29 Skin Resurfacing with Ablative Lasers
Ablative laser resurfacing is one of the most effective therapies available for wrinkle reduction. This is an aggressive method of skin resurfacing whereby water in the skin is heated and vaporized by laser energy, causing a controlled injury to the epidermis and dermis. It is most commonly performed using either carbon dioxide (CO2) or erbium:yttrium aluminum garnet (Er:YAG) lasers. Traditional ablative laser resurfacing deeply penetrates the skin (up to 300 µm), and because the epidermis is fully ablated, it is associated with prolonged recovery times, and may have serious complications of infection, hypopigmentation, and scarring1 and, hence, is rarely performed today. Less aggressive superficial ablative treatments (ranging in depth from 20 to 50 µm) are still commonly performed, particularly for reduction of dyschromia and mild wrinkles.2 Superficial ablative laser resurfacing is also referred to as a laser peel.
In 2004, a novel method of fractional resurfacing, which involves treating only a portion or “fraction” of the skin, was introduced.3 Fractional devices deliver laser energy to the skin in microscopic columns, also called microthermal zones. This delivery method allows for very deep penetration in the skin (up to 1.5 µm). Figure 29-1 shows a comparison between deep fractional microthermal zones and “conventional” horizontal plane resurfacing.
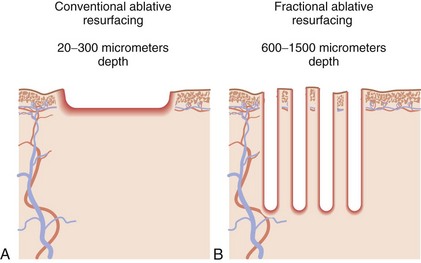
FIGURE 29-1 Ablative laser patterns of injury: (A) conventional “horizontal plane” and (B) fractional.
The untreated adjacent tissue between microthermal zones serves as a reservoir of regenerative cells that migrate into the treatment area and facilitate rapid wound healing. Fractional ablative resurfacing has been shown to effectively reduce wrinkles and improve dyschromia in photoaged skin and has the advantages of reduced recovery time and reduced risks compared to conventional ablative laser resurfacing.4–6
Laser Principles
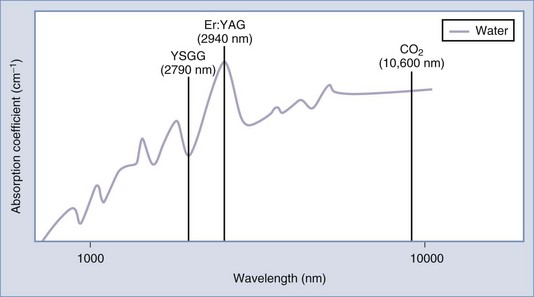
Ablative lasers achieve wrinkle reduction through the use of water as the target chromophore to heat and vaporize tissue. The two main laser wavelengths used for ablative resurfacing, 2940 nm (Er:YAG) and 10,600 nm (carbon dioxide), are well absorbed by water. A third, less frequently used wavelength is 2790 nm (yttrium scandium gallium garnet or YSGG). Figure 29-2 shows the water absorption spectrum and these three ablative resurfacing lasers. Note that the erbium 2940 nm wavelength is at a water absorption peak and is approximately 15 times more highly absorbed by water than CO2.
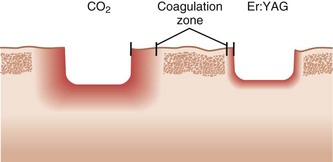
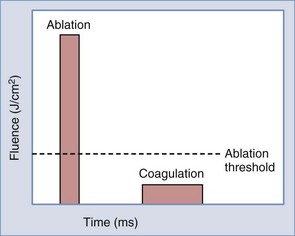
Absorbed laser energy has two main effects on tissue: (1) removal of tissue, called ablation, and (2) heat transference to surrounding tissue, called coagulation. Coagulation clinically results in tissue tightening. A controlled amount of coagulation with treatments is, therefore, desirable but too much thermal injury can be associated with complications such as hypopigmentation and scarring. Due to a greater absorption by water, Er:YAG lasers ablate tissue at lower fluences (approximately 1 J/cm2), compared to CO2 lasers, which require higher fluences to achieve similar ablation (approximately 5 J/cm2). Er:YAG lasers, therefore, cause less thermal damage to the surrounding tissues and have smaller zones of coagulation than CO2 lasers. Figure 29-3 shows the zones of coagulation around a region of ablation with a CO2 versus an erbium laser. The amount of ablation and coagulation is controlled by laser fluence and pulse width (see Chapter 19, Aesthetic Principles and Consultation, for a discussion of laser parameters). Ablation is most effectively achieved with short pulse widths and high fluences, whereas coagulation is achieved with longer pulse widths and lower fluences (Figure 29-4). By varying these two parameters, ablative laser devices can independently control the amounts of ablation and coagulation achieved.
Laser fluence is also a major determinant of the depth of injury with fractional ablative devices, where higher fluences penetrate deeper. Density settings control the percentage of skin that is treated. More aggressive fractional ablative treatments are, therefore, achieved with high fluences and high density parameters. Some fractional devices utilize scanners and computer software to “randomly” deliver pulses within a set pattern so that the pulses are not adjacent to one another. Changing the energy delivery pattern from sequential to nonadjacent pulses allows for high energies to be delivered without the effects of bulk heating.7 This is particularly useful with CO2 devices which cause greater thermal injury.
In summary, fractional ablative laser devices have variable fluences, spot sizes, spot densities, and pulse widths, all of which affect the depth of penetration as well as the degree of ablation and coagulation achieved.8 Because these devices are still relatively new, clinical correlation is required to determine how these different parameters impact results, downtime, and side effects.
Patient Selection
Fitzpatrick skin type classification is an important factor in assessing patients for laser resurfacing (see Chapter 19, Aesthetic Principles and Consultation, for skin type classification). The ideal patient has a fair complexion (Fitzpatrick types I through III) with lesions responsive to laser ablation (see the Indications section below). Patients with darker complexions (Fitzpatrick types IV and V) may be treated as well, but must be informed about their higher risk for pigmentary complications and the need for more cautious treatment parameters, which may limit results. Although patients with Fitzpatrick skin type V may be candidates, in reality these patients rarely present with the facial aging signs that patients with lighter skin types complain of, and one rarely encounters such a patient seeking facial resurfacing. It is advisable for providers getting started with fractional ablative resurfacing to limit treatments to lighter skin types (I through III).
Indications9,10
Ablative laser resurfacing has traditionally been used for patients with more advanced signs of facial aging (Glogau stage IV) including generalized static wrinkles, keratoses, severe dyschromia, sallow color, and coarse pores (see Chapter 19 for a discussion of the Glogau photoaging scale). With the advent of fractional technologies that have more rapid recovery times and fewer risks, ablative laser procedures are being performed in patients with less severe photoaging. Nonetheless, the most common indication today for fractional ablative laser resurfacing is still moderate to severe wrinkles as well as scars.
Alternative Therapies
Skin resurfacing can also be accomplished by mechanical exfoliation procedures such as microdermabrasion and chemical peeling treatments which typically penetrate to the epidermis or upper reticular dermis (see Chapter 22, Chemical Peels and Chapter 23, Microdermabrasion). Dermabrasion is a mechanical, “cold steel” method of removing epidermis, papillary, or upper reticular dermis. Dermabrasion and chemical peeling have the advantage of being less expensive than laser resurfacing. However, extensive hands-on experience in a preceptor environment is required in order to learn the art of dermabrasion.11
Products Currently Available
See the Resources section at the end of the chapter for a list of manufacturers of devices that have these wavelengths.
Contraindications
See the General Laser Contraindications section in Chapter 26, Hair Reduction with Lasers. Additional contraindications include the following:
Disadvantages of Laser Resurfacing
Equipment
Anesthesia—Intraoral Nerve Blocks
Anesthesia—Assistive External Device
See Chapter 20, Anesthesia for Cosmetic Procedures, and Chapter 3, Anesthesia, for more information.
Procedure Preparation
One Month Prior
Preprocedure Skin Care Products
Preprocedure products typically contain retinoids, alpha hydroxy acids, antioxidants such as vitamin C, sunscreens, and, for patients prone to hyperpigmentation, skin lightening agents such as hydroquinone or a cosmeceutical such as kojic acid, arbutin, niacinamide, or azelaic acid are also used.13 The goal for using these products is to condition the skin and create a healthier pretreatment epidermis and dermis, thereby promoting more rapid healing postprocedure. Although prescription-strength retinoids have traditionally been used preprocedure,14 some physicians recommend using less irritating retinoids such as retinol or retinaldehyde.15
Preprocedure skin care for ablative laser treatments should be started 1 month prior to the procedure and discontinued 1 week prior to the procedure to ensure a fully intact epidermis at the time of treatment. In darker Fitzpatrick skin types (III or higher), topical lightening agents, such as hydroquinone 4% to 8%, are commonly used pretreatment (see Chapter 24, Skin Care Products, for preprocedure treatment regimes).
One Week Prior
Fractional Ablative Laser Resurfacing: Steps and Principles
General Treatment Technique
Planning and Designing
Ablative laser resurfacing may be performed to a region of the face or to the entire face. Figure 29-5 shows three of the most commonly treated facial aesthetic subunits (modified from Gonzales-Ulloa16). The periocular subunit is bounded inferiorly by the crest of the zygoma and superiorly by the orbital rim. The upper lip subunit






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


