(1)
Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil
3.1 Synonyms
Febrile herpes.
3.2 Concept
Herpes is an infectious and contagious disease subject to recurrence. It may be transmitted through sexual relations or in the birth canal in infected mothers. In many cases the source of contamination is not defined.
3.3 Incubation Period
The incubation period is from 1 to 26 days (average of 7 days) after contact.
Contact with ulcerated or vesicular lesions is the most common form of transmission, but this may also occur in asymptomatic patients. In many cases, the incubation period can be longer and hard to define.
3.4 Etiologic Agent
Herpes simples is caused by two antigenic types of Herpes simplex virus: HSV-1 and HSV-2.
HSV-1 occurs more frequently in lesions of the lips, the face and areas exposed to sunlight. HSV-2 predominates in the genital region.
These are DNA viruses that are thermolabile and sensitive to ether, phenol and formaldehyde and are partially inactivated by ultraviolet radiation. They have a high resistance to cooling.
3.5 Clinical Presentation (Figs. 3.1–3.54)
Initial outbreak: Preceded by subjective symptoms. The initial outbreak appears in about 24 h, including erythema, burning, itching and pain. Grouped vesicles appear on the erythematous base, which remain for 4–5 days and then recede. The whole process lasts from 2 to 3 weeks. The first symptoms to the genitalia may be accompanied by fever, headache, malaise and myalgia. Inguinal or femoral lymphadenopathy occurs in 75% of cases.
Recurrent infection: As HSV remains latent in the myelin sheath of peripheral nerves, new outbreaks can be expected. These are less intense than the first occurrence. Lesions are generally larger and more painful in patients with AIDS or other immunosuppressive diseases.
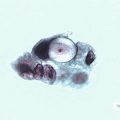
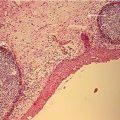
3.6 Laboratory Diagnosis Tests: Figs. 3.55–3.63
Samples collected by swabbing the lesions (preferably from the base of the vesicles) can be referred for the following tests:
- (a)
Cytodiagnosis (Papanicolaou or Giemsa).
- (b)
Cell culture.
- (c)
Molecular biology (PCR).
- (d)
Histopathological exams may be used in cases of extensive or chronic ulceration. During the active phase, serological screening reveals increased levels of IgG.
Evaluation of laboratory methods
Exam | Sensitivity % | Specificity % |
|---|---|---|
Tzanck Test | 40–50 | >99 |
Papanicolaou | 30–40 | >95 |
Direct IF | 70–80 | >95 |
Viral culture | 25–90 | >95 |
PCR | >95 | >95 |
- (e)
Serology.
Should be used antibody based tests in G glycoprotein that is more specific type (100% sensitivity and specificities of 98% [HSV-1] and 96% [HSV-2])
Type specific serological tests may be requested when:
- 1.
recurrent genital symptoms or atypical symptoms with negative cultures.
- 2.
A clinical diagnosis of HSV without confirmation.
- 3.
Partner (s) with genital HSV.
- 4.
Consider yet for: people with STD, HIV and MSM with risk behavior.
3.7 Treatment
Table 3.1
Therapeutic regimens
Antiviral | Dosage | Frequency | Duration | Route of administration |
Treatment of first infection | ||||
Aciclovir | 400 mg | 8/8 h | 7–10 days | Oral administration |
Aciclovir | 200 mg | 4/4 h (5×/day) | 7–10 days | Oral administration |
Famciclovir | 250 mg | 8/8 h | 7–10 days | Oral administration |
Famciclovir | 1 g | 12/12 h | 7–10 days | Oral administration |
Treatment of recurrences | ||||
Aciclovir | 400 mg | 8/8 h | 5 days | Oral administration |
Aciclovir | 200 mg | 4/4 h (5×/day) | 5 days | Oral administration |
Aciclovir | 800 mg | 12/12 h | 5 days | Oral administration |
Aciclovir | 800 mg | 8/8 h | 5 days | Oral administration |
Famciclovir | 125 mg | 12/12 h | 5 days | Oral administration |
Famciclovir | 1 g | 12/12 h | 1 day | Oral administration |
Famciclovir | 500 mg single dose followed by 250 mg 12/12 h for 2 days | Oral administration | ||
Valaciclovir | 500 mg | 12/12 h | 5 days | Oral administration |
Valaciclovir | 1 g | 1×/day | 5 days | Oral administration |
Valaciclovir | 500 mg | 12/12 h | 3 days | Oral administration |
Suppression treatment | ||||
Aciclovir | 400 mg | 12/12 h | Up to 6 months | Oral administration |
Famciclovir | 250 mg | 12/12 h | Up to 1 year | Oral administration |
Valaciclovir | 500 mg | 1×/day | Up to 1 year | Oral administration |
3.8 Other Medication
Some drugs such as trifluorothymidine, vidarabine and cidofovir may be used in specific cases.
Pritelivir, a HSV helicase-primase inhibitor, demonstrates anti-viral activity in vitro and in animal models infected with the herpes simplex virus (HSV). This drug has been tested, using a placebo as a comparison, to verify its efficacy and safety in healthy people with a HSV-2 genital infection. The study was randomized and included 156 HSV-2-positive individuals. The authors of the study concluded that pritelivir reduces levels of genital excretion of HSV and the number of days that lesions lasted, depending on the dose applied, in healthy men and women with genital herpes. We still do not know anything about this drug’s commercial availability.
As a result of its properties (analgesic, anti-inflammatory and antiviral), the phytotherapeutic drug Uncaria tomentosa (Imunomax®) is indicated, in gel form containing 50 mg/g, to be applied topically to herpetic lesions three times a day until they improve or heal.
3.9 Complications
Infection of the central nervous system (meningitis/encephalitis) or disseminated disease.
Neonatal infection occurs frequently with visceral and central nervous system involvement. Around 70% of newborns infected with neonatal herpes are born of mothers that are asymptomatic at the time of labor.
In addition to congenital abnormalities such as hydranencephaly and chorioretinitis, fetal abnormalities can include miscarriage, premature birth and intrauterine growth restriction in cases of vertical transmission (mother-baby).
Factors that increase the chances of intrauterine transmission include: initial outbreak of the disease present in the mother, multiple herpetic lesions, premature rupture of membranes and introduction of electrodes for fetal monitoring in pregnant women with a history of recurrent genital herpes.
It has been observed that suppression therapy with 400 mg of acyclovir every 8 h from the 36th week of pregnancy and elective cesarian section significantly reduce the chances of infection of the baby in cases of mothers with recurrent herpes.
Recurrent herpes simplex is associated with the development of recurrent erythema multiform. HSV-1 is more commonly associated with hypersensitivity phenomenon.
3.10 Differential Diagnosis
Hard chancre, soft chancre, traumatic exfoliation, genital erythema multiforme and genital canker sores associated with AIDS.
3.11 Observations
In many cases a clinical diagnosis can be made.
In our experience, genital herpes is the most common diagnosis of an infectious disease when the presenting symptom is a genital sore, and that these even more common than syphilis lesions. However, this may vary according to region and community. An awareness of the prevailing epidemiologies of the surrounding area is therefore essential to good medical practice.
Wounds in anus should also be considered in the evaluation for HSV diagnosis. The same must be said for recurrent wounds (with vesicles or not) of the skin of buttocks, of thighs root.
Cesarian birth is recommended in cases of genital lesions or if these have been present up to 1–2 weeks before the birth, especially if these were part of the initial outbreak of the disease. However, the availability of practical and safe conditions for the carrying out of this procedure should always be considered.

Fig. 3.1
Patient presenting the typical symptoms of genital herpes: grape-like grouped vesicles to the external genitalia (arrow)

Fig. 3.2
For etiological diagnosis of infection by herpes simplex, puncture the vesicle with a finely-gauged needle, taking care to open it laterally. This will avoid any bleeding, as the base of the lesion will not be punctured. Carefully lift up the skin of the vesicle exposing the base. Gently scrape it with a wooden spatula, then prepare a smear on a glass slide for posterior cytological analysis

Fig. 3.3
This case had the same presenting symptoms as the case above. If diagnosis is performed using cytology, the Tzanck test can be used where the slide is left to air dry, using the Giemsa staining technique. If the Papanicolaou technique is chosen, the slide must be quickly introduced into the flask (the same used for PAP) containing a fixative (alcohol or an equal parts solution of alcohol and ether). Other fixatives (in liquid or spray form) may also be used, such as carbowax

Fig. 3.4
Male patient with a single vesicle lesion to the body of the penis. He claimed to have had similar symptoms on two previous occasions in the last 12 months. The ideal method for the collection of material from the base of the lesion is to break the vesicle and scrape the base with a wooden spatula, whether for staining cytology or for molecular biology testing (PCR or hybrid capture). In this particular case, as the lesion was very small, we opted to collect a sample using the imprint technique, in which the vesicle is opened and a glass slide is applied in blotting movements
Fig. 3.5
A 14-year-old HIV-positive patient with severe symptoms of genital herpes and an intense secondary infection in the genital lesions (a) and the inguinal region (b). People with HIV or any other immunosuppressive disease often present more severe symptoms in terms of number, size and time before remission
Fig. 3.6
Female patient with symptoms of recurrent genital herpes (sic—according to information provided by the consultant), but who did not undergo any kind of testing to confirm this diagnosis. Observe the grouped vesicles on the left labia majora with signs of secondary infection. Some vesicles were already ruptured (a). A sample was collected from the lesion using the imprint method (b). Cytology was not specific, probably due to the stage of the disease, the secondary infection and because most of the material inside the vesicles degenerates when they are ruptured for over 24 h. However, we try to establish etiological diagnosis for all of the cases that we receive
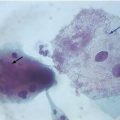
Fig. 3.7
This adolescent patient came to the clinic with her mother for a routine gynecological check-up, as she had become sexually active only a short time before (3 months). She reported just “slight” vaginal discharge, which was sometimes moderately itchy. During physical examination we observed vesicles typical of herpetic infection. Diagnosis was made using the Giemsa technique after observation of the cytopathic effect of multinucleation in a swab taken from the base of the lesion

Fig. 3.8




A young patient with vesicular lesions on a hyperemic base on the skin of the left thigh (arrows), characterizing the initial stages of a herpetic lesion. During the initial phase, symptomatology includes hyperemia and itching followed by pain after the appearance of vesicles. With the rupture of the vesicles, painful ulcers are formed. Healing begins with the formation of scabs and takes a varying amount of time, depending on if it is the initial outbreak, a recurrent outbreak, if there are any associated infections or diseases, principally HIV, or any other chronic and/or immunosuppressive comorbidities
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
