24 Skin Care Products
Skin care is an essential component of aesthetic medicine. Topical skin care products are used for treatment of photoaging, such as fine lines, rough texture, and dyschromia, and are particularly beneficial in patients with darker Fitzpatrick skin types, where more aggressive treatments may be contraindicated. Visible changes with most topical products are subtle and slow, and typically require regular use over a 3- to 6-month period. Another key role for topical products in aesthetic practice is supporting and enhancing the results of minimally invasive aesthetic procedures. They are used preprocedure to condition and prepare the skin, postprocedure to promote healing and soothe skin, and are helpful in the management of complications.1,2
The three main categories of topical products, based on their regulatory status, are:
Dry Skin (Xerosis)
Xerosis, scaling, winter itch, and flaking are all terms used to describe dry skin. To understand treatment options for dry skin, one must first consider how the skin naturally maintains moisture. Skin is comprised of the epidermis, dermis, and subcutaneous layers (see Figure 19-3 in Chapter 19, Aesthetic Principles and Consultation). The outermost layer of the epidermis, the stratum corneum, forms the epidermal barrier. It functions as an evaporative barrier, maintaining skin hydration and suppleness, and as a protective physical barrier against microbes, trauma, and chemical irritants, and it reduces the harmful effects of ultraviolet (UV) light.3
Photoaged skin has sluggish, disorganized keratinocyte maturation, which leads to corneocyte retention and disruption of the epidermal barrier. Water escapes more freely from the skin causing dehydration and dryness, which can be measured as increased transepidermal water loss.4 Environmental insults such as harsh topical chemicals, temperature and humidity extremes, and genetic abnormalities (e.g., ichthyosis) can also damage the integrity of the skin barrier contributing to dryness.
Treatment of Dry Skin
Moisturizers used to treat dry skin increase hydration by binding and trapping water in the epidermis, and by enhancing epidermal barrier function to reduce evaporative water loss. Skin is rendered more supple and healthy, and clinically demonstrates improvements in smoothness and wrinkles.5 These effects can be temporary, such that once the moisturizer is removed the effects are gone. Effects can also be long-lasting when the integrity of the skin barrier is strengthened following repeated use.
Moisturizers contain three main types of ingredients, each of which serves a unique function6–8:
Most moisturizers are composed of all three ingredient types (occlusives, humectants, and emollients) to create a product that is both effective and cosmetically elegant and does not feel oily to the touch. Although the term emollient is sometimes used interchangeably with moisturizer, it is truly one of three components that can be found in moisturizers. Table 24-1 lists common ingredients found in moisturizers.
TABLE 24-1 Common Moisturizing Agents and Their Function4,12
Moisturizer Types | Functions | Ingredients |
|---|---|---|
| Occlusive | Trap water on the skin surface and enhance lipid component of epidermal barrier. | Oils (petrolatum, mineral oil) Cholesterol, squalene Waxes (beeswax, carnauba wax, liquid wax) Silicones (dimethicone, cyclomethicone) Stearic acid, cetyl alcohol, stearyl alcohol Lanolin, lanolin alcohol |
| Humectant | Attract water from the dermis. | Glycerin Urea Hyaluronic acid Sorbitol Propylene glycol |
| Emollient | Smooth roughened epidermis. | C12-15 alkyl benzoate Cetyl stearate Glyceryl stearate Octyl octanoate Decyl oleate Isostearyl alcohol |
Barrier repair creams are a newer class of moisturizer that contain occlusive and humectant ingredients at ratios that closely mimic the content of normal, healthy stratum corneum: ceramides (50%), fatty acids (30%), and cholesterol (30%). They enhance barrier function, reduce transepidermal water loss, and increase the skin’s resistance to environmental irritants.9 These products may be used by patients with compromised barriers, such as those exposed to cleansers and chemicals, and conditions such as atopic dermatitis. Barrier repair products include nonprescription CeraVe® and TriCeram®, and prescription Mimyx®, Atopiclair®, and EpiCeram®.
Dry skin may also be associated with hyperkeratosis as seen with ichthyosis, keratosis pilaris, and callouses. Topical hydroxy acids such as lactic acid 5% to 12% (e.g., generic ammonium lactate available in the brand names of Lac-Hydrin® and AmLactin®) and urea 10% to 40% (e.g., Carmol® and Vanamide®) are keratolytic and function to reduce stratum corneum thickness and increase hydration.10
Exfoliation treatments, which superficially resurface the skin by removing the topmost layers of the epidermis, can also be used to treat dry skin. Exfoliation stimulates the keratinocyte maturation process with regeneration of a healthier epidermis. This results in a compacted stratum corneum and increased production of ceramides, which improves epidermal barrier function and skin hydration.11,12 Exfoliation, where the outermost layers of skin are removed, can be achieved using mechanical methods (e.g., microdermabrasion) with gentle abrasion, or using chemical methods (e.g., chemical peels) with application of topical products such as acids (see Chapter 23, Microdermabrasion, and Chapter 22, Chemical Peels, respectively).
Photoaging
Most of the changes seen with skin aging are due to years of cumulative UV exposure, referred to as photoaging.13,14 Skin is affected by ultraviolet A radiation (UVA, 320 to 400 nm), long-wavelength solar radiation that penetrates into the dermis, and ultraviolet B (UVB, 290 to 320 nm), shorter wavelength radiation that is absorbed by the epidermis.
Skin Rejuvenation Products
Products used for the treatment of photoaging must address several aspects of the aging process, including increasing skin exfoliation and stimulating epidermal renewal, increasing synthesis of collagen and other dermal matrix components, reducing hyperpigmentation, and increasing hydration. Products used for skin protection are aimed at preventing damage from UV exposure and free-radical oxidation. Skin care regimes usually consist of multiple topical products, including prescription medications and cosmeceuticals, to address these various aspects of skin aging. Table 24-2 lists topical products commonly used for skin rejuvenation and their functions.15
TABLE 24-2 Skin Rejuvenation Products and Their Functions16–19
| CLEANSE | |
| Cleanser selected based on skin oiliness/dryness | |
| TREAT | |
| Textural changes Fines lines Rough skin | Retinoids, hydroxy acids, N-acetyl glucosamine, growth factors, kinetin, peptides, moisturizers |
| Dyschromia Solar lentigines Postinflammatory hyperpigmentation | Retinoids, hydroquinone, kojic acid, azelaic acid, arbutin, and others (Tables 24-3 and 24-4) |
| Vascular ectasias Telangiectasias Rosacea | Bisoprolol, allantoin, aloe, algae extract, borage and evening primrose oil, vitamin C, chamomile, green tea extracts |
| PROTECT | |
| Antioxidants | Vitamin C, vitamin E, ferulic acid, coffee berry, idebenone, gluconolactone, polyhydroxy acids, resveratrol, tea and red wine extracts |
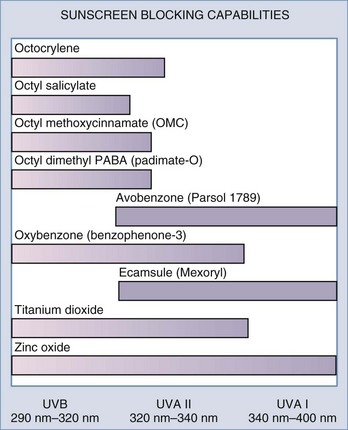
| Sunscreens | Zinc oxide, titanium dioxide, and others (Figure 24-1) |
Prevention of Photoaging
Antioxidants
UV light generates free radicals in skin which oxidize nucleic acids, proteins, and lipids, leading to the development of skin cancers and signs of photoaging.13 The skin protects itself by preventing free-radical damage with endogenous antioxidants consisting primarily of vitamin C in the aqueous compartment, and vitamin E in the lipid compartment such as cell membranes and stratum corneum. Vitamins C and E can be applied topically to enhance antioxidant protection.16,17 These two antioxidants act synergistically. Ferulic acid is another antioxidant that can improve the protective effects of vitamins E and C.17 In addition to antioxidant properties, vitamin C also directly increases collagen synthesis and clinically reduces fine lines.20 The greatest percutaneous absorption of topical vitamin C is obtained with L-ascorbic acid in acidic formulations at pH 3.5 or less, with concentrations of 10% to 20%.17
Sunscreens
Sunscreens protect the skin by reducing UV exposure. There are two main types of sunscreen ingredients each of which has a different mechanism of action. Physical sunscreens, composed of inorganic compounds, reflect and scatter UV light, whereas chemical sunscreens, composed of organic sunscreens, absorb UV light.18 To achieve broad-spectrum UVA and UVB coverage, multiple sunscreens are often combined. Figure 24-1 shows common sunscreen ingredients and their UV blocking capabilities. Certain sunscreen combinations offer greater photostability. For example, avobenzone alone has poor photostability; however, the addition of oxybenzone (HelioPlex®) renders it highly photostable. Sunscreens with broad-spectrum UVA and UVB coverage with an SPF 30 are generally recommended for daily use. Because sunscreens do not block all UV radiation, maximal protection from UV damage is provided by using an antioxidant in addition to a sunscreen.17
 tsp for the face and 1 oz for the body of cream sunscreens.
tsp for the face and 1 oz for the body of cream sunscreens.Treatment of Photoaging
Retinoids
Topical retinoids are used to treat virtually all cosmetic aspects of photoaged skin, including: fine lines, dry and rough skin, hyperpigmentation, as well as acne.19,21,22 Retinoids are vitamin A derivatives, which range from potent prescription products such as tretinoin and synthetic tretinoin derivatives such as tazarotene, to less active cosmeceutical products such as retinol (Figure 24-2). Two topical retinoid products are FDA approved to treat photoaging: Renova® (tretinoin) and Avage® (tazarotene). Several other topical prescription retinoids approved to treat acne are also used off-label to treat photoaging such as Retin-A® (tretinoin), Retin-A® Micro (a less irritating formulation of tretinoin), Differin® (adapalene), and other generic versions of these.
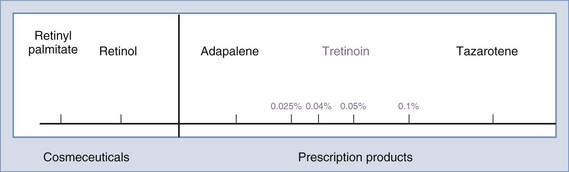
Cosmeceutical retinoids include retinol (vitamin A), retinal (vitamin A aldehyde), and retinol storage forms (retinyl acetate and retinyl palmitate).23 They are less irritating than prescription retinoids and, when used in recommended doses, do not cause a retinoid dermatitis. However, they are much less effective than prescription retinoids in reducing the signs of photoaging.
Matrix Metalloproteinase Inhibitors
Matrix metalloproteinases (MMPs) are naturally occurring enzymes that degrade the skin’s extracellular matrix to facilitate recycling of collagen, elastin, and glycoaminoglycans.24 In young, healthy skin, production of matrix components exceeds destruction caused by MMPs. In photoaged skin, matrix degradation is accelerated because UV light upregulates MMPs. Enhanced matrix degradation combined with age-related decline in collagen synthesis, decreases the structural integrity of the skin’s matrix and contributes to the formation of wrinkles, skin laxity, and telangiectasias.25 Products that inhibit MMPs, such as zinc, calcium, idebenone, and lactobionic acid (polyhydroxy acid) reduce destruction of dermal matrix, increase dermal collagen and elastin, and clinically improve textural changes in photoaged skin.26,27
Human-Derived Growth Factors
Endogenous growth factors are regulatory proteins that initiate wound healing by mediating signaling pathways within and between cells.28 Multiple growth factors migrate to wounds and interact synergistically to promote wound healing and tissue regeneration including synthesis of new dermal matrix components. Topical application of growth factor products, such as Nouricel-MD®, which is derived from human fibroblast cultures, twice daily for 3 months has been shown to improve skin hydration and reduce roughness, hyperpigmentation, and wrinkles in photoaged skin.29,30 Growth factors are large protein molecules and their size may limit penetration through an intact epidermis. Combining them with skin resurfacing procedures that thin or disrupt the skin’s barrier, such as laser resurfacing, chemical peels, and microdermabrasion, or topical exfoliants such as hydroxy acids, may improve penetration of these active proteins.31









