Inframammary incision preferred
Small-/medium-sized breasts
Minimal ptosis
Small NAC diameter
Prior circumareolar incisions
Consideration for other incisions
Moderate/severe ptosis requiring NAC repositioning
High likelihood of post-mastectomy XRT
Special Considerations
Autologous Flap Reconstruction
In our experience performing NSM in conjunction with immediate autologous reconstruction, we have found that peri-areolar incisions can lead to higher rates of nipple necrosis as compared to IMF incisions [4]. Given the compromised esthetic outcomes that can result from NAC necrosis [5], we have developed alternative strategies when performing autologous reconstruction following NSM, including using IMF incisions and performing two-stage reconstruction with initial expander placement.
Prior Breast Surgery (Reduction Mammoplasty/Mastopexy, Lumpectomy)
NSM incision selection in patients with prior breast surgery, particularly those with peri-areolar or circumareolar incisions, can be challenging due to concerns for skin flap and nipple perfusion following mastectomy. However, use of the IMF incision is often a good choice in these patients, as it avoids any further disruption to the dermal blood supply to the NAC. Performing NSM in this population requires careful preservation of the periareolar dermis in order to maximize NAC viability through the subdermal plexus circumferentially supplying the NAC after NSM [6]. Our group and others have found that NSM can be safely performed through IMF incisions following prior breast surgery, with low rates of ischemic complications [7–10].
Anticipated Post-mastectomy Radiation Therapy
In our experience, we have found that use of the IMF incision should be avoided in women with a high likelihood of post-mastectomy radiation therapy due to higher complication rates, particularly wound breakdown and subsequent expander-implant loss [11]. This is likely related to a number of factors. From a mechanical standpoint, incisions along the most dependent portion of the breast are more susceptible to downward pressure from the expander-implant sitting just above the at-risk, irradiated incision. Additionally, when incisional breakdown does occur, expander-implant salvage can be more challenging with IMF incisions, which are directly over the thinnest portion of the pectoralis muscle or the interface between acellular dermal matrix and the chest wall. With periareolar incisions, the expander-implant is well covered by a thick layer of pectoralis muscle just deep to the incision, which likely provides improved expander-implant protection, supporting the higher rates of salvage after incisional breakdown seen in patients with peri-areolar incisions in our practice. Further, with periareolar incisions, it is much easier to close both the capsule and pectoralis muscle, thus leaving well-vascularized tissue beneath the healing TSSM incision , which can help with expander-implant salvage if superficial incisional breakdown does occur.
Technique
Preoperative Markings
Standard preoperative markings for NSM through an IMF incision include the sternal notch, midline, bilateral inframammary folds, and the planned incision (Fig. 5.1). The incision should be made 5–7 mm above the IMF itself in order to be well concealed underneath the breast postoperatively. For adequate exposure, the incision is ideally a minimum of 7 cm in length; as the subsequent scar is hidden from view when looking straight towards the breasts, the longer incision is well accepted by patients postoperatively and helps significantly during the procedure.
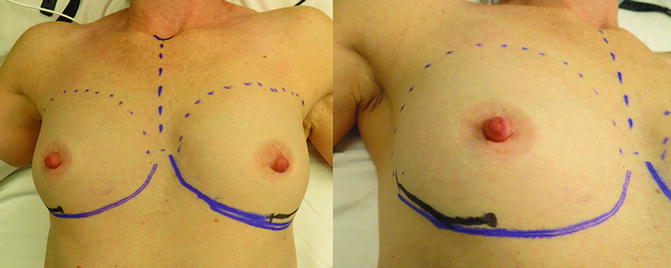
Fig. 5.1
Preoperative markings for NSM via an IMF incision
Operative Technique
Mastectomy skin flaps are created using electrocautery throughout the breast except for underneath the NAC, where sharp dissection is used. Use of lighted retractors is beneficial for adequate exposure, particularly during resection of the axillary tail. Care should be taken when beginning the flap as the surgeon moves in a cranial fashion. This “inferior” portion of the envelope is at the greatest risk for ischemic complications (Fig. 5.2). Starting the flap with adequate retraction is essential for avoiding a “thin” flap. Once the entire breast has been separated from the skin and the tail is removed from the clavipectoral fascia, the breast can be taken off the pectoralis either from cranial to caudal or by starting at the incision and lifting the breast from below (Fig. 5.3). Depending on distance from the incision to the border of the clavicle, sometimes it is easier to elevate the breast from below. Care must be taken to not get between the pectoralis major and minor, but if done properly this method requires less retraction and lifting on the skin envelope for exposure. Following removal of the mastectomy specimen, the specimen is oriented, with care to mark the tissue just deep to the NAC for focused pathological analysis upon permanent sectioning. The mastectomy skin flap is then inverted at the NAC skin and any residual nipple tissue is sharply excised and sent as a separate specimen (Fig. 5.4).

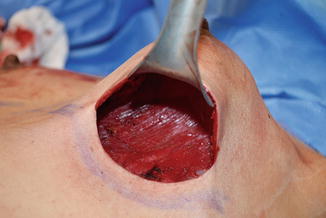
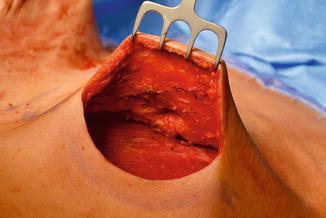
Fig. 5.2
Initiating inferior flap
Fig. 5.3
Removing breast tissue off muscle from an inferior approach
Fig. 5.4
Anterior flap revealing cored out nipple
The vast majority of NSM reconstructions at UCSF are implant-based, with a small number of microsurgical reconstructions performed. Based on our early experience demonstrating high rates of ischemic complications with immediate permanent implant placement [2], all prosthetic reconstructions done after NSM are two-stage procedures. This involves subpectoral placement of a textured, integrated valve tissue expander with detachment of the pectoralis major at its inferior origin and use of an inferolateral sling of acellular dermal matrix to complete the pocket for the expander (Fig. 5.5). One closed-suction drain is placed into the mastectomy space. At the completion of the case, dressings are placed over the breast mound and around the nipple in such a way as to centralize the NAC over the breast skin and minimize subsequent NAC asymmetry or malposition.
 Patient Selection and Breast Imaging
Patient Selection and Breast Imaging
 Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
 Nipple and Breast Anatomy
Nipple and Breast Anatomy
 Management of Complications Following Nipple-Sparing Mastectomy
Management of Complications Following Nipple-Sparing Mastectomy
 The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
 Techniques to Avoid Nipple and Flap Necrosis
Techniques to Avoid Nipple and Flap Necrosis




Related posts:
Patient Selection and Breast Imaging
Plastic Surgery Considerations in Reconstruction After Nipple-Sparing Mastectomy
Nipple and Breast Anatomy
Management of Complications Following Nipple-Sparing Mastectomy
The Vertical Infra-Areolar Approach to Nipple Skin-Sparing or Total Skin-Sparing Mastectomy
Techniques to Avoid Nipple and Flap Necrosis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
