(1)
Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil
7.1 Gonorrhea
7.1.1 Synonymy
Gonococcal disease, blennorrhea, clap, drip.
7.1.2 Concept
Infectious and contagious disease of the mucous membranes. Classic STD transmitted through intercourse in almost all cases; accidental or perinatal contamination is an exception.
More than a million STIs are acquired every day. In 2012, an estimated 357 million new cases of curable STIs (gonorrhoea, chlamydia, syphilis and trichomoniasis) occurred among 15–49 year-olds worldwide, including 78 million cases of gonorrhoea [1].
7.1.3 Incubation Period
Two to ten days after infecting contact. However, there are cases’ reports of incubation period of 24 h and others which exceeds 20 days.
7.1.4 Etiological Agent
Neisseria gonorrhoeae. A diplococcus Gram-negative bacterium and polymorphonuclear intracellular. However, it may have its morphology and staining characteristics altered during chronic processes or after the use of antibiotics. This bacterium can be found extracellularly in the early stages of infection.
Sensitive to most antiseptics, dyes easily outside its habitat.
Often strains are detected with antimicrobial, plasmidial and chromosomal resistance.
7.1.5 Clinical Presentation (Figs. 7.1, 7.2, 7.4–7.26, 7.28–7.41, 7.44–7.51)
Man: Sensation of formication or intraurethral itching with dysuria. Soon after, the urethral mucous arises and quickly becomes mucopurulent, with abundant and spontaneous elimination at the lightest pressure of the penis. The urethral meatus edges become swollen and erythematous.
Woman: The gonococcal urethritis has no exuberance of symptoms as in men, and the clinical picture is composed of dysuria, urinary urgency and, less often, yellowish secretion. Cases are generally only explained by endocervicitis, which becomes a gonococcal infection suspicion when associated with the anamnesis data.
It is assumed that half of the women infected with gonococcus is oligosymptomatic or even asymptomatic.
Women with clinical sign of turbid or purulent cervical mucus complaining about pelvic pain or painful vaginal touch must be investigated into gonococcus and Chlamydia.
Purulent vulvovaginitis due to gonococcus, although rare, is more frequent in rape victims and children, or during the first vaginal intercourse in pubescent women as they have the vaginal epithelium somewhat stratified.
The pharynx and anus exposure of women and mainly of men who have sex with men is asymptomatic or oligosymptomatic in most patients.
7.1.6 Laboratory Diagnosis (Figs. 7.43, 7.52–7.60)
Direct bacterioscopy: the Gram stain technique of urethral secretions shows the presence of Gram-negative diplococci inside polymorphonuclear.
Culture: Thayer-Martin selective medium.
Molecular biology technique (NAAT [nucleic acid amplification test]; hybrid capture)—high sensitivity and specificity comparable to culture, which actually are increasingly obsolete. There are PCR kits that allow the diagnosis of multiple simultaneous infections including Chlamydia trachomatis, Mycoplasma sp., Ureaplasma urealyticun. Materials for these techniques can be collected by health professionals or by self-collecting. Specially, the first urine of the day.
In cases of acute urethritis in men, the bacterioscopy is a good method. In woman, culture or molecular biology techniques of cervical canal is the best option.
In women the simultaneous research in the urethra and endocervix is a good conduct, as the chances of positive results are increased.
Evaluation of Laboratory Methods
Exam | Sensitivity % | Specificity % |
|---|---|---|
Gram | ||
Urethra | 90–95 | 95–99 |
Endocervix | 45–65 | 90–99 |
Vagina, anus | Not recommended | |
Culture | ||
Urethra | 94–98 | >99 |
Endocervix | 85–95 | >99 |
Molecular biology | ||
PCR, hybrid capture | 95–98 | >99 |
7.1.7 Treatment and Control
Unrestricted access to antimicrobials combined with inadequate selection, overuse and subdoses of antibiotics, as well as the inherent genetic mutations of bacteria have contributed to the development of antibiotic resistance to N. gonorrhoeae throughout the world and is a constant concern of epidemiological control centers.
We have listed official protocols of cases of urethral, cervical and anorectal involvement with no complications of the Centers for Disease Control (CDC) 2015 [1], World Health Organization (WHO) Guideline, 2016 [2].
7.1.7.1 CDC 2015 [2]
Esquema recomendado: Ceftriaxona 250 mg, IM, dose única, mais Azitromicina1 g VO, dose única.
Esquema alternativo: Ceftizoxima 500 mg, IM, dose única; ou Cefoxitina 2 g, IM, com probenecida 1 g, VO, dose única; ou Cefotaxima 500 mg, IM, dose única.
7.1.7.2 WHO 2016 [1]
Treatment and Control of Gonococcal Infections
Genital and Anorectal Gonococcal Infections
The WHO STI guideline recommends that local resistance data should determine the choice of therapy (both for dual therapy and single therapy).
In settings where local resistance data are not available, the WHO STI guideline suggests dual therapy over single therapy for people with genital or anorectal gonorrhoea.
The WHO STI guideline suggests the following options:
Dual therapy (one of the following)
ceftriaxone 250 mg intramuscular (IM) as a single dose PLUS azithromycin 1 g orally as a single dose
cefixime 400 mg orally as a single dose PLUS azithromycin 1 g orally as a single dose Single therapy (one of the following, based on recent local resistance data confirming susceptibility to the antimicrobial)
ceftriaxone 250 mg IM as a single dose
cefixime 400 mg orally as a single dose
spectinomycin 2 g IM as a single dose.
Remarks: Because of the emerging resistance data for gonococcal infections and reduced effectiveness of some medicines, good practice dictates that the choice of treatment depends on reliable local data on antimicrobial susceptibility. Alternative single-medicine therapies, such as gentamicin or kanamycin, have not been suggested due to lack of surveillance data. Guidance for surveillance of antimicrobial resistance in N. gonorrhoeae is available from WHO [3]. This recommendation applies to pregnant women, who should be closely monitored for complications.
Oropharyngeal Gonococcal Infections
In adults and adolescents with gonococcal oropharyngeal infections, the WHO STI guideline suggests dual therapy over single therapy.
The WHO STI guideline suggests the following options: Dual therapy (one of the following)
ceftriaxone 250 mg intramuscular (IM) as a single dose PLUS azithromycin 1 g orally as a single dose
cefixime 400 mg orally as a single dose PLUS azithromycin 1 g orally as a single dose
Single therapy (based on recent local resistance data confirming susceptibility to the antimicrobial)
ceftriaxone 250 mg IM as single dose.
Remarks: Treatment failures have been observed after single therapy for gonococcal oropharyngeal infections and therefore dual therapy is suggested over single therapy.
This recommendation applies to pregnant women, who should be closely monitored for complications.
Retreatment of Gonococcal Infections After Treatment Failure
In people with gonococcal infections who have failed treatment, the WHO STI guideline suggests the following options.
If reinfection is suspected, re-treat with a WHO-recommended regimen, reinforce sexual abstinence or condom use, and provide partner treatment.
If treatment failure occurred after treatment with a regimen not recommended by WHO, re-treat with a WHO-recommended regimen.
If treatment failure occurred and resistance data are available, re-treat according to susceptibility.
If treatment failure occurred after treatment with a WHO-recommended single therapy, re-treat with WHO-recommended dual therapy.
If treatment failure occurred after a WHO-recommended dual therapy, re-treat with one of the following dual therapies:
ceftriaxone 500 mg IM as a single dose PLUS azithromycin 2 g orally as a single dose
cefixime 800 mg orally as a single dose PLUS azithromycin 2 g orally as a single dose
gentamicin 240 mg IM as a single dose PLUS azithromycin 2 g orally as a single dose
spectinomycin 2 g IM as a single dose (if not an oropharyngeal infection) PLUS azithromycin 2 g orally as a single dose.
Remarks: Before retreatment, reinfection should be distinguished from treatment failure, resistance data should be obtained when possible, and the WHO-recommended regimens should be used.
Gonococcal Ophthalmia Neonatorum
In neonates with gonococcal conjunctivitis, the WHO STI guideline suggests one of the following treatment options:
ceftriaxone 50 mg/kg (maximum 150 mg) IM as a single dose
kanamycin 25 mg/kg (maximum 75 mg) IM as a single dose
spectinomycin 25 mg/kg (maximum 75 mg) IM as a single dose.
Remarks: Due to the large net benefit with treatment, good practice dictates that neonates should be treated for gonococcal conjunctivitis. The choice of treatment may depend on the cost and quality of the medicine in different settings and on equity considerations. Side-effects should be monitored in neonates.
For all neonates, the WHO STI guideline recommends topical ocular prophylaxis for the prevention of gonococcal and chlamydial ophthalmia neonatorum.
For ocular prophylaxis, the WHO STI guideline suggests one of the following options for topical application to both eyes immediately after birth:
tetracycline hydrochloride 1% eye ointment
erythromycin 0.5% eye ointment
povidone iodine 2.5% solution (water-based)
silver nitrate 1% solution
chloramphenicol 1% eye ointment.
Remarks: Recommendations 5 and 6 apply to the prevention of both chlamydial and gonococcal ophthalmia neonatorum. Cost and local resistance to erythromycin, tetracycline and chloramphenicol in gonococcal infection may determine the choice of medication. Caution should be taken to avoid touching eye tissue when applying the topical treatment and to provide a water-based solution of povidone iodine.
DO NOT USE ALCOHOL-BASED POVIDONE IODINE SOLUTION.
We point out that the single dose schemes should be restricted only to acute forms, not to complicated ones. In chronic, extragenital or disseminated infections, the therapy should not be less than 10 days. There are no alternative schemes for patients infected with HIV or with AIDS.
In male gonococcal urethritis the cure criterion is eminently clinical by the regression of signs and symptoms. Endocervix, anal canal and pharynx culture or methods of molecular biology should be carried out 7 days after treatment.
7.1.8 Complications
Men: Balanoposthitis, littritis, cowperitis, prostatitis, epididymitis and stenosis of urethra.
Women: Bartholinitis, salpingitis, pelvic inflammatory disease (PID), pelviperitonitis and perihepatitis.
The disseminated gonococcal infection is rare occurring in 0.3–3% of cases and affects mainly the skin (dermatitis), joints (arthritis) and, less frequently, the heart valves (endocarditis) and the meninges (meningitis).
7.1.9 Differential Diagnosis
Men: Non-gonococcal urethritis (Chlamydia trachomatis, Mycoplasma sp., Ureaplasma urealyticum or Trichomonas vaginalis), chemical urethritis (by the introduction of irritant substances in the urethra with prophylactic or curative purposes); traumatic urethritis (habit of compression of the penis); testicular torsion or tumor in men in pain in this region.
Women: Endocervicitis, bartholinitis and chlamydial salpingitis.
7.1.10 Observations
Therapeutic failure can occur with any therapeutic scheme due to bacterial resistance.
The transmission risk for men’s partners with urethral gonorrhea is of 90–97%; in affected women partners there is a risk of 50–60%.
In case of persistence of signs and symptoms after male gonococcal urethritis correct treatment, a chlamydial infection should be investigated. The permanence of the process should exclude trichomoniasis as there are coinfection reports of 5–10% of cases.
Infectious arthritis processes in young adult have in gonococcus and in Chlamydia major etiological agents.
7.2 Infections with Chlamydia Trachomatis
7.2.1 Synonymy
Non-gonococcal urethritis, NGU, cervicitis, pelvic inflammatory disease, PID.
7.2.2 Concept
The STD that exposes itself in the way of urethritis, endocervicitis, subacute ophthalmia or PID.
7.2.3 Incubation Period
Two weeks, and may extend up to a month or more.
7.2.4 Etiological Agent
Chlamydia trachomatis strains D, E, F, G, I, J and K are obligatory intracellular parasites bacteria, mainly of cylindrical epithelial cells. They multiply within inclusions vacuoles leading to cell lysis in 72 h. Only develops in cell culture such as McCoy cells. Due to the small size and growth only in cell element, Chlamydiae were confused with viruses for a long time.
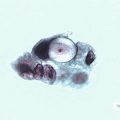
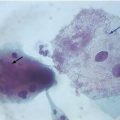
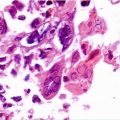
7.2.5 Clinical Manifestations (Figs. 7.3, 7.27)
Men: Urethritis with clear and mucoid secretion, rarely purulent, accompanied by mild or moderate dysuria is the main symptom.
Women: Endocervicitis with cervical mucus similar to the male urethritis, which, by the way, can also occur in females. Symptoms of ectropion and friability with cervical mucosa easy bleeding are not rare.
However, more than half of men and women infected with Chlamydia is asymptomatic or oligosymptomatic.
7.2.6 Laboratory Diagnosis (Figs. 7.61–7.66)
Only those who think and search for Chlamydia will find the diagnosis. Material should be collected through swab from places under suspicion, mainly urethra and cervical canal, and packaged according to the laboratory kit standards. If PCR or hybrid capture were used, the first urine (male or female) and vaginal/endocervical secretion, in women, are the materials of choice. Materials for molecular biology techniques can be collected by health professionals or by self-collecting, especially the first urine of the day.
The serology is only indicated in cases of invasive or complicated diseases, as salpingitis, arthritis, pneumonia or lymphogranuloma venereum. Serologies will be considered positive when equal to or greater than 1:32 and only if Elisa-based synthetic peptides derived from MOMP show no cross-reactivity. Culture is currently restricted to scientific research centers.
The conventional or liquid medium colpocitology of endocervical canal material presenting change compatible with chlamydial infection, in our opinion should be appraised. This is very different from encouraging the research of Chlamydia infection using such methodology.
Evaluation of Laboratory Methods
Exam | Sensitivity % | Specificity % |
|---|---|---|
Cytology, Giemsa | 45 | 95 |
Cytology, Papanicolaou | 62 | 96 |
Elisa assay | 70–80 | >99 |
Immunofluorescence | 80–92 | >99 |
PCR, Hybrid capture | 85–95 | >99 |
Serology | 40–50 | 85 |
Treatment and Control
CDC (2015) [2] | WHO (2016) [3] | ||
|---|---|---|---|
Uncomplicated genital chlamydia | Recommended scheme | – Azithromycin 1 g, orally, single dose; or | – Azithromycin 1 g, orally, single dose; or |
– Doxycycline 100 mg, orally, 12/12 h, for 7 days | – Doxycycline 100 mg, orally, 12/12 h, for 7 days | ||
Alternative scheme | – Erithromicin 500 mg, orally, 6/6 h, for 7 days; or | – Tetracycline 500 mg, orally 6/6 h, for 7 days; or | |
– Erythromycin ethylsuccinate 800 mg, orally, 6/6 h, for 7 days; or | – Erithromicin 500 mg, orally, 6/6 h, for 7 days; or | ||
– Levofloxacin 500 mg, orally, single dose for 7 days; or | – Ofloxacin 200 mg, orally, 12/12 h or 400 mg, orally, daily single dose, for 7 days | ||
– Ofloxacin 300 mg, orally, 12/12 h, for 7 days | |||
Anorectal chlamydial infection | Recommended scheme | Doxycicline 100 mg, orally, 12/12 h, for 7 days; or | |
Azithtomycin 1 g, orally as a single dose | |||
Genital chlamydial infection in pregnant women | Recommended scheme | Azithromycin 1 g orally in a single dose | Azithromycin 1 g orally as a single dose; or |
Amoxicillin 500 mg, orally, 8/8 h, for 7 days; or | |||
Erythromycin 500 mg, 6/6 h, for 7 days | |||
Alternative scheme | Amoxicillin 500 mg orally 8/8 h for 7 days; or | ||
Erythromycin base 500 mg orally 6/6 h for 7 days; or | |||
Erythromycin base 250 mg orally 6/6 h for 14 days; or | |||
Erythromycin ethylsuccinate 800 mg orally 6/6 h for 7 days; or | |||
Erythromycin ethylsuccinate 400 mg orally 6/6 h for 14 days | |||
Ophthalmia neonatorum | Recommended scheme | Erythromycin base or ethylsuccinate 50 mg/kg/day orally divided into 4 doses daily for 14 days* | Azithromycin 20 mg/kg/day orally, one dose daily for 3 days, over erythromycin 50 mg/kg/day orally, in four divided doses daily for 14 days |
Alternative scheme | Azithromycin suspension, 20 mg/kg/day orally, 1 dose daily for 3 days* | ||
*An association between oral erythromycin and azithromycin and infantile hypertrophic pyloric stenosis (IHPS) has been reported in infants aged <6 weeks. Infants treated with either of these antimicrobials should be followed for signs and symptoms of IHPS |
In the complicated or upper genital tract illness (endometritis, salpingitis, epididymitis, arthritis, etc.), the use of Doxycycline 100 mg, O, 12/12 h during 21 days is recommended.
New exams in the control of cure are not necessary, unless the symptoms do not regress or there is a great possibility of reinfection.
For all neonates, the WHO STI guideline recommends topical ocular prophylaxis for the prevention of gonococcal and chlamydial ophthalmia neonatorum.
For ocular prophylaxis, the WHO STI guideline suggests one of the following options for topical application to both eyes immediately after birth:
tetracycline hydrochloride 1% eye ointment
erythromycin 0.5% eye ointment
povidone iodine 2.5% solution (water-based)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree