated postoperative radiation, as these features may predispose to postoperative nipple malposition. The lateral radial incision may lead to lateral retraction of the nipple long-term. Any native nipple deviation will also be accentuated after mastectomy.
To this end, a number of intraoperative measures have been described. Securing the underside of the nipple to the pectoralis muscle in the desired location with an absorbable suture is feasible, but care must be taken to avoid further compromise of the blood supply to the nipple. Liberal use of suction drains to limit tangential movement of skin over the reconstruction is often preferred. Some surgeons favor use of external fixation devices such as surgical bras or clear occlusive skin dressings to minimize skin displacement. Optimizing expander selection, position, and fill will also facilitate proper nipple position. Maximal initial expander fill without compromise of mastectomy skin flap viability may help preserve satisfactory positioning. If the tissue expander or implant is positioned too medial for example, the nipple-areolar complex relative to the breast footprint will appear too lateral. This is difficult to correct and occasionally requires removal and repositioning of the tissue expander and repeat expansion with the device centered relative to the NAC.
The effort placed into nipple preservation for improved cosmetic outcome is potentially rendered futile if nipple-areolar complex malposition develops, but this adverse outcome is by no means infrequent. The most common displacement patterns are upward vertical malposition and lateral deviation, which have been observed in 69 and 75 %, respectively in smaller series [10]. In Small et al.’s cohort of 319 NSMs, malposition as measured by 1 cm or greater distance between actual and ideal nipple position occurred in 13.8 % of cases. Ideal nipple position was defined as either the point of maximal projection of the implant or the intersection of the mid-clavicular line and the inframammary fold in cases of implant malposition [16].
Once nipple malposition occurs, correction can be quite difficult. The first point of concern should be analysis of implant position and presence of capsular contracture. If implant malposition is due to capsular contracture, pocket revision with capsulotomy and/or capsulectomy should be performed prior to any attempt at nipple repositioning (Fig. 18.4). Inframammary fold elevation and lateral pocket release or capsulorraphy are the most common corrective maneuvers to address needs at post-NSM revision. If feasible, a less projectile or smaller implant may also be more forgiving. Need for nipple repositioning can then be reassessed and performed at the same operation or in a staged fashion.
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
 Nipple and Breast Anatomy
Nipple and Breast Anatomy
 The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
 The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
 Techniques to Avoid Nipple and Flap Necrosis
Techniques to Avoid Nipple and Flap Necrosis




Related posts:
Patient Selection and Breast Imaging
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Nipple and Breast Anatomy
The Inframammary Approach to Nipple-Sparing Mastectomy: The Georgetown University Hospital Experience
The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
Techniques to Avoid Nipple and Flap Necrosis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
