9 The Shave Biopsy
Indications
The following lesions are among those that are frequently diagnosed by shave biopsy:



FIGURE 9-3 A keratoacanthoma on face is appropriate for a shave biopsy.
(Copyright Richard P. Usatine, MD.)
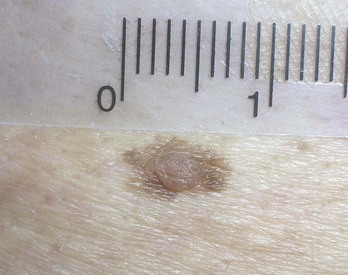
FIGURE 9-4 Dysplastic nevus can be shaved with a deep shave for diagnosis and treatment.
(Copyright Richard P. Usatine, MD.)
Shave excision can also be used to remove the following benign lesions:

FIGURE 9-5 Shave excision of a verrucous-appearing seborrheic keratosis on the forehead.
(Copyright Richard P. Usatine, MD.)

Contraindications
There are no contraindications for shave biopsy based on location of the lesion. The use of a shave biopsy to diagnose a melanoma is controversial with a wide range of opinions. A superficial shave biopsy of a suspected melanoma runs the risk of losing important depth information used for staging and margin determination. However, if the melanoma is thin and the shave biopsy gets below the tumor, then nothing is lost. On the other hand, if a punch biopsy is performed of a large lesion and the punch misses the area with melanoma, this false-negative result can lead to missing the diagnosis of the melanoma. Although doing a complete full-thickness biopsy of a small suspected melanoma is optimal, this may be too deforming for a large superficial pigmented lesion on the face that might possibly be lentigo maligna melanoma (LMM) but appears more consistent with a solar lentigo (Figure 9-7). A broad scoop shave biopsy of LMM (Figure 9-8) may give a better tissue sample than one or more punch biopsies and will not cause the cosmetic deformities of a large full-thickness biopsy. It is also common practice to use a broad scoop shave to remove an atypical mole suspected of being a dysplastic nevus.


Advantages of A Shave Biopsy
The following advantages of a shave biopsy benefit the patient:
A number of studies have shown the shave biopsy to produce a better cosmetic result than the punch biopsy and the fusiform diagnostic excision.1–3
Disadvantages of A Shave Biopsy
For the patient, the disadvantages of shave biopsy include the following:
A superficial shave biopsy should heal with little to no indentation of the skin.4 Deep-shave biopsies are more likely to leave an indentation. Persistence rates of melanocytic lesions for shave biopsy range from approximately 13% to 28%.5 Persistence does not always translate into regrowth. If regrowth does occur, it is important to have access to the original pathology report to avoid overdiagnosing a benign regrowth as a melanoma (pseudomelanoma). Methods useful to differentiate pseudomelanoma from melanoma include accurate clinical records of prior biopsy sites along with evidence of scarring within the current biopsy.5
Equipment
The Personna DermaBlade is an excellent razor blade for shave biopsies. The blue plastic handle makes it easy and safe to grip the sharp razor blade and control the blade for an accurate and precise shave excision. The cost of the disposable DermaBlade is about the same as a standard disposable No. 15 scalpel. Other options include the Personna or Wilkinson double-edge razor blade. The Personna (or Personna Plus with Teflon coating) double-edge blade is very sharp and can be broken in half for easy use (Figure 9-9). Although these do not come in sterile packaging, they can be safely used for shave biopsies without using the autoclave. At approximately 15 cents per cutting blade (30 cents per two-sided blade), these are the most cost-effective tool for shave biopsies. They can be broken in half within their paper container to avoid cutting your hand prior to use. It might take some more time to get used to the bare blade, but once you have mastered its use, you will find this type of low-cost blade to be sharp and effective.

Miltex produces a BiopBlade flexible scalpel for shave biopsies. Its design is similar to that of the DermaBlade, using a single-edge razor blade with a plastic bendable handle. It is currently more expensive than the DermaBlade and has no advantages over the DermaBlade. The plastic handle can snap in half if the blade is bent incorrectly. The Personna single-edge razor blade is too rigid for shave biopsies. All of these blades (Figure 9-10) are available for purchase through Delasco (www.delasco.com) and some can be purchased through other suppliers.

Shave Biopsy: Steps and Principles
Three critical steps in the shave biopsy include:
Preoperative Measures







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


