Key points
• Patient-reported outcome instruments (PROIs) are questionnaires that measure concepts by asking patients directly, without clinician interpretation, and should be used to measure procedural outcomes.
• The FACE-Q is a new validated, reliable, and responsive PROI.
• There are four FACE-Q domains: appearance appraisal, quality of life, process of care, and adverse effects.
• The Face Q link is www.qportfolio.org .
• PROIs can be completed preoperatively, postoperatively, and at all follow-up points, which is important when examining and comparing outcomes pre-and postoperatively, but also to follow outcomes over time.
• Review of PRO data allows surgeons to see where and among which groups they are achieving surgical success and conversely where and among which groups they are not.
• This information is invaluable in that it allows surgeons to set realistic expectations for new patients based on prior outcomes demonstrated among similar patients.
• PRO data enhances physician-patient communication and transparency in the all-important presurgical consultation.
• Utilizing PROIs, surgeons can collect adverse event outcome data from the patient perspective to explain risks, complications, and recovery to each patient so that he or she can make an informed decision regarding surgery.
Introduction
As the field of plastic surgery continues to grow, specifically facial plastic surgery, both cosmetic and reconstructive, the importance of understanding and grading success is crucial. However, in contrast to other fields of medicine and surgery, objective measures of outcome (e.g., physical function and health status) are not the most important factors when evaluating cosmetic facial procedures. Rather, primary measures of success are satisfaction with appearance and improved quality of life, including social confidence and psychologic well-being.
Although it may have historically been acceptable for surgeons to impose their aesthetic preferences on patients, the movement of medicine toward a patient-centered approach has made this approach antiquated. This is especially true given that patients seeking aesthetic surgery span a wide range of cultures and backgrounds. These procedures now transcend all gender, ethnic, age, and socioeconomic lines. As the patient population continues to diversify, it is essential that the surgical community collects information about procedural outcomes, especially outcomes among different groups, with the goal of enhancing procedural transparency.
While some facial surgical procedures are designed to address aesthetic concerns alone, most skeletal facial surgeries are designed to address both aesthetic as well as functional concerns. For example, patients undergoing orthognathic surgery usually have a dentofacial deformity or traumatic injury that cannot be corrected with orthodontic therapy alone. However, the goal of surgery is not only to establish normal anatomic and functional relationships and an ideal dental occlusion, but to optimize facial aesthetics as well. This is why orthognathic surgery is often combined with genioplasty in an attempt to create an ideal aesthetic facial shape of the lower and midface because the chin not only contributes to facial proportion in frontal and lateral views but also supports overlying soft tissues. Therefore, unsurprisingly, primary desired outcomes for patients undergoing orthognathic surgery and genioplasty include not only improved function but also satisfaction with facial appearance and an enhanced quality of life.
In measuring surgical outcomes, historically, the research and clinical communities have generally favored the opinions of the provider. However, in the setting of aesthetic skeletal facial surgical procedures, such as rhinoplasty, orthognathic surgery, and genioplasty, which are typically elective in nature this balance shifts to include patient perception. Therefore in pursuit of the goal of furthering evidence-based medicine, clinically meaningful and scientifically sound patient-reported outcome instruments (PROIs), which are questionnaires that measure concepts by asking patients directly, without clinician interpretation, should be used to measure procedural outcomes. , However, historically, there has been a lack of studies examining patient perceptions of outcomes following aesthetic skeletal facial surgery using validated, reliable, and responsive procedural-specific PROIs, potentially due to a shortage of these instruments. Thankfully, to address the need for cosmetic PROIs, Klassen et al. recently developed the FACE-Q, a new PROI made up of numerous independently functioning scales, many of them area specific and procedure specific. The FACE-Q measures concepts important to facial aesthetic patients, including appearance, health-related quality of life, and process of care.
About the FACE-Q
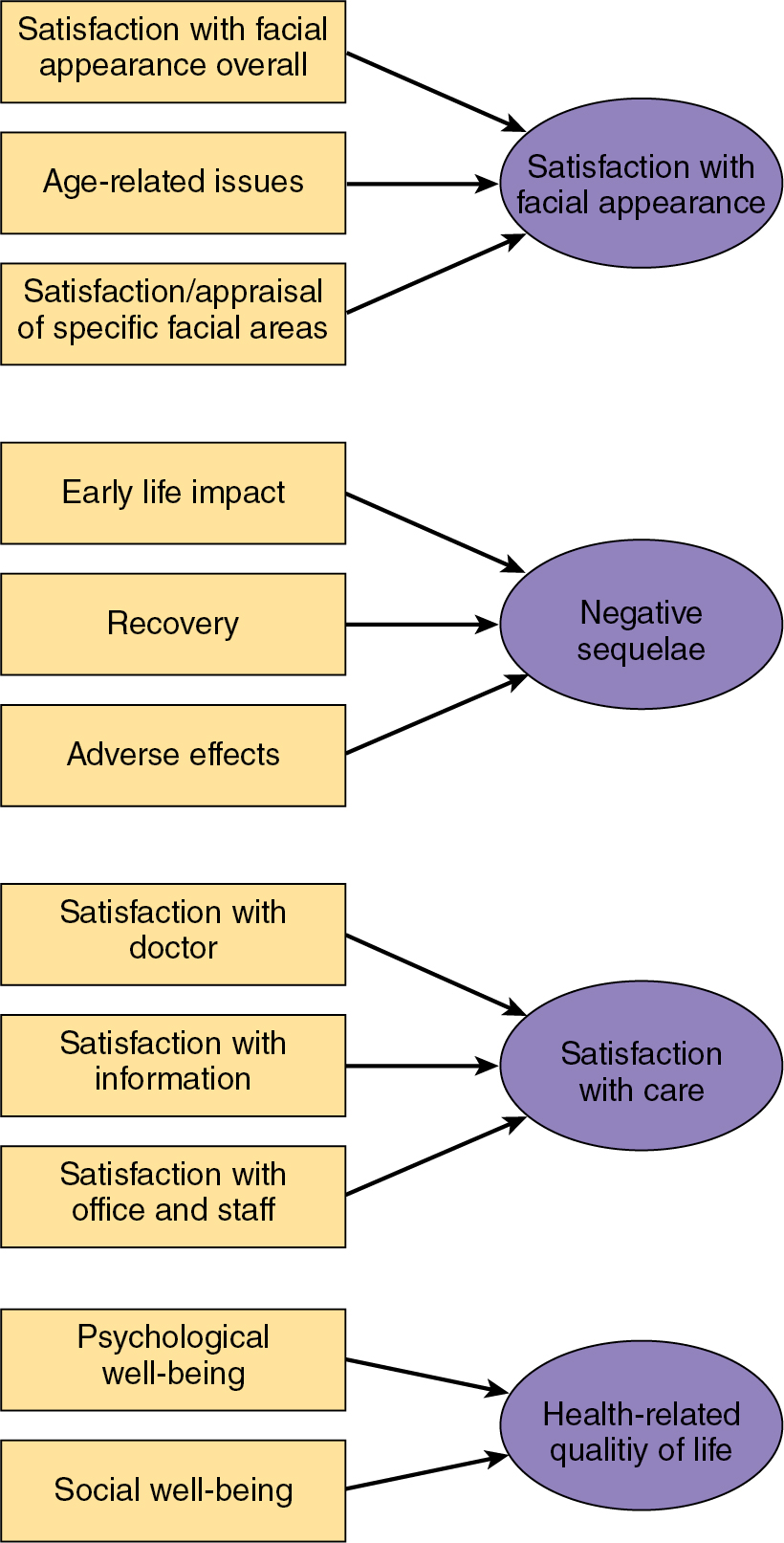
The FACE-Q is a new validated, reliable, and responsive PROI composed of over 40 independently functioning scales that measure outcomes and concepts important to patients undergoing facial aesthetic procedures, both surgical and nonsurgical. There are four FACE-Q domains: appearance appraisal, quality of life, process of care, and adverse effects. ,
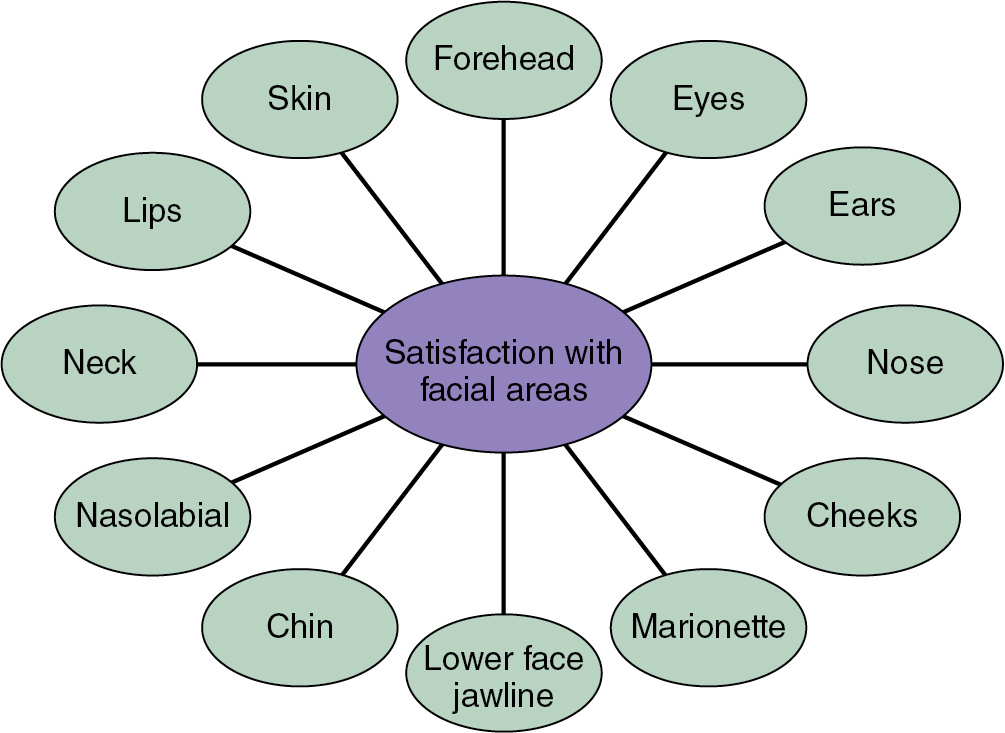
For example, scales that measure appearance appraisal include Satisfaction with Facial Appearance ( Fig. 6.1 ). Overall, as well as more specific scales, such as Satisfaction with Nose, Satisfaction with Chin, Satisfaction with Lower Face and Jawline, and Satisfaction with Forehead. Scales that measure quality of life include Social Function, which measures social confidence, and Psychologic Well-Being. Both scales ask respondents to answer items with facial appearance in mind. Scales that measure process of care include Satisfaction with Doctor, Satisfaction with Decision (to pursue surgery), and Satisfaction with Information Received (regarding/before procedure). Finally, the FACE-Q also includes a series of adverse effects checklists related to procedures undergone. These checklists ask patients to evaluate the most common postoperative symptoms experienced by patients both overall (Recovery Early Symptoms) as well as in different specific areas of the face, depending on which area has been operated on (e.g., Nose, Ears, and Lower Face and Neck).
Validated FACE-Q scales are scored from 0 to 100, with higher FACE-Q scores indicating greater satisfaction with appearance, quality of life, or process of care. The FACE-Q can be completed preoperatively, postoperatively, and at all follow-up points, which is important when examining and comparing outcomes pre- and postoperatively, but also to follow outcomes over time.
Important uses of the FACE-Q
Patients seeking aesthetic skeletal facial surgery span a wide range of cultures and backgrounds. Thus although harmony, symmetry, and function are the ultimate goals of any facial surgery, patients seek a variety of desired objectives and outcomes. There is no one universal result that appeals equally to all patients, even patients of similar backgrounds. Every procedure must be tailored to suit each individual patient.
Additionally, as mentioned earlier, given that patient demographics continue to evolve, it is important that surgeons collect patient-reported outcome (PRO) data relevant to different groups of patients. By reviewing PRO data, surgeons can see where and among which groups they are achieving surgical success and conversely where and among which groups they are not. This information is invaluable in that it provides feedback to surgeons and also allows surgeons to set realistic expectations for new patients based on prior outcomes demonstrated among similar patients. PRO data enhances physician-patient communication and transparency in the all-important presurgical consultation. With the advent of the FACE-Q, surgeons can finally study outcomes differences among various demographic groups by using a validated PROI.
Surgeons have already started using the FACE-Q in an effort to collect PRO data. For example, the FACE-Q has been used to describe demographic predictors of differences in patient satisfaction with appearance and quality of life following rhinoplasty. The study examined gender, age, ethnicity, race, and income and found that while women who undergo rhinoplasty experience significant improvements in satisfaction with facial appearance and quality of life, men are more likely to experience a significant improvement in satisfaction with facial appearance without a corresponding improvement in quality of life. The study also found that Caucasian patients demonstrated statistically significant improvements in satisfaction with facial appearance and quality of life, while non-Caucasians did not. Additionally, patients younger than 35 years of age were more likely to experience enhanced satisfaction with facial appearance and quality of life compared with patients older than 35 years of age. Finally, the study found that patients with annual incomes greater than/equal to $100,000 were more likely to experience significant increases in satisfaction with facial appearance and quality of life compared with patients with annual incomes less than $100,000. Similar studies can and should be conducted among even larger groups of rhinoplasty patients (the above study was conducted among only 59 patients) as well as among patients undergoing other aesthetic skeletal facial procedures with the goal of obtaining more information regarding differences in outcomes among various demographic groups.
As mentioned earlier, in addition to functional outcomes, aesthetic outcomes are also important to patients undergoing skeletal facial surgery. For example, the LeFort I osteotomy, bilateral sagittal split osteotomy (BSSO) of the mandible, and osseous genioplasty are used to reconstruct the facial skeleton, with the goal of restoring the ideal aesthetic form and improving function. Given the importance of the chin in facial appearance, many surgeons opt to perform combined orthognathic surgery and genioplasty to enhance aesthetic outcomes. With the above goals in mind, the FACE-Q has also been used to evaluate outcomes in patients following orthognathic surgery and/or genioplasty ( Fig. 6.2 ). Among 56 patients presenting for orthognathic surgery and/or genioplasty, the authors demonstrated statistically significant improvements in both satisfaction with facial appearance and in quality of life. Specifically, the patients displayed statistically significant improvements in Satisfaction with Facial Appearance Overall, Satisfaction with Lower Face and Jawline, Satisfaction with Chin, and Social Confidence. Of note, there was no improvement found in psychologic well-being.