15 Cryosurgery
Cryosurgery is the most commonly performed dermatologic procedure in the United States. There are many different ways to achieve cold temperatures, but clinically, the end result is to freeze the fluid in cells, which causes crystals that damage the cells, resulting in tissue destruction. Different cell types are destroyed at different temperatures (see Table 15-1). Melanocytes are relatively fragile causing the tendency for hypopigmentation with their death. Cartilage and bone are most resistant to freezing and other cells are in between.
TABLE 15-1 Key Events during Freezing Including Cell Death
Temperature (°C) | Event |
|---|---|
| +11 to +3 | 65% of capillaries and 35% to 40% of arterioles and venules develop thrombosis. |
| −0.6 | Freezing begins to occur in tissue. |
| −4 to −7 | Melanocytes die. |
| −15 to −20 | 100% of blood vessels develop thrombosis. |
| −20 | Cells in sebaceous glands and hair follicles die. |
| −21.8 | Ice crystals theoretically form in the tissue (the eutectic temperature of sodium chloride solution). |
| −20 to −30 | Keratinocytes and malignant cells die. |
| −30 to −35 | Fibroblasts die. |
| −50 to −60 | All cells die including cartilage cells. |
Source: Adapted from Vidimos A, Ammirati C, Poblete-Lopez C. Dermatologic Surgery. London: Saunders; 2008; Table 8-3.
Indications
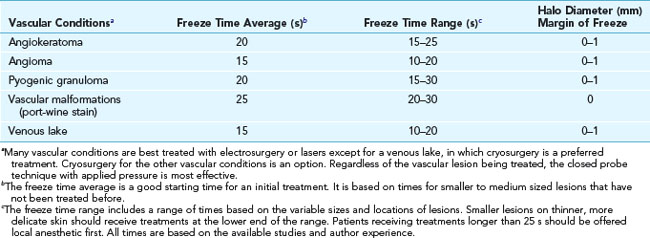
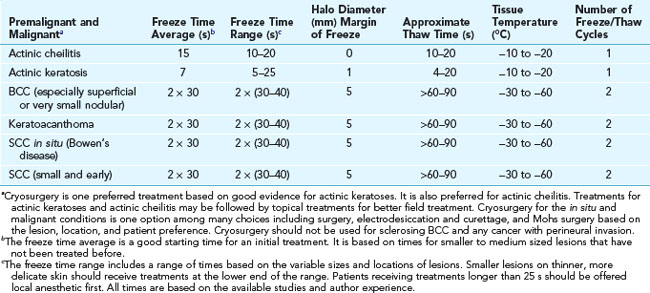
Cryosurgery is most often used to treat actinic keratoses and benign conditions. Table 15-2 provides recommended freeze times and margins of freeze for benign conditions (using liquid nitrogen with an open spray technique). Table 15-3 gives recommended freeze times and margins of freeze for vascular conditions (using liquid nitrogen with a closed probe or an open spray technique). Table 15-4 lists recommendations for treating premalignant and malignant conditions (using liquid nitrogen with an open spray technique). Details on how to perform these procedures follow.
TABLE 15-2 Recommended Freeze Times and Margin of Freeze for Benign Conditions Using Liquid Nitrogen with an Open Spray Technique
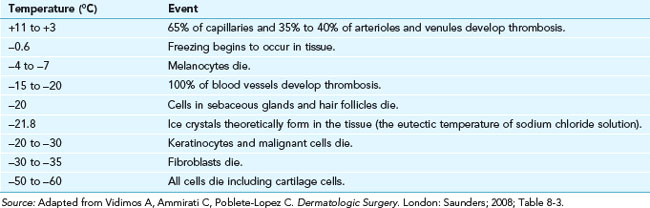
TABLE 15-3 Recommended Freeze Times and Margin of Freeze for Vascular Conditions Using Liquid Nitrogen with a Closed Probe or an Open Spray Technique
Contraindications
Contraindications for cryosurgery are listed in Table 15-5.
TABLE 15-5 Contraindications for Cryosurgery
Contraindications | Category |
|---|---|
| By Lesion | |
| Melanoma | A |
| Recurrent basal cell carcinoma | A |
| Sclerosing basal cell carcinoma (BCC) | A |
| Micronodular BCC | R |
| Nevus | A |
| Any undiagnosed lesion suspicious for non-melanoma malignancy (tissue should be sent for pathology first) | R |
| Morphea | A |
| By Area | |
| Skin cancer on ala nasi and nasolabial fold | R |
| Neoplasm of upper lip near vermillion border | R |
| Neoplasm over the shins | R |
| By Patient | |
| Previous adverse reaction to cryotherapy (e.g., cold anaphylaxis) | A |
| Cryoglobulinemia | R |
| Myeloma, lymphoma | R |
| Autoimmune disorders (including pyoderma gangrenosum) | R |
| Raynaud’s disease, especially when lesion is on fingers, toes, nose, ears, penis | R |
A, Absolute; R, relative.
Advantages of Cryosurgery
Advantages for the patient include:
Disadvantages of Cryosurgery
Disadvantages for the patient include:
Equipment for Liquid Nitrogen
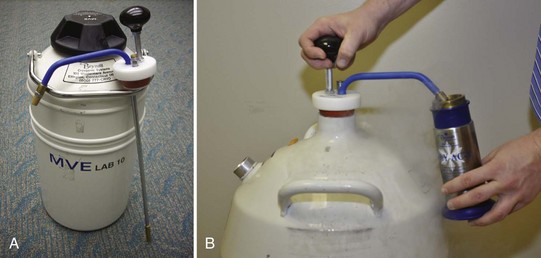

FIGURE 15-2 Two types of cryosurgical spray guns from Brymill (left) and one from Wallach (right).
(Copyright Richard P. Usatine, MD.)

FIGURE 15-4 A large assortment of cryosurgical probes, apertures, and spray tips.
(Copyright Richard P. Usatine, MD.)
Cryosurgery: Principles and Getting Started
TABLE 15-6 Factors That Affect the Freezing of Tissue
Factor | Key Principles |
|---|---|
| Rate of tissue freezing | Rapid freezing causes more cell death. In the open spray technique, this is influenced by the rate of liquid nitrogen spray to the skin (aperture and configuration of the spray conduit). |
| Rate of intermittent spraying | |
| Halo diameter | The wider the halo, the deeper the freeze at the periphery of the lesion. |
| Distance of spray tip to tissue | The closer the tip is to the tissue, the colder the tissue may become because air is not as good a conductor as tissue. |
| Tissue temperature | Final tissue temperature of less than −30°C will kill malignant cells. |
| Duration of freezing | |
| Rate of thawing | Slow thawing causes more cell death. |
| Repetition of freeze/thaw cycles |
Source: Adapted from Vidimos A, Ammirati C. Poblete-Lopez C. Dermatologic Surgery. London: Saunders; 2008; Table 8-2.
Cryosurgery Methods
Many different techniques are used to perform cryosurgery. The most common ones are listed in Table 15-7, which explains how the cryogen is applied and its temperature.
TABLE 15-7 Forms of Various Cryogens and Temperatures
Cryogens | Form | Temperatures (°C) |
|---|---|---|
| Liquid nitrogen | Open spray, closed probes and CTA Tissue temperature is less cold if delivered with CTA | −196 |
| Nitrous oxide in tank | Closed probes on special gun | −89 |
| Solidified CO2 in tank | Closed probes on special gun | −79 |
| CryoPen | Refrigerated closed probes | −75 |
| Verruca-Freeze (chlorodifluoromethane and propane) | Chemical spray into cones or disposable buds with evaporation producing the cold | −70 |
| Wartner (dimethyl ether and propane) | OTC foam applicator for warts only | −57 |
| Histofreezer (dimethyl ether and propane) | Application is via disposable 2- and 5-mm buds | −55 |
Liquid Nitrogen
Liquid nitrogen is stored in dewar containers ranging in size from 5 to 50 L. The nitrogen may be withdrawn using a ladle, a valve system, or a withdrawal tube (Figure 15-1). The withdrawal tube is the most simple and efficient way to extract liquid nitrogen from your storage container.
A more time-effective and more efficacious approach is to use a cryogun (Figure 15-2). Once filled, the unit can be used to treat many patients rapidly. The spray method allows the clinician to reach tissue temperatures of up to −196°C while the CTA is not likely to get below −20°C. Although there is a cost involved in the purchase of a cryogun, these units can last a clinician’s full career and pay for themselves very quickly. The reimbursement for cryosurgery is excellent for only a few minutes of your time.
Michael D. Bryne developed the first handheld spray device using liquid nitrogen for medical use in 1968. His family continues to run the Brymill Corporation, which sells the most widely used cryoguns. The variety of cryoguns available from Brymill include (Figure 15-2):






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


