Graph 2.1 Progression of the clinical presentation of syphilis
VDRL may provide a false positive result in low titers as a result of cross reactivity and a false negative result, mainly during the primary and late latent stages. This may also occur with treponemal screening with less frequency.
The prozone effect occurs when there is an excess of antibodies in relation to the antigen during VDRL testing, producing a false negative result. Upon dilution of the serum, high titers can be observed. This patient will normally be in the secondary phase.
Carriers of HIV more often have different serological responses, in terms of both false positive results and for very high titers.
Clinical presentations that suggest syphilis should not be underestimated, even when serological screening produces a negative result.
Investigation for neurosyphilis should not be delayed for HIV (human immunedeficiency virus) positive patients presenting neurological symptoms/disease.
Graph 2.2 Syphilis diagnosis summary. IF direct immunofluorescence, FT Fontana-Tribondeaux (silver impregnation), PCR Polymerase Chain Reaction
2.7 Evaluation of Laboratory Methods
Exam | Sensitivity (%) | Specificity (%) |
|---|---|---|
Darkfielda | 85–95 | 100 |
Immunofluorescencea | 90–95 | >98 |
VDRL | 70–100b | 79–98c |
FTA-Abs/Elisa | 85–100b | 95–100c |
MHA-TP | 70–100 | 95–100 |
PCR | >95 | >98 |
aVaries according to professional bVaries according to the stage of the disease cVaries according to population | ||
2.7.1 Treatment and Control
Early (primary/secondary) and latent (up to 1 year) infection: single dose of penicillin G benzathine 2,400,000 IU IM (1,200,000 IU in each gluteal region). We prefer to repeat a second dose after an interval of 1 week, avoiding the administration of a single dose.
Latent (over 1 year) and late infection: penicillin G benzathine 2,400,000 IU IM, once a week for 3 weeks.
Neurosyphilis: Crystalline penicillin G 24,000,000 IU per day (4,000,000 IU every 4 h) IV, for 21 days.
Criteria of cure: VDRL 3, 6 and 12 months after treatment must present a reduction in four titers or a negative result from 6 months to 1 year. Pregnant women must be monitored on a monthly basis. A reduction of 1 titer per month is to be expected. Treatment should be repeated if serology increases by four titers.
Alternative drugs: Azithromycin 1 g orally per week for 2 or 3 weeks for cases of syphilis up to 1 year; no studies have been carried out for cases over 1 year. Doxycycline 100 mg orally every 12 h or erythromycin or tetracycline 500 mg orally every 6 h for 14 days for cases of syphilis up to 1 year and for 28 days for cases of syphilis over 1 year.
Pregnant women: Follow the treatment regimen using penicillin G benzathine. Tetracyclines, doxycycline and erythromycin estolate are contraindicated.
Children over 1 month old: Should have a cerebrospinal fluid (CSF) examination to exclude neurosyphilis. Review the patient in full to establish if it is a case of congenital or acquired syphilis. Early latent syphilis: penicillin G benzathine 50,000 units/kg IM, up to the adult dose of 2.4 million units in a single dose. We prefer to repeat a second dose with an interval of 1 week, avoiding the administration of a single dose. Late latent syphilis or latent syphilis of unknown duration: penicillin G benzathine 50,000 units/kg IM, up to the adult dose of 2.4 million units, administered over 3 doses at 1-week intervals (total 150,000 units/kg up to the total adult dose of 7.2 million units)
HIV positive patients: Perform clinical and serological (VDRL) evaluations 3, 6, 9, 12 and 24 months after treatment. These patients have a higher risk of neurological complications than patients that are not infected with HIV. They may also present more cases of serological failure.
Severe penicillin hypersensitivity is much less frequent than is claimed by both popular and medical myth. Those who think otherwise should seek out well-documented information.
2.7.2 Complications
Late syphilis: Neurosyphilis, cardiovascular and mucocutaneous (gums).
Early and late congenital syphilis: Congenital syphilis is a type of watchdog disease for the health system. When it occurs, it shows up errors in the system and the quality of prenatal services. The WHO has established that there should be no more than one case in every 1000 live births. It is known that at least 40% of those conceived by mothers with untreated syphilis during gestation will have serious problems or die. Therefore, pregnant women with syphilis or suspected syphilis should be treated with medical urgency. The incidence of congenital syphilis in many developing countries reflects the disregard, or negligence, of society as a whole (health managers, health professionals, the general population and the media) towards an easily diagnosed disease for which effective treatment is available. However, cases of congenital syphilis can be observed among the disadvantaged communities of developed countries.
Syphilis is considered to be inadequately treated when:
Treatment is carried out using antibiotics other than penicillin.
Treatment is incomplete or inadequate during the clinical phase, even if carried out using penicillin.
Treatment is initiated less than 30 days from birth.
Serological titers increase after treatment.
Sexual partners are not treated or this treatment is not documented.
Even in cases where pregnant women are adequately treated for syphilis, newborns must be checked for the disease. Although not common, babies can still contract congenital syphilis from an adequately treated mother.
Positive serological results for newborns of mothers with syphilis may occur up to 18 months after birth.
When evaluating a case of suspected congenital syphilis, the patient’s full clinical history must be considered; clinical and serological tests for the mother; serology and bone radiology for the newborn and clinical and serological tests for the mother’s sexual partner.
The sexual partner should never be forgotten. The clinical examination, serological tests and adequate treatment of this individual are imperative.
2.7.3 Differential Diagnosis
Herpes simplex, soft chancre, Rollet’s mixed chancre (hard + soft chancre), donovanosis, pharmacodermia, exanthematous viruses, fissures and traumatic ulcers.
2.7.4 Observations
Pregnant women must undergo at least two serological tests, one on their first visit and the other in the 34th–36th week of pregnancy. Any genital lesions must be investigated immediately.
Request for serology immediately after treatment is not indicated.
In cases of hypersensitivity to penicillin, desensitization should only be carried out in a safe environment with experienced professionals.
Serology can present low titers (1:4) for the rest of the patient’s life, even after correct treatment.
Treatment failure can occur with any therapeutic regimen, although there are no reports of resistance of Treponema pallidum to penicillin.
Treatment failure may occur as a result of falsified medicines. Unfortunately this situation can occur in any country.
In cases where the exact time of infection is unknown, it is better to opt for a treatment regimen of three doses of penicillin G benzathine at weekly intervals.
A Jarisch-Herxheimer reaction may occur after the first dose of any treponemicidal medication. This will manifest as an exacerbation of skin lesions, fever, headache and arthralgia. This occurs more frequently at the exanthematous stage and responds well to analgesics and antipyretics. However, some professionals recommend betamethasone 12 mg IM and acetylsalicylic acid 500 mg orally before the first dose of antibiotics in patients with severe secondary syphilis mucocutaneous lesions.
Although azithromycin can be used in pregnant women, it is important to remember that this drug does not cross the placental barrier. Therefore, after birth the child must be evaluated and treated. For this reason, penicillin continues to be the first treatment option. Its substitution should be analyzed with extreme care.
As many laboratories no longer perform the FTA-Abs test, we find it practical to request treponemal screening without specifying which type of exam.
Based on our knowledge of syphilis serology we do not recommend requesting FTA-Abs-IgM, as false positive results are very common.

Fig. 2.1
An adolescent patient who had already sought out health services twice, complaining of this painless lesion that appeared 2 weeks previously. Diagnosis: hard chancre. On one occasion, in a room at the Brazilian College of Surgeons in Rio de Janeiro, I heard Professor Eduardo Rabelo say the following phrase: “Any genital lesion has a 90% chance of being syphilitic; we need to think syphilitically.” I had already heard this phrase spoken by various brilliant physicians. Older colleagues affirmed that the phrase was first spoken by Prof. Feijó. Regardless of the author of this phrase, this figure of 90%, is still a challenge for us now in 2011, as we still see many cases of syphilis that pass through various physicians without the hypothesis of infection by T. pallidum ever being raised

Fig. 2.2
Similar to the previous case: hard chancre. It has this name as if the lesion is palpated, hardening around the base and the edges can be observed, which is typical of invasion by mononuclear cells

Fig. 2.3
Case of hard chancre identical to the previous examples, representing the location where the Treponema entered the patient. This is also called an inoculation chancre. Some time ago it was believed that the disease primarily stayed in the genital area and then spread to the skin and the other organs. Today we know that syphilis is a systemic disease from the beginning, as it rapidly spreads from the point it entered to the satellite lymph nodes and beyond. Therefore, we prefer to classify syphilis as early, latent and late instead of primary, secondary and tertiary. From our point of view, this is physiopathogenically more correct

Fig. 2.4
In this case, the hard chancre looks more like desquamation

Fig. 2.5
As well as the classic single, painless, hardened lesion, we can also observe papillae on the corona of the glans indicated by the arrows. Many still confuse these with HPV infection. These are absolutely normal glandular formations

Fig. 2.6
With this case of hard chancre we want to highlight the visible edema on the foreskin, and the detail that upon covering and exposing the glans, the part of the foreskin around the lesion does not fold. This is due to lymphoplasmocytic infiltration, which causes the edges and base of the initial syphilis lesion to harden

Fig. 2.7
Very similar to the previous case and to Fig. 2.15 of this chapter. This patient reported having a fixed non-exclusive partner who was examined and whose clinical examination was normal. Syphilis serology for the partner was negative. After an interval of 30 days, the serology exam was repeated, and on this occasion was positive: VDRL 1:16 and FTA-Abs also positive

Fig. 2.8
In the vast majority of cases, hard chancre lesions in men present in the form of a single painless or relatively painless lesion with a hard base, which even without specific treatment will tend to recede within 30–60 days

Fig. 2.9
You can always count the number of times it has been possible to clearly determine an initial hard chancre lesion in a female patient on one hand. In over 2000 closely followed cases of syphilis, in only four will you be confident enough to affirm that it is a hard chancre. I have four photographs. When the hard chancre is well documented in women, it is more frequently observed on the vulva, as is shown in this case. Syphilis is more often diagnosed in women during the roseola or papular or erosive genital syphilide stage and not during the initial hard chancre stageIt would be logical to believe that initial lesions are found more frequently in the vagina and cervix, which would make diagnosis more difficult. In these situations, the woman generally presents with vaginal discharge and receives topical medicines for vaginitis. As the hard chancre then recedes, many of these are not diagnosed. As the syphilis develops, these cases provide another opportunity for diagnosis at a later stage with the appearance of the mucocutaneous lesions characteristic of secondary syphilis

Fig. 2.10
Attention must be paid to searching for adenopathy, which is generally bilateral and painless, accompanying the hard chancre (arrow) in practically 100% of cases. Still a case of hard chancre. One of our partners was consulted without the clinical manifestations of syphilis and negative serological tests (VDRL, FTA-Abs). In such situations, the correct conduct would be to introduce treponemicidal medication

Fig. 2.11
It may be difficult to accept such as case as a hard chancre. However, as a result of diagnostic confirmation, positive results from direct darkfield microscopy, serology (VDRL 1:16) and a bilateral inguinal lymphapolydenomegaly, it was confirmed to be a hard chancre. Observe the prominent edges in the close up

Fig. 2.12
A young patient who presented both a hard chancre on the vulva and vaginal discharge. Highlighted are the base and edges of the hard chancre

Fig. 2.13
An adolescent who had a hard chancre for over 20 days and was applying a polyvalent cream (antibiotic, antifungal and corticosteroid) because VDRL had been negative and the possibility of syphilis was rejected. It is worth remembering that at the initial hard chancre stage it is common that serology will not react. The diagnostic standard is to look for treponema in the lesion (darkfield microscopy)
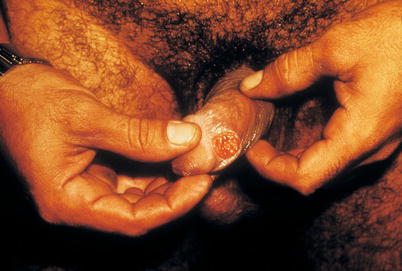
Fig. 2.14
A patient with a large and relatively painless ulcerative lesion on the balanopreputial groove, frenulum and penile body, the final diagnosis of which was hard chancre

Fig. 2.15
This type of lesion has already been shown. Note the edema around the hard chancre lesion. The skin around the lesion is so infiltrated that it doesn’t have enough elasticity to fold
Fig. 2.16
A patient who was seen at the STD (sexually transmitted disease) clinic at UFF (Universidade Federal Fluminense) with a single, painless ulcerative lesion to the penis. He reported that the lesion appeared approximately 25 days after unprotected sexual contact with a new partner. Upon clinical examination, we found a lesion with a hard base (a), bilateral inguinal micropolyadenomegaly and vegetative lesions (b), also on the shaft of the penis. Material was collected from the lesion (c) for direct darkfield microscopy, which was positive for spirochetal bacteria. An excision was carried out on the condyloma lesions, treatment with penicillin G benzathine was initiated and a vaccine was prescribed for hepatitis B, although the latter was refused by the patient
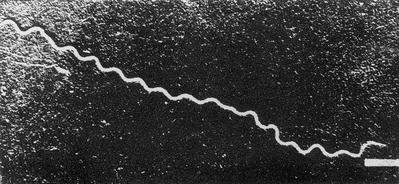
Fig. 2.17
Since cultures of T. pallidum still do not exist, the gold standard for diagnosis is still to find bacteria in the lesion through direct microscopy. Some physicians recommend DNA-Tp PCR screening as standard practice. However, this molecular technique is not readily available for most physicians around the world, even in developed countries. The most frequently used technique is dark field microscopy, although silver Impregnation (Fontana-Tribondeaux) and immunofluorescence may also be used. The latter normally provides results just as good as those of darkfield microscopy. A molecular biology technique for the diagnosis of Treponema pallidum has been available on the world market for years. One product is being used for the diagnosis of genital ulcers, with which it is possible to detect the DNA of T. pallidum, herpesvirus and H. ducreyi using the same sample (Multiplex-Roche). This electron micrograph shows a sample of T. pallidum
Fig. 2.18
We like to spread the concept of thinking syphilitically, because syphilis is much more common than is realized, especially in developing countries and the vulnerable populations of developed countries. In this figure, we can observe (a) a hard chancre lesion in the balanopreputial groove next to the frenulum. But in (b) the lesions are caused by genital herpes. After receiving advice, the patient agreed to undergo a HIV test. The result was positive. Cases involving more than one STD are common. Avoid ending investigations after the diagnosis of just one STD and seek to check for other possibilities

Fig. 2.19
Initial lesions on the vagina, mouth and anus are not always that same as the typical lesions of the penis. This is a case of a hard chancre on the anus. It is common for multiple lesions to occur in this region

Fig. 2.20
The same situation as shown in the previous figure. Note here that to get a better look at the lesions you need to pull back the anal rim, but take care as these lesions are generally painful. These areas are rich in other bacteria, so proof via the presence of bacteria (T. pallidum) is not as easy. Sometimes other non-pathogenic spirochetes with coarse morphology can be found in this area. This may be confusing. Although inguinal adenopathy can exist, it is generally smaller than lesions on the penis or vulva. This is due to the lymphatic drainage of the anus not occurring solely via inguinal lymph nodes

Fig. 2.21
This patient complained mainly of urethral discharge. During the exam, a set of hard chancres was identified on the internal wall of the foreskin when the patient exposed the area further for photography. The patient also reacted positive to hepatitis B serology

Fig. 2.22
A young patient seen at the STD clinic at the Matta Foundation in Manaus, Amazonas State, with a hard chancre on the base of the penis. It is worth remembering that sometimes condoms do not cover this area very well. Some physicians call this “condom chancre” as transmission may occur even using a condom. Following this logic, transmission will not occur using a female condom as it covers a wider area. Lesions in this area are rare, as are those on the scrotum

Fig. 2.23
This figure illustrates the case of a patient with a hard chancre (a), genital herpes lesions (b) and gonococcal urethritis (c). After receiving advice, the patient underwent HIV and hepatitis B testing, the results of both being positive. The partner was examined and presented endocervicitis with a large quantity of pus and pelvic pain. They underwent two HIV exams and tested negative both times. The patient reported being a drug user (nasal cocaine) and having extramarital sexual relations (2 or 3 per year). Edema around the syphilitic lesion on the frenulum can be observed in the close up (a)

Fig. 2.24
The Fontana-Tribondeaux method showing spirochetes using a common microscope (magnified 1.000×). Silver salts attach to the surface of the bacteria, increasing their thickness and making them visible under a microscope. Direct examination of syphilitic lesions using this technique is a viable alternative when a darkfield condenser is not available, although it is not very sensitive and is completely dependent on correct sampling of clinical material
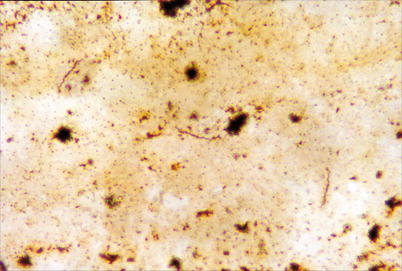
Fig. 2.25
Treponema pallidum impregnated with silver salts using the Fontana-Tribondeaux method. Spirochetes are dark brown against a light brown background (magnified 1.000×). Clinical material must be sampled after cleaning the ulcer with sterile saline solution and using one of the following methods:Apply a drop of commercial sulfuric ether on the clean base of the lesion, wait around 1–2 min for exudate to be produced which will mobilize the treponemes from their sub epithelial position. Then add a drop of sterile saline solution and collect the mixture with a spatula or platinum or plastic loop, using this to place a thin smear on a slide in one direction only, avoiding circular movements. Leave the sample to dry at room temperature before proceeding. Another method is to use a dry gauze to scarify the base of the lesion very carefully in order to avoid bleeding, which may interfere with the final result if this material is observed under a darkfield microscope. If this occurs, dry off the blood and start again, sampling the exudate according to the method described above
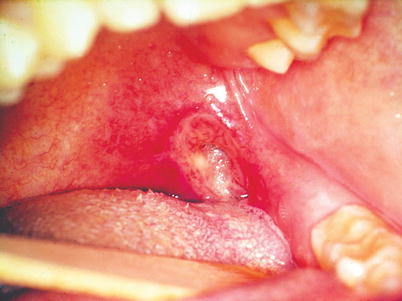
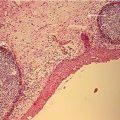
Fig. 2.26
Ulcerative lesion, with raised hardened edges and a clean base in a patient who was infected during oral sex, whose clinical diagnosis was confirmed in the laboratory through visualization of Treponema pallidum under a darkfield microscope and through histopathological findings of inflammatory infiltrate and periarteritis, confirming the hard chancre as a primary syphilis. Left submandibular inflammatory lymph nodes were palpable

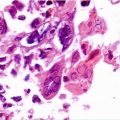
Fig. 2.27
Image showing a slightly irregular depressed area with loss of papillae in the median region of the tongue, characterizing erythematous candidiasis. On the anterior portion there is an irregular ulcerative hard chancre with hardened edges (see arrow). This patient had HIV. The submental lymph nodes were palpable

Fig. 2.28
Painless lesion located in the region between the red of the lip and the mucous membrane, with raised edges, well defined with an erythematous halo and a base covered in a whitish necrotic material. During examination the patient reported that the lesion had appeared 10 days previously after practicing oral sex with a prostitute. A sample was collected from the base of the lesion and the presence of spirochetes morphologically compatible with Treponema pallidum were identified, characterizing a primary syphilis lesion. The patient returned just 3 weeks later and the lesion had practically disappeared. However, VDRL presented a titer value of 1:128. During the first consultation, the patient was medicated with penicillin G benzathine
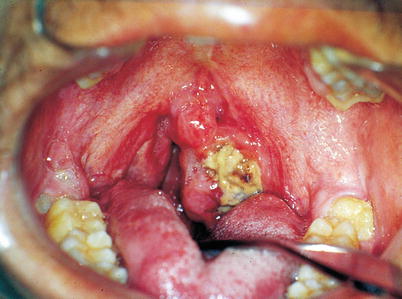
Fig. 2.29
HIV positive homosexual patient with leprosy who practiced oral sex, with an extremely painful ulcerative crater-shaped lesion full of intense inflammatory infiltrate with a necrotic base in the oropharyngeal transition area. The retroauricular and submandibular lymph nodes on the same side as the lesion were palpable, painful and movable. The probable clinical diagnosis was hard chancre, however, collection of material identified the presence of Fusobacterium necrophorum and Prevotella intermedia, as well as Bororrelia vincent, Porphyromonas gingivalis, Tannerella forsynthesis, Treponema denticola, Staphylococcus aureus and non hemolytic specimens of Streptococcus. Blood testing presented anemia and significant leukocytosis. The lesion had a fetid odor and was diagnosed as cancrum oris, serving as a differential diagnosis for syphilitic hard chancre

Fig. 2.30
Male bisexual patient who practiced oral sex, with an extremely painful crateriform ulcer with raised edges and a clean base located in the region of the lingual belly and extending to the left edge of the tongue. This had appeared 2 weeks previously and there were no other lesions in the mouth. Left submandibular lymph nodes were palpable and painful. Hard chancre was one of the considered diagnoses; however, collection of material for microbial analysis was negative, leading to a diagnosis of major aphthous ulceration. Medication with corticosteroids started the healing process. Investigations to seek any immunological origins for the lesion were then initiated

Fig. 2.31
Male patient of 54 years who reported practicing oral sex and using inhaled drugs, and who upon examination presented an ulcerative lesion with hardened and raised edges. Considering the patient’s anamnesis and the clinical characteristics of the lesion, one of the considered diagnoses was hard chancre. After detailed observation of the ulcer, which had a base speckled with erythematous spots and a moriform appearance, diagnosis was confirmed using exfoliative cytology and biopsy. The fungus Paracoccidioides brasiliensis was found on histological sections impregnated with Grocott-Gomori methenamine silver stain. The patient was referred for systemic investigations, and among the most important findings were pulmonary lesions caused by paracoccidioidomycosis and HIV positive serology

Fig. 2.32
Male patient of 42 years, street seller and smoker who frequently practiced oral sex, presenting an irregular ulcer with elevated and hardened edges and a clean base fixed to underlying structures, located on the lower lip and extending from to the labial mucosa. The patient reported that the lesion had been present for 6 months. Since hard chancre on the lip mimics the clinical characteristics presented, we could include this as a probable differential diagnosis. Contrary to diagnosis of hard chancre were the time that the lesion had been present and risk factors for epidermoid carcinoma that included the patients profession, exposing him to UV radiation, and smoking. This diagnosis was confirmed after biopsy and histopathological examination

Fig. 2.33
Patient exhibiting a linear and irregular “snail track” erythematous lesion on the upper lip, which has been classically described by Alfred Fournier as one of the clinical signs of secondary syphilis. It should be observed that it is the patient lifting their own upper lip, as professionals must use gloves during physical examination to avoid possible contamination
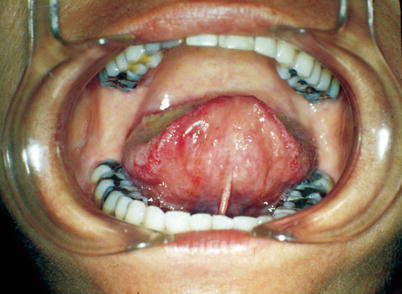
Fig. 2.34
Previously described patient presenting linear and irregular erythematous areas bilaterally covering the lingual belly during the secondary phase of syphilis

Fig. 2.35
Patient lifting her upper lip to reveal a labial mucosa with opal-white coloration and irregular erythematous serpiginous lines, a clinical sign of secondary syphilis

Fig. 2.36
View of the soft palate and oropharynx of the previously described patient, revealing opal-white plates with edges marked with irregular lines, a sign of secondary syphilis in the mouth

Fig. 2.37
View of the anterior region of the buccal vestibule of the same patient, revealing the irregular erythematous area with the white necrotic plates associated with secondary syphilis

Fig. 2.38
Patient presenting irregular white plates on the lower lip surrounded by a erythematous halo, repeated in the region between the soft and hard palate in the second stage of syphilis

Fig. 2.39
White necrotic plates located bilaterally in the anterior region of the lingual belly, where erythematous areas can also be observed in the region between the lingual belly and the floor of the mouth, both clinical manifestations of secondary syphilis in the buccal cavity

Fig. 2.40
Female patient with an irregular white erythematous plate in the anterior region of the buccal mucosa, a clinical characteristic of secondary syphilis that was confirmed with serological exams (FTA-Abs and VDRL). The patient’s partner presented hard chancre on the penis and on a finger

Fig. 2.41
The same patient presenting white erythematous areas in the anterior region of the buccal mucosa, identical to those observed on the other side, another sign of secondary syphilis

Fig. 2.42
Patient with secondary syphilis, presenting an elevated irregular white necrotic plate with a wrinkled surface located on the on the left side of the edge and belly of the tongue. This condition is known as flat condyloma or papular syphilide. At the top of the image an irregular red plate can be observed covering the hard palate close to the molar teeth

Fig. 2.43
The same patient presenting an irregular, elevated white necrotic plate with a wrinkled surface, located on the right side of the edge and the belly of the tongue

Fig. 2.44
Patient in the secondary phase of syphilis presenting irregular, elevated white necrotic plates, with a wrinkled surface and separated by erythematous areas, located on the right side of the tongue, characterizing syphilitic flat condyloma (condyloma latum)

Fig. 2.45
The previous patient in the secondary phase of syphilis, viewed from the front, showing in detail the irregular and raised white necrotic plates, with wrinkled surfaces and separated by erythematous areas, characterizing flat condyloma

Fig. 2.46
Patient presenting an irregular white area (and other with necrotic) on the anterior and mid hard palate, permeated on its edges by erythematous areas. As well as these buccal lesions, the patient presented typical syphilitic roseola lesions spread across various cutaneous areas

Fig. 2.47
The patient described above, from a side view, presenting maculopapular cutaneous lesions typical of syphilitic roseola

Fig. 2.48
There is a well-known phrase by Ricord, who said: “Satellite adenopathy accompanies chancre like a shadow accompanies the body.”Adenopathy is generally bilateral, mostly or totally painless, micropolyadenomegaly (olive stone) and not inflamed. It is obviously satellite to the inoculation chancre. If the chancre is in the mouth, adenitis will be cervical; if it on the finger it will be in the corresponding underarm. It may, as is shown in this figure, present one side more prominent than the other. The patient in question presented various syphilitic lesions on the vulva (Not hard chancre but papular syphilides) and cervicovaginitis caused by gonococcus and Trichomonas vaginalis

Fig. 2.49
Syphilitic adenitis may sometimes become inflamed, and may even drain spontaneously. This did not happen with this patient. She sought medical help for vaginal discharge, vulval lesions and a “lump” on her groin. She was prescribed with vaginal cream, oral acyclovir and doxicycline and incision and draining of the inguinal lump. She sought medical help the following day, complaining of arthralgia, headache, fever and red blotches covering her body. The result of VDRL was 1:256. This is clinically defined as a Jarisch-Herxheimer reaction. It is not recommend incision and draining of adenitis. Antibiotics will generally solve the problem. In these cases, healing can take a very long time

Fig. 2.50
Another case of syphilitic adenitis. We would include to the phrase that adenitis accompanies chancre that it also accompanies syphilids. This is the groin of the patient in Fig. 2.69

Fig. 2.51
Groin of another patient with papular syphilides on the penis. The arrow indicates the largest protrusion

Fig. 2.52
If the development of syphilitic lesions is observed, the progression of the disease can be seen. This figure shows a case of syphilitic roseola. These are red blotches on the skin, mainly on the trunk, characterizing the exanthematous stage. They are generally not itchy and tend to disappear in 30–40 days, even without treatment. The patient often presents with flue-type symptoms (low fever, asthenia, sweating, headache, arthralgia). This phase demonstrates the dissemination of Treponema pallidum throughout the whole body. The skin reflects what is happening, perhaps on a lower scale, to the spleen, liver and lungs

Fig. 2.53
This 74-year-old patient was prescribed with an antihistamine, as it was thought that he had eaten bad shrimp. In reality, he was having sexual relations with a woman who did not know she had syphilis. Not even her doctor knew this, as she had a discreet ulcerative lesion on the vulva, slight inguinal adenitis and was prescribed medication for recurrent herpes, because the patient in question had presented with a small similar lesion to that shown here 2 months previously. VDRL presented a positive result of 1:128 for her and 1:256 for him
Fig. 2.54
(a) Trunk of a patient with syphilitic roseola. In (b), areas of erythema with papular lesions, sometimes eroded and demarcated. The lesions presented at various stages

Fig. 2.55
As well as typical roseola lesions, erythematous plates can also be observed, with a superficial trauma appearing
Fig. 2.56
An adult, homosexual patient who had multiple partners without using condoms, presenting exanthema across all of his skin and buccal cavity, including palmoplantar rosellas. He is a patient at the STD clinic at UFF, where he was treated for early syphilis 5 years previously. Questioned about condom use, he claimed that oral sex with a condom made him vomit and that as he was homosexual he would always be at risk. Serology was positive for syphilis and negative for HIV. When we advised him to refer his partners for treatment, his mother, who was with him during the consultation said: “There’s going to be a huge line here, doctor”. We responded that that wouldn’t be a problem and that it would be better for everybody
Fig. 2.57




(a) This type of case of syphilis is not rare. (a) Satellite inguinal adenitis around lesions to the vulva; (b) palmar roseola; (c) papuloulcerative lesions to the vulva and perineum. (b) The arrow indicates a large inguinal protrusion, more notably to the left. In the genital area, papuloulcerative lesions can be seen on the perineum. (c) A more detailed look at the perineal and perianal lesions. This case illustrates the need to observe the multiple lesions that early syphilis can present
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
