38 Surviving Financially
One important way to survive financially is to be paid appropriately for the procedures performed in the office. Coding and billing for skin procedures can be very complex. It is essential for the practitioner to understand the idiosyncrasies of the ICD-9 and CPT codes if billing is to be completed correctly.1–7 The objective is not to charge as much as possible, but rather, to optimize billing once the proper procedure has been performed. Oftentimes, the same procedure can be billed using three or four different codes. Without exception, one method will pay more. Knowing the proper application of billing rules can, and does, make a significant difference in the financial bottom line of the practice.
Unless a clinician is going to enter into the aesthetic field, the instruments used to perform dermatologic procedures are inexpensive. The most costly would be an electrosurgical unit and a liquid nitrogen gun (see Chapters 14 and 15). On the other hand, aesthetic equipment such as lasers can be very expensive, exceeding $150,000. However, when properly utilized on a frequent basis, lasers will offer the greatest revenue returns compared to other aesthetic procedures that require consumable products, such as botulinum toxin and dermal fillers. Cost versus fee charged for aesthetic laser treatments is more difficult to analyze due to the multiple variables involved such as methodology of acquiring the capital equipment, incidental disposable goods, cost of office space for storing the device, and maintenance contracts ($10,000 per year is common for aesthetic lasers).
A properly designed spreadsheet can be used to estimate whether major investments will provide an adequate financial return. Sales representatives will often paint a rosy picture and provide flow sheets which always conclude that there will be a significant return on investment. Major investments, however, require a careful independent study analysis of main factors.8
The purpose of this chapter is to help the reader become familiar with proper CPT coding for biopsies, destructions, and excisions of skin lesions. It will also help identify the pitfalls and common errors in coding and discuss financial considerations for aesthetic procedures. Tables 38-1 and 38-2 list common coding terminology and modifiers.
| Ablation | See “Destruction” |
| Balance billing | The process of charging a patient the difference between what the physician bills and what the insurance company pays. If a provider participates with an insurance carrier, only copays and deductibles may be charged to the patient. If there is no participation agreement, then the provider may bill the patient for any fees not paid by the insurance company. |
| Biopsy | The procedure used to obtain tissue for histologic examination. This can be done with shave, punch, excision, curettement, and incisional procedures. |
| Electrosurgery/fulgurate/desiccate/cauterize | The use of electrical current heat to treat/destroy an area. |
| CPT | Current Procedural Terminology, published and updated annually by the AMA. Every medical procedure has a CPT code number. The majority of billing is completed using CPT terminology.2 |
| Cryosurgery | The use of low temperatures to destroy (by freezing) a lesion (liquid nitrogen; nitrous oxide closed system; chemical spray canisters). |
| Debridement | Removal of devitalized tissue, dirt, and/or eschar from wounds or infected areas. |
| Destruction | Treatment of a lesion using cryosurgery, chemical application, injection of a chemical, curettement, or electrosurgery. Using a shave technique would also qualify, but in general, reimbursement would be higher using a shave or biopsy code than a destruction code for benign lesions. |
| Explanation of benefits (EOB) | A sheet provided by insurance companies that is enclosed with the payments for various procedures explaining what is allowed, what is the patient’s responsibility (copay, deductible, not covered), what is not allowed (must be “written off” by the provider), and the amount of the enclosed payment. |
| Excision | Removal of a lesion using sharp dissection or electrosurgical cutting. In a shave excision, a slicing technique is used to remove either all or a portion of the lesion. It does not require suturing. Elliptical or fusiform excision includes full-thickness (through the dermis) removal of the lesion and requires closure, usually with sutures (or glue or adhesive strips). |
| Global period | Certain procedures have global periods. During this time, additional services (relating to the original procedure) cannot be charged. For most skin surgical procedures, this period is 10 days (no global period for shaves and punches). |
| ICD-9 (International Classification of Diseases, 9th Revision) | Every diagnosis has a specific numbered code. A diagnostic code is required to justify the reason for a CPT (procedure) code.1 The ICD-10 codes are currently scheduled to be implemented October 1, 2013. |
| Incision and drainage (I&D) | Simple: Contents expressed after incision. |
| Complex: Multiple conditions would qualify for a complex I&D, including the removal of a sac, such as in a sebaceous cyst, or insertion of a drain, such as iodoform gauze. The size and depth of the abscess could also be a factor, as well as excessive time required to complete the procedure. If multiple I&Ds of different lesions are done at the same time, it would also be considered “complex.” | |
| J-codes | Nearly every injectable medication has a specific number assigned to it called the J-code. When administered, the physician charges for not only the administration itself (a CPT code), but also for the particular chemical delivered (identified by the J-code). |
| Modifiers | These are numbers appended to a CPT code while billing to indicate that more than just the usual services were provided for the particular CPT code. (See Table 38-2 for common modifiers). |
| Paring | Removal and/or decrease in the bulk of a lesion, by peeling or shaving it away using a scalpel or a sharp instrument. |
| -25 | Significantly separate E&M on the same day as a procedure. |
| Example: If a patient comes in for a mole removal and you have documentation that you also treated the patient for hypertension, osteoporosis, smoking, etc., use the -25 modifier with the office visit code. | |
| -50 | Bilateral procedures. |
| Example: If you perform sclerotherapy on both legs, you would use the -50 modifier with the sclerotherapy code. | |
| -51 | Multiple procedures. |
| Example: When multiple procedures, other than E&M, are performed at the same session by the same provider, the primary procedure or service may be reported as listed. The additional procedure(s) or service(s) may be identified by appending modifier -51 to the additional procedure or service code(s). Note: This modifier should not be appended to designated “add-on” codes. | |
| -59 | Distinct procedural service. |
| Example: If you performed a cyst excision and decided to also freeze some actinic keratoses, use the -59 modifier with the cryosurgery because it is a completely separate procedure from the excision. | |
| -79 | Unrelated procedure or service by the same physician during a postop period. |
| Example: If a patient comes in to have sutures removed during the postop period, and you perform cryosurgery on some actinic keratoses at the same visit when the sutures are removed, then -79 is used to clarify a separate procedure during a postop period. |
Essentials for Proper Coding and Billing
To code and bill properly, the following information is necessary:
ICD-9 Coding
The majority of dermatologic procedures will involve an abnormal lesion. The diagnostic code (ICD-9) will vary depending on the location on the body and whether it is malignant (primary, secondary, or carcinoma in situ), benign, of uncertain behavior, or unspecified behavior (see Table 38-3). Specific conditions will have separate codes: abscesses, foreign bodies, cysts, etc.
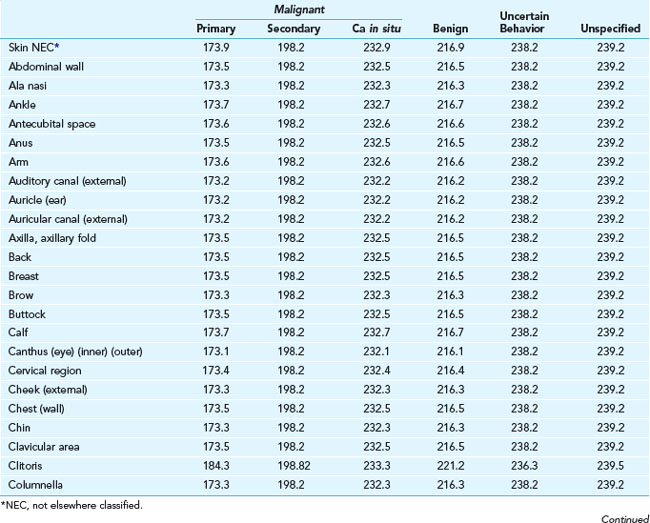
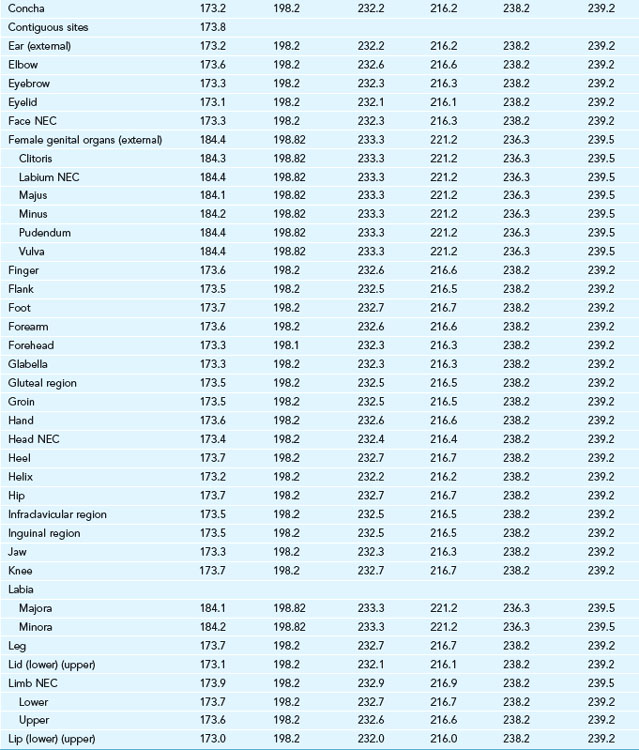
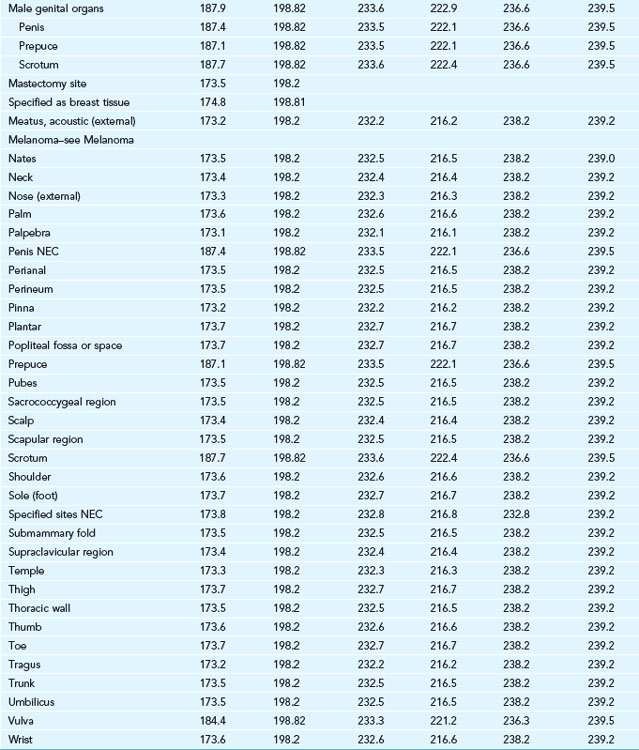
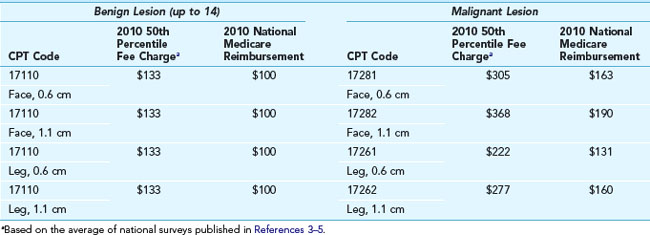
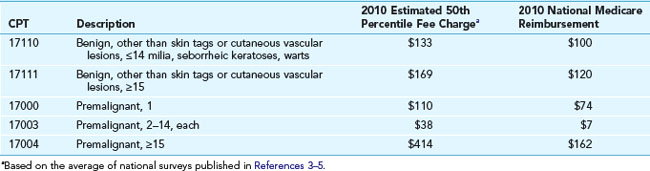
When the diagnosis is uncertain, several options are available. One can use the “uncertain behavior” code if the procedure is a biopsy. If a definitive treatment is performed, it sometimes helps to wait for the pathology to return before completing the billing process. It is best not to use the “unspecified” code because, for whatever reason, many insurance plans will reject that code. If a biopsy was performed, the reimbursement will be the same whether it is coded as “benign” or “malignant.” It makes little difference if the code is correct when only a biopsy was done. However, it is extremely important to know if the lesion was benign or malignant if a treatment is carried out. Note the differences in Table 38-4 for the 50th percentile charges and reimbursement for benign and malignant lesions. These lesions could have been treated with liquid nitrogen cryosurgery, electrosurgery, laser ablation, or other methods. The same time may have been required whether the lesion was benign or malignant, but the fees charged and eventually reimbursed vary markedly.
TABLE 38-4 50th Percentile Charges (National) for Destruction of Selected Skin Lesions and the Average Medicare Reimbursement (2010)
There is no specific code for premalignant lesions, such as actinic keratoses, on a particular body part. They can all be coded as 702.0 (actinic keratosis), regardless of location. However, reimbursement is higher for destruction of multiple premalignant lesions because each lesion (e.g., actinic keratosis) is charged individually (see Table 38-5).
The Importance of Size
Lesion size can be a major determinant in reimbursement. For some codes such as destruction for benign or premalignant lesions, size does not make a difference. However, if the lesion is malignant, the reimbursement varies widely (see Table 38-4). Similarly, size is very important in the repair of lacerations. For all excisions, size is best determined prior to the injection of any anesthetic.
The Importance of Location
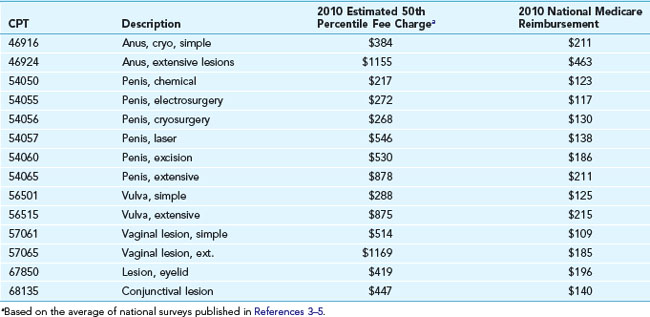
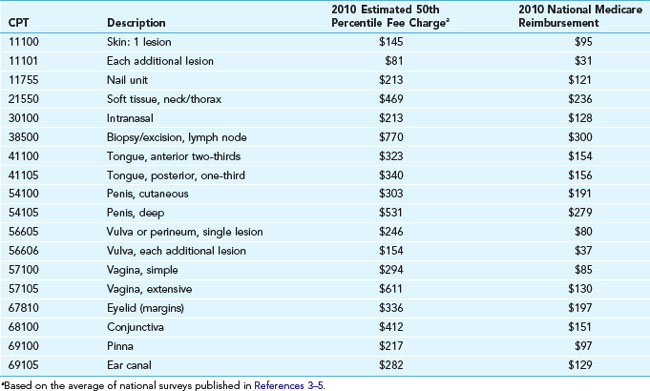
It is critical to know that the same procedure performed on different anatomic locations is reimbursed differently. Even for benign destructions, where size and location usually does not matter, there are some exceptions. For instance, treatment of benign lesions of the penis, vulva, vagina, perineum, anus, and the eyelids all have distinct CPT codes (see Table 38-6). Biopsy codes are also specific for similar sensitive areas (see Table 38-7).
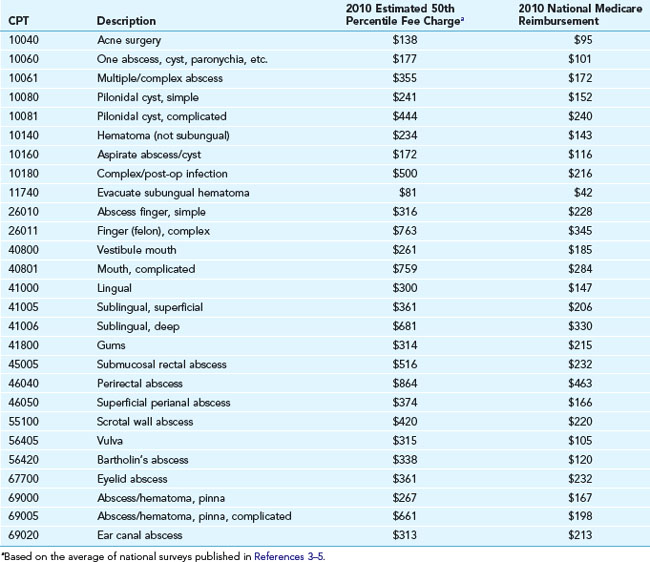
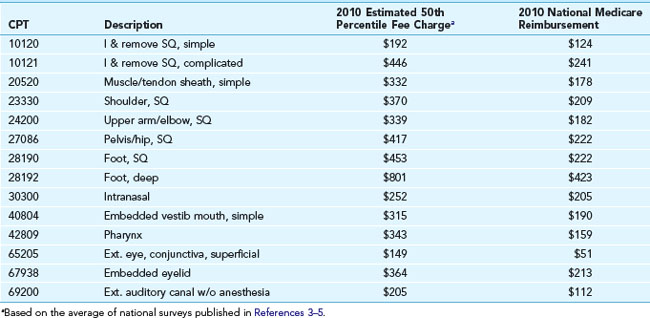
CPT codes and reimbursement numbers are provided in Table 38-8 for incision and drainage (I&D) procedures and in Table 38-9 for foreign body removal.
The Importance of Method
In general, the method of destruction does not change the coding. However, for the anus and genital areas, there are specific codes for the method used (see Table 38-6).
Shave excisions are distinctly different than full excisional procedures that require suture repair. Here, again, the “method” is important. Specific codes are used for shave excisions depending on size and location (see Table 38-10).









