(1)
Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil
5.1 Synonyms
Inguinal lymphogranuloma, Nicolas-Favre-Durand disease, climatic bubo, the fourth disease, benign suppurative periadenitis.
5.2 Concept
Sexually transmitted disease characterized by the presence of large inguinal buboes at an advanced stage.
5.3 Incubation Period
One to two weeks.
5.4 Etiological Agent
Chlamydia trachomatis, serovars L1, L2 and L3.
5.5 Clinical Manifestations (Figs. 5.1–5.12)
The main symptom is inflamed and painful inguinal adenitis (buboes). These may be due to advanced-stage genitoinguinal or chronic genitorectal lesions.
The advanced stage may develop into multifocal fistulation, which is recognized as a “watering can” type suppuration. During this phase, a feeling of general unwellness similar that associated with a cold may occur.
The chronic phase may affect the pararectal lymph nodes, causing anal stenosis. The genital region may develop elephantiasis, fistulas and ulcers. On the vulva this is called esthiomene.
At the beginning of the outbreak, the patient often has a feeling of general unwellness, fever and loss of appetite, which can lead to weight loss.
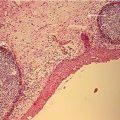
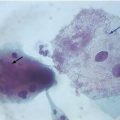
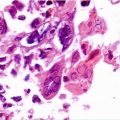
5.6 Laboratory Diagnosis
Laboratory diagnosis to confirm LGV is still substandard in developing countries, demanding of health professionals a mixture of intuition and clinical acumen. Laboratory diagnosis can be carried out via: cytology through Giemsa or Papanicolaou staining with observation of inclusion bodies (Figs. 5.18, 5.19), detection of C. trachomatis by culture in cell media, serological screening (complement fixation test, immunofluorescence, microimmunofluorescence and dose of anti-Chlamydia IgA—anti-MOMP IgA), (molecular biology (PCR) of samples swabbed from lesions or buboes. Serological screening, complement fixation test) is important if titers are equal to or lower than 1:64.
Evaluation of Laboratory Methods (Lewis, DA—modified)
Exam | Sensitivity % | Specificity % |
|---|---|---|
Giemsa | 45 | 95 |
Papanicolaou | 62 | 96 |
Elisa | 70–80 | >99 |
Immunofluorescence | 80–92 | >99 |
PCR | >95 | >99 |
Serology | 40–50 | 85 |
5.7 Treatment and Control
The therapeutic regimens recommended by the Centers for Disease Control and Prevention (CDC, 2010) and the UK National Guideline for the management of lymphogranuloma venereum (UK, 2013) are provided in the table below.
Antibiotic | Dose | Frequency | Duration | Route of administration |
|---|---|---|---|---|
Doxicycline | 100 mg | 12/12 h | 21 days | Oral |
Doxicycline | 200 mg | 24/24 h | 21 days | Oral |
Erythromycin | 500 mg | 6/6 h | 21 days | Oral |
Azithromycin | 1 g | 1× week | 3 weeks | Oral |
Other therapeutic regimens using tetracycline, minocycline and moxifloxacin are described in the literature.
Oral sulfametoxazol 800 mg + trimetoprim 160 mg, 12/12 h for 21 days.
Oral tianfenicol 500 mg, 8/8 h for 21 days.
Laboratory control exams are not required if the recommended therapeutic regimen has been concluded.
5.8 Complications (Figs. 5.13–5.17)
The difficulty of initial diagnosis of LGV or inadequate therapeutic approach may lead to complications, which include proctitis, proctocolitis sometimes imitating Crohn’s disease, fistulas, stenoses and disfiguring fibroses, vulval ulceration, stenotic proctitis and elephantiasis of the vulva (esthiomene), penis, scrotum or perineum.
5.9 Differential Diagnosis
Soft chancre, syphilis, ganglionic or vulval tuberculosis, cat scratch disease (benign lymphoreticulosis) and Hodgkin’s disease should be considered at first. Lapromatous leprosy and paracoccidiodomycosis (blastomycosis) with large inguinal masses may also be included in differential diagnosis.
5.10 Observations
Antibiotics do not have a dramatic effect on the duration of inguinal lymphadenopathy, and the sequelae associated with the chronic phase do not recede. Advanced symptoms are quickly eradicated.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree