(1)
Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil
4.1 Synonyms
Chancroid, simple chancre, ulcus molle, Ducreyi chancre, soft chancre.
4.2 Concept
Acute, localized, phagedenic and autoinoculable STD.
4.3 Incubation Period
From 2 to 5 days. Longer periods are rare.
4.4 Etiologic Agent
Haemophilus ducreyi: a Gram-negative coccobacillus, a facultative anaerobe that is grouped in pairs and difficult to cultivate in artificial media.
4.5 Clinical Presentation (Figs. 4.1–4.25)
Ulcerative lesions, generally multiple, with irregular borders and containing pus and a base with a soft consistency when long, phagedenic, painful and autoinoculable, generally accompanied by unilateral inguinal adenitis (buboes), which in 30–50% of cases develops to suppuration through a single orifice.
It occurs more frequently in men on the frenulum and the balanopreputial groove, and in women on the furcula and the inside of the small and large vulval lips.
It is predominant in men, with 40 cases for each case found in women.
4.6 Laboratory Diagnosis
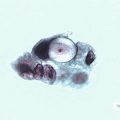
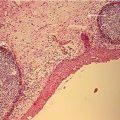
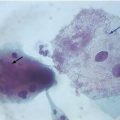
Direct examination of lesions: bacterioscopy of a swab taken from lesions using the Gram technique. It is recommended that excess pus must be removed before samples are collected from the borders of the lesion. Smear should be prepared by wiping in one direction so as not to alter the arrangement of the bacteria (Figs. 4.26–4.28).
Culture: this should be prepared immediately after collection of the sample. The best results are obtained from samples taken from buboes, when these are present and are ruptured. This bacteria is difficult to isolate, and a Nairobi, Johannesburg or enriched chocolate agar medium should be used.
Multiplex PCR (M-PCR): highly sensitive and specific method of diagnosis. This also allows simultaneous detection of Treponema pallidum and HSV-1 and -2.
Other exams with varying specificity and sensitivity, still not commonly used in daily medical practice include: immunofluorescence (IF), research-based NAAT (nucleic acid amplification test), serological screening and spectrometry methods.
4.7 Evaluation of Laboratory Methods (Lewis, DA—modified)
Exam | Sensitivity% | Specificity% |
|---|---|---|
Gram | 5–63 | 51–99 |
Culture | 35–91 | >94 |
PCR | 56–100 | 52–100 |
IF | 89–100 | 63–81 |
Enzyme immunoessay serology—(various methods) | 48–100 | 23–90 |
4.8 Treatment and Control of Cure
Antibiotic | Dose | Frequency | Duration | Method of administration | Reference |
|---|---|---|---|---|---|
Azithromycin | 1 g | Single dose | – | Oral | CDCb; EGc |
Ceftriaxone | 250 mg | Single dose | – | Intramuscular | CDC; EG |
Erythromicin | 500 mg | 8/8 h | 7 days | Oral | CDC |
Ciprofloxacina | 500 mg | 12/12 h | 3 days | Oral | CDC |
Longer-term treatment regimens are recommended in patients that are also infected with HIV.
Clinical studies using thiamphenicol, spectinomycin and fleroxacin have demonstrated satisfactory results.
In cases of soft chancre, control of cure is prominently clinical.
4.9 Complications
Local deformities and sequelae resulting from the healing process.
4.10 Differential Diagnosis
Hard chancre, herpes simplex (principally in patients with immunosuppression), lymphogranuloma venereum, donovanosis, traumatic erosions and secondary infections.
4.11 Main Differences between Hard Chancre and Soft Chancre
Hard chancre (primary ulcer, chancre) | Soft chancre (Chancroid) |
|---|---|
Incubation period—21 to 30 days | Incubation period—2 to 5 days |
Generally a single lesion | Generally multiple lesions |
Erosion or ulceration | Ulceration |
Hard base (lymphocytic infiltration) | Soft base (purulent reaction) |
Clean, erythematous, serous base | Dirty, purulent, irregular base |
Flat borders | Undermined borders |
Non-inflammatory, painless, multiple and nonfistulizing bilateral adenopathy occurring in almost 100% of cases | Inflammatory, painful and single unilateral adenopathy, fistulizing through a single orifice, in 30–60% of cases |
4.12 Observations
This disease does not have a high incidence or prevalence and a general decline in recorded cases of chancroid has been observed, above all in developed countries.
Soft chancre may be an important factor in the acquisition and transmission of HIV. As well as the facilitating role that genital ulcers play, H. ducreyi infection recruits CD4 lymphocytes and macrophages to the infected region, exposing HIV target cells to contamination.
This diagnosis should be considered even when just one ulcerative lesion is present.
This diagnosis is much more common in men than in women.
Coinfection with hard chancre (syphilis) is reported in around 5% of cases and is known as Rollet’s chancre. In these cases, soft chancre symptoms are observed at first followed by hard chancre symptoms.
Patients who wash their genitals before their consultation may undermine the effectiveness of bacterioscopic diagnosis, especially if they use antiseptic products such as povidone-iodine or chlorhexidine.
Fig. 4.1
(a) 58-year-old patient presenting an extensive ulcerative lesion containing a large quantity of purulent discharge and relatively serious painful symptoms. He reported having a fixed sexual partner, but that he occasionally liked to have sexual relations with prostitutes. The frequency of this turned out to be twice a week, or in other words it was routine behavior. He reported not using condoms, but simply washing his penis well after sex. According to the patient, these lesions appeared 1 week after having sex with a neighbor (arrow). He said that this woman was married. In the close up, a small pustule can be observed close to the urethral meatus. (b) During the healing process: photograph taken a week after treatment (single-dose oral thiamphenicol 5 g). (c) The area healed completely after treatment. The patient did not report any side-affects. He mentioned noticing an improvement 24 h after taking the medication

Fig. 4.2
Case of soft chancre involving multiple ulcers. Purulent discharge cannot be seen as the patient cleaned his penis with toilet paper, water and soap in the bathroom before the consultation. This makes direct or cultural bacteriological examination more difficult

Fig. 4.3




In this case, a noticeable characteristic of soft chancre can be observed: autoinoculability. In the past (until the 1970s) some doctors attempting to make a soft chancre diagnosis tried to demonstrate this characteristic in the following way: they removed the purulent discharge from the genital lesion and used a small needle to scarify the skin in the deltoid region, inoculating the secretion from the genital lesion in this area. They covered the skin with a watch-glass and after five days they looked for a typical soft chancre lesion. Some more rigorous doctors took a swab of the secretion using the Gram technique to look for coccobacillus grouped in chains, characteristic of infection by H. ducreyi. Perhaps these doctors were trying to identify the disease according to Koch’s Postulates
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
