Fig. 11.1
Interpretation of markers for hepatitis B
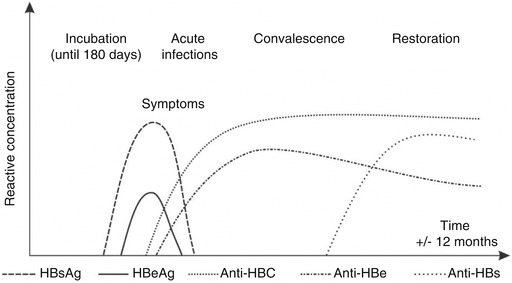
Fig. 11.2
Principal markers of hepatitis B infection and their serological expressions
Evaluation of Laboratory Methods
Exam | Sensitivity % | Specificity % |
|---|---|---|
HBsAg | 90 | 92 |
PCR | 90 | 90 |
11.1.6 Treatment
In the acute phase, treatment basically consists of support: the objective is the fastest recuperation of hepatocytes through rest, maintaining homeostasis, correcting metabolic and electrolytic disturbances, diet and symptomatic medication (avoid sedatives, diuretics and tranquilizers). Drinking alcohol is prohibited. In case of intense pruritus use anti-histamines. Antiviral treatment is recommended just for acute hepatitis B with prolonged development; in cases of ascites, accentuated icterus/cholestasis and persistent or extrahepatic manifestations; in fulminant hepatitis; in candidates for liver transplant. The regular use of corticosteroids is not recommended.
In the chronic phase, an increasing range of medication is available: interferons, lamivudine, tenofovir, adefovir, entecavir, telbivudine and other experimental drugs, as well as liver transplant. The duration of this can last from weeks to months. There are a range of therapeutic regimens, which vary according to the degree of severity, comorbidities, viral genotype and the local protocols of each country.
Active immunization (vaccine) should be carried out over three intramuscular doses (deltoid), the first within the first 12 h of life, in maternity, the second after 1 month and the third at 6 months. Adults are vaccinated in the same way (0, 30 and 180 days). Loss of dose does not mean the course has to be restarted.
A positive immunological response to the vaccine is defined as the development of hepatitis B surface antibodies (anti-HBs) at titers above 10 mIU/mL 1–3 months after the final dose. This is not recommended as a routine dose, as a response is observed in 95% of healthy vaccinated people. This is indicated for groups of people with a high risk of exposure to HBV and with immunosuppression: health professionals, homosexuals, sex professionals, partners of HBV carriers, HIV carriers, patients undergoing haemodialysis, etc. Those who do not respond should complete a second three-dose course of the vaccine. The second course is successful in around 50–70% of patients. Another approach is vaccination using a double dose, mainly in patients with immunosuppression. The regularity of this test is controversial, but it is recommended that this be carried out annually for those with chronic renal failure undergoing haemodialysis.
The need for reinforcement is also controversial. Those that benefit from this are those in which there is an indication of anti-HBs titration, as described above. In high-risk individuals (for example, health professionals), regular tests of anti-HBs levels and the use of an extra dose, where necessary, may be necessary in order to maintain immunity. Recommendations vary from country to country and from health service to health service.
Passive immunization (hyperimmune immunoglobulin—0.06 mL/kg of weight) must be carried out (even in pregnant women) up to 48 h after accidental exposure or up to 14 days, in cases where exposure is through sexual contact, and repeated after 30 days.
Concomitant vaccination should also be used according to routine dosage (use different muscular groups).
There is a range of new vaccines that have already been launched or that are being developed to improve immunogenicity and/or the convenience of administration: recombinant derived from mammal cells with antigens from the pre-S region; the combination of antigens S and C with intranasal administration; and vaccine combined with an adjuvant, such as a hepatitis A or HBV-ISS vaccine.
11.1.8 Complications
Fulminant hepatitis (0.1–1% of cases) with a mortality rate of 60%.
Chronic disease (1 to 10–90% in newborns), developing into cirrhosis of the liver or hepatocellular carcinoma in 25–40% of cases.
11.1.9 Vertical Transmission (VT)
Seroprevalence in pregnant women seen in the public health system can vary a lot. In Brazil this figure is around 1%.
Pregnant women with acute or chronic HB should be seen by an obstetrician and a clinical professional (a haematologist, gastroenterologist or infectologist).
HBsAg and HBeAg-positive pregnant women that do not receive immune prophylactic intervention present a 50–80% probability of vertical transmission (VT). In cases where the HBeAg marker is negative, the VT rate is around 10 times lower.
HB is the only viral hepatitis until today that is responsive to prophylaxis for VT (in both acute and chronic infections) if immunoprophylaxis is carried out adequately in both the mother and the newborn. Pregnant women with acute HB present increased rates of preterm labour, premature births and intrauterine growth restriction.
During hospital internment, good practice dictates that pregnant women infected with HBV (principally acute infections) are provided with individual and sanitary accommodation, just as attention to biosafety precautions should follow the same standards as for HIV infection.
The method of delivery should follow obstetric conditions and procedures that are invasive to the foetus should be avoided. The umbilical cord should be clamped as quickly as possible. In addition, the maternity team (perinatologists) should be aware of the mother’s infection in order to know what conduct to use with the newborn.
11.1.10 Differential Diagnosis
Other viral hepatitis, protozoan, bacterial, fungal, drug-induced and alcoholic hepatitis; diseases of the gall bladder and the pancreas.
Remember that there may be a coinfection/superinfection of hepatitis B with other forms that have become chronic: hepatitis C and hepatitis D. The main differential diagnosis, however, is with hepatitis C, estimated to occur in 250 million of the world’s carriers, 25% of these experiencing a progression to the symptomatic form of the disease. This disease has a prevalence of 15–20% in North American homosexual men. Detection of HCV-RNA is carried out using PCR 3 weeks after contact with the HCV virus, while anti-HCV antibodies can only be detected after 3 months.
11.1.11 Observations
Negative results for all markers: do not hesitate to prescribe a course of vaccines against hepatitis B. Many professionals forget to do this.
Vaccines contain subunits and are genetic recombinants with HBsAg as an antigenic source (they present no risk to pregnant women or patients with immunosuppression).
Do not hesitate to carry out serological screening of family members, especially for the sexual partner of the person with HBV.
Safe sex using a condom (male or female) is imperative when one of the partners has HB.
In countries with a high prevalence such as South Africa, Brazil, China, India and Russia (and many others) serological screening is recommended for all pregnant women whose serological and HBV vaccine status are unknown.
11.2 Scabies
11.2.1 Synonyms
Seven-year itch
11.2.2 Concept
Parasitic infestation of the skin caused by a mite. Transmission occurs predominantly through close contact with an infected person, and infection through clothes is rare. Sexual transmission of scabies is a possibility. It is a worldwide disease that is endemic in developing countries and cyclic in developed countries, with no preference according to gender, race or age and affecting all socioeconomic classes.
11.2.3 Incubation Period
The female creates a habitat by digging a tunnel into the skin. The male does not invade the skin and dies after mating. For 15–30 days, the female deposits from 40 to 50 eggs in the subcorneal tunnel and then dies. The biological cycle of the egg lasts for 2 weeks. Therefore, symptoms are expected to occur 3–4 weeks after infectious contact.
11.2.3.1 Etiologic Agent
Sarcoptes scabiei, variety hominis, is an arthropod from the Sarcoptidae family. It is difficult to visualize with the naked eye, has an oval-shaped body and its colour varies from grey to yellowy-brown, marked by parallel transversal grooves; it has four pairs of legs and various setae and spines. This mite can survive for up to 2–3 days in warm humid environments, increasing the potential for indirect transmission. Sarcoptes is species specific, with transmission from domestic animals (dogs, cats, pigs, horses, etc.) to humans occurring occasionally, not progressing to other individuals.
11.2.3.2 Clinical Manifestations
Itching, particularly at night, is the principal symptom. This occurs as a result of the parasite tunnelling through the skin and/or through sensitivity to the components of Sarcoptes. Lesions are most commonly found on the vesicopapules and the papules, mainly located on the abdomen, buttocks, flanks, thighs, between the fingers, in the underarms and breasts. The pathognomonic lesion is represented by the scabies burrow, which is normally winding and measures between 5 and 15 mm with a vesicle at the end (protrusion of the mite). Abrasions, pustules and nodules may also be observed (more on the genitals and covered areas).
Crusted or Norwegian scabies occurs with the presence of numerous mites and in individuals with immunosuppression or who are malnourished or infected by the HTLV-1 virus. This manifests as stratified crusts, mainly on the bony protrusions and extremities. This form is very contagious. Itching may be discreet or absent.
11.2.4 Laboratory Diagnosis
Screening for the mite and its eggs must be carried out using scarification, shaving or curettage of the lesion, particularly the mite protrusion; dilute the material in mineral oil and identify the mite using an optical microscope. Triangular structures that seem to be “hang gliding” can be seen through the dermatoscope. Biopsy with a punch of 2 mm may reveal the parasite, as well as the eggs in its tunnel, and it may be necessary to take a series of sections from the block.
11.2.5 Evaluation of Laboratory Methods
We could not find any studies containing this data. However, specialist reports state that sensitivity does not exceed 60% but specificity is over 95%.
11.2.6 Treatment and Control of Cure
The topical therapeutic options below are effective and should be applied at night for three consecutive days and repeated after an interval of 1 week. Adults should apply medication to the whole body from the neck down and children under 10 should also apply it to the scalp. A common error is to apply it just to the areas that are itching. The indiscriminate use of medications should be avoided as this may cause primary irritant dermatitis. In addition, it is not recommended that clothes and bedclothes are washed in boiling water, and these can simply be exposed to the sun or ironed. Concomitant treatment of all close family members is recommended in order to avoid reinfection, even of those who are asymptomatic. Domestic animals are not hosts of Sarcoptes scabiei, variety hominis, and therefore do not need to be treated.
Itching can be intense in some areas, particularly in the male genital region, and depending on the extent and intensity of this it can be treated with medium to high strength topical corticosteroids or systemic antihistamines in order to provide physical comfort to the patient and reduce the possibility of secondary infections via abrasions.
Permethrin lotion 5%: there are no controlled studies on the use of permethrin in pregnant or breastfeeding women (risk category B); it is contraindicated in children under 2 months old.
Deltamethrin lotion 10%: like permethrin this is a pyrethroid, a synthetic substance obtained from the esterification of chrysanthemic acid, which is extracted from the flower of the chrysanthemum (Chrysanthemum cinerariaefolium).
Crotamiton lotion 10%: approved by the FDA just for the treatment of adults and contraindicated in pregnant and breastfeeding women. This drug is less effective than permethrin.
Monosulfiram 25% in alcoholic solution: this should be diluted in water at a proportion of 1:2 (adults) and 1:3 (children); avoid alcohol for 10 days to prevent the antabuse effect.
Benzyl benzoate 25%: often irritating and can cause contact dermatitis.
Lindane lotion (gamma-hexachlorocyclohexane) 1%: a neurotoxin that should not be used in children or pregnant or breastfeeding women. Its sale has been suspended in Brazil and Europe. The FDA considers lindane to be a second-line therapy for scabies and lice.
Precipitated sulphur 5–10%: a paste prepared in water or liquid vaseline; as it is not an irritant, it is used mainly in children younger than 2 months and pregnant women.
Systemic options include:
Ivermectin tablets 6 mg: oral treatment for adults and children over 15 kg and 2 years. Contraindicated in pregnant and breastfeeding women. The recommended dose is 200 μg/kg or according to the table: 15–24 kg = ½ tablet; 25–35 kg = 1 tablet; 36–50 kg = 1½ tablets; 51–65 kg = 2 tablets; 66–79 kg = 2½ tablets; >80 kg = 3 tablets. This should be taken as a single dose at night and repeated after 1 week.
11.2.7 Complications
Secondary infections and eczematization of the lesions. In breastfeeding women and patients with immunosuppression this may affect the face, scalp, palms of the hands and souls of the feet, an area where not usually affected in adults.
11.2.8 Differential Diagnosis
Hives, impetigo, syphilitic roseola, drug allergy and other pruritic rashes; crusted scabies can be confused with psoriasis, seborrheic dermatitis and eczema.
11.2.9 Observations
There is no indication for the concomitant use of topical and systemic treatment for scabies.
Frequent scabies infection is associated with STDs.
Patients with AIDS may present atypical clinical manifestations.
It is important that all family members living in the same house are treated at the same time and that guidance is offered on better hygiene/cleanliness of the home environment (mattresses, quilts, bed sheets…).
In cases of secondary infection, topical or systemic antibiotics used principally for the treatment of streptococci or staphylococci are required.
11.3 Pediculosis Pubis
11.3.1 Synonyms
Public lice. Crabs.
11.3.2 Concept
Ectoparasitosis known for centuries, and for some this is the most contagious sexually transmitted disease. Mainly transmitted through intimate/sexual contact and occasionally through fomites.
11.3.3 Incubation Period
Although this parasite can take up to 27 days to reach the adult phase and that after fertilization egg laying can begin within around 36 h, symptoms usually start after around 1 week. All of this depends on the number of parasites transmitted and principally on the level of hygiene of the host.
11.3.4 Etiologic Agent
Pthirus pubis. This is an insect from the genus Pthirus and of the suborder Anoplura (sucking lice). It can be seen with the aid of a magnifying glass. Morphologically it has a short head embedded in a cavity in the thorax, and its abdomen, which is larger than the thorax, has six legs. The abdomen has four small elevations with various bristles. Its eggs are elongated and easily attach to hairs.
11.3.5 Clinical Manifestations
The patient’s main complaint is intense itching. Urticarial lesions, vesicles or pigmented macules (bluish = cerulean macules) may be observed as a reaction to the saliva and/or anticoagulant that the parasite injects into the dermis while it is feeding. Historically this was the transmitter of endemic typhus and trench fever, as it can transmit rickettsia and borreliosis. The parasite can affect the pubic area, underarms, beard and eyelashes.
11.3.6 Laboratory Diagnosis
Removal of hairs and examination under a microscope to identify the adult insects or viable eggs. In more serious infestations the parasite can be seen with the naked eye.
11.3.7 Evaluation of Laboratory Methods
We could not find any studies containing this data.
11.3.8 Treatment and Control of Cure
Topical and systemic treatments follow the same application criteria used for scabies. Sexual partners should be evaluated and treated at the same time.
Permethrin lotion 5%
Malathion lotion 0.5%
Benzyl benzoate lotion 25%
Lindane lotion (gamma-hexachlorocyclohexane) 1%
Solid vaseline: used to remove lice from the eyelashes; apply twice a day for 8 days.
Ivermectin tablets 6 mg: oral treatment for adults and children over 15 kg and 2 years. Contraindicated in pregnant and breastfeeding women. The recommended dose is 200 μg/kg or according to the table: 15–24 kg = ½ tablet; 25–35 kg = 1 tablet; 36–50 kg = 1½ tablets; 51–65 kg = 2 tablets; 66–79 kg = 2½ tablets; >80 kg = 3 tablets. This should be taken as a single dose at night and repeated after 1 week.
Trichotomy or physical removal of eggs attached to hairs using a fine comb.
11.3.9 Complications
Secondary infection and eczematization (rare) in very serious cases and infestation of the eyelashes, which may cause blepharitis.
11.3.10 Differential Diagnosis
Impetigo, microbial eczema, neurodermatitis, psoriasis, seborrheic dermatitis and contact dermatitis. Infestation of the eyelashes may resemble blepharitis.
11.3.11 Observations
As the incidence of other STDs is common in carriers of pediculosis pubis, the relevant laboratory investigations are necessary in order to rule out any coinfections.
In cases of secondary infection, topical or systemic antibiotics are recommended.
11.4 Molluscum Contagiosum
11.4.1 Synonyms
Water warts.
11.4.2 Concept
Disease caused by a poxvirus, characterized by the presence of a varying number of papules transmitted through direct contact with the skin. Autoinoculation can occur with new lesions appearing in other areas.
11.4.3 Incubation Period
Generally 3 weeks to 3 months after exposure.
11.4.4 Etiologic Agent
This is a poxvirus with four subtypes, with type 1 being the most prevalent. This virus has the capacity to reproduce in the cytoplasm of infected cells, provoking the appearance of cytoplasmic inclusions (Henderson-Patterson bodies).
11.4.5 Clinical Manifestations
Presence of hemispherical papules 3–6 mm in diameter that are isolated and well defined, either pink or the same colour as the skin, often with an umbilicated centre and a slightly erythematous base, more commonly found on the trunk and extremities in children and on the genitals in adults.
It is generally asymptomatic, and there may be itching or perilesional eczema. Generalized and persistent lesions may be found in patients with immunosuppression.
11.4.6 Laboratory Diagnosis
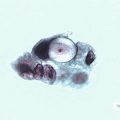
In case of uncertain diagnosis, carry out microscope investigations. Place the material obtained through curettage onto a slide, fix it with alcohol using the same method used for gynaecological examinations and request stained cytology using the Papanicolaou or Wright technique to screen for cytoplasmic inclusions.
For cytology using the Giemsa technique, leave the slide to air dry before sending it to the laboratory in a dry flask. Inclusions can also be seen via histopathological examination, but only as an exception.
11.4.7 Evaluation of Laboratory Methods
We could not find any studies containing this data.
11.4.8 Treatment and Control of Cure
Curettage of lesions as the procedure of choice.
Trichloroacetic acid 30–50% applied to lesions once a week.
Cryotherapy with liquid nitrogen: this procedure is painful but should be used on larger lesions.
Tretinoin cream 0.025–0.1%: may cause irritation to folded areas or areas exposed to the sun.
Potassium hydroxide solution 5 or 10%: applied to lesions once a day for up to a week.
Imiquimod cream 5%: applied three times a week every other night. Wash the area 8 h after each application. This should not be used by pregnant and breastfeeding women.
Systemic medication: griseofulvin and cimetidine have been cited; cidofovir and intralesional interferon have been used in patients with immunosuppression.
Specific treatment is often not necessary, as the lesions usually involute spontaneously after a few months.
11.4.9 Complications
Eczematisation, inflammation and secondary infection. Lesions on the eyelids may lead to conjunctivitis.
11.4.10 Differential Diagnosis
Acne vulgaris, prickly heat, chicken pox, basal cell epithelioma, lichen planus, milium, condyloma acuminata and other warts. In patients with AIDS, cutaneous cryptococcosis may present lesions similar to those for molluscum contagiosum.
11.4.11 Observations
Patients should be re-examined after treatment at intervals of 15 days to 2 months.
The sexual partners of adult patients should be examined it lesions are found in the anogenital region.
Atypical extragenital lesions in adults, especially on the face, suggest coinfection with HIV or other immunodeficiencies.
When lesions are observed on the genitals, some professionals often confuse them with HPV. Therefore, we believe that in some cases material from the lesions should be sent for histopathological examination.

Fig. 11.3
Traumatic lesion leading to petechiae on the junction of the hard and soft palate, contracted from performing fellatio. In this case, differential diagnosis includes herpes, other viruses and bacterial infection with streptococcus

Fig. 11.4
Ulcer on the buccal floor contracted from performing cunnilingus. Observe the sharp uneven borders of the anterior teeth. Differential diagnosis includes diseases that cause mouth ulcers, such as syphilis or herpes. In this case, as in the previous case, if the patient is HIV positive the infectiousness of the lesion will be higher. However, if the patient is HIV negative they will be more susceptible to contamination with HIV and other infections every time they practice oral sex

Fig. 11.5
Patient in her 50s referred to the STD clinic due to a genital tumour. She was very worried as she thought it was a malignant or serious venereal disease. This was simply a sebaceous cyst, which was at first treated by removal of the inner mass and then on another occasion by removal of the capsule. It is extremely important to keep in mind that we must consider STDs in our everyday practice. However, we must also remember that not everything found on the genitals is an STD. Establishing a diagnosis based on assumptions and without verifying the epidemiological history and performing thorough clinical and laboratory examinations represents low-quality medical practice. Therefore, we must follow global medical care routines in full

Figs. 11.6 and 11.7
Patient referred for peniscopy as his partner obtained oncological colpocytology results suggesting HPV. He did not present any lesion suggesting he was infected with this virus. He was diagnosed with a dermal cyst on the scrotum
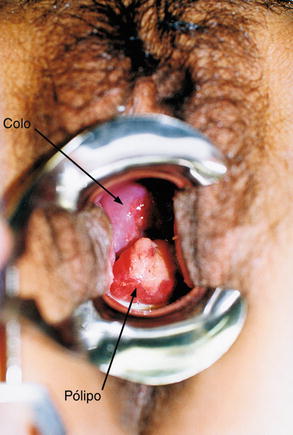
Fig. 11.8
Patient presenting large cervical polyps (arrow) that extends to the vaginal introitus. This was the reason for her referral. After a routine check up with direct examination of a vaginal swab we diagnosed vaginitis caused by Trichomonas vaginalis. Serological screening for syphilis, HIV, hepatitis B and C was non-reactive. We prescribed a course of injections against hepatitis B

Fig. 11.9
Patient referred to the Fluminense Federal University (UFF) STD clinic for treatment of bartholinitis. This was not a case of bartholinitis, but an abscess in the area close to the right labia majora. The patient reported that she had had similar symptoms on three previous occasions and that these had reduced upon local application of a stupe and antibiotic cream. Incision and drainage, as well as systemic antibiotic therapy, are the procedures that should be used to treat this. We must emphasize the fact that many of these processes start after depilation followed by folliculitis

Fig. 11.10
Twenty-six-year-old patient referred by the urology clinic presenting extensive balanitis with stinging. He reported this being the first time these symptoms had appeared. He denied receiving any previous treatment and said that the symptoms had appeared 24 h previously. Serological screening for HIV and syphilis was non-reactive. Bacteriology exams of a swab taken from the lesion using the Gram technique and dark field microscopy did not provide a clearer diagnosis. Stained cytology using the Papanicolaou and Giemsa techniques was non-specific. The patient was advised to wash using boric acid solution and topical application of Uncaria tomentosa gel 5%, which lead to complete cure within 4 days

Fig. 11.11
Patient seen at the UFF STD clinic after referral from the public health system, presenting classic symptoms of fungal balanitis (a). He reported that he sought medical attention for these symptoms and was given an IM dose of penicillin benzathine without being examined. Direct examination of a swab taken from the area did not provide a diagnosis of fungus. However, stained cytology was positive for hyphae. He was treated with itraconazol and given advice on hygiene. One week later he was fully recovered (b)

Fig. 11.12
Nineteen-year-old patient referred by a private health company for treatment of bartholinitis. The symptoms had persisted for over a week despite the use of oral antibiotics, azithromycin and ciprofloxacin. She was not experiencing fever or intense pain. She reported that the swelling did not hurt but was causing her discomfort (sic). Note in panels (a, b) that there is no inflammation. The clinical diagnosis was Bartholin’s cyst. Panels (c–f) show the marsupialisation of the gland. In (g), a drainage tube was left attached for just 24 h, as if left for longer this could facilitate a secondary infection of the gland
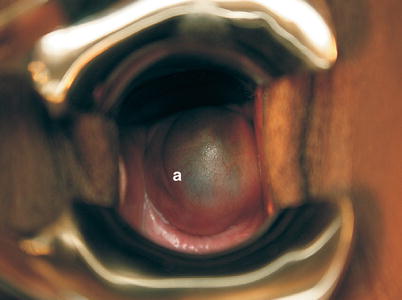
Fig. 11.13
Thirty-five-year-old patient, referred to the STD clinic at the Valença Faculty of Medicine in Rio de Janeiro by the Family Health Program (PSF) in the same city, with a history of vaginal tumours that were observed during sampling for oncological colpocytology carried out by a non-medical professional at this service. Examination carried out at the STD clinic revealed that this was a Gartner duct cyst ( a ), a disease with a low prevalence, and that it was not related to any STD. These are remnants of the mesonephric ducts on the lateral part of the vulva
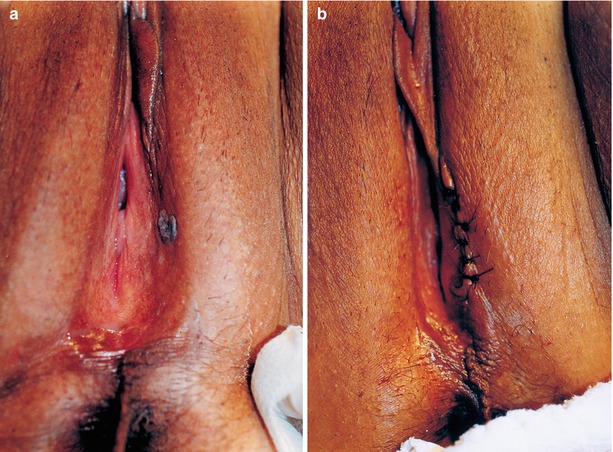
Fig. 11.14
(a) Patient presenting a vegetating lesion on the vulva that had been present for a few months and on various occasions had been treated with trichloroacetic acid solution and podophyllin, as it was thought that it was a case of condyloma acuminata. (b) After examination, we proceeded to perform surgical exeresis. Histopathology revealed this to be a case of syringoma, a benign tumour that is rarely seen on the vulva. This is understood to be an adenoma on the ducts of the intra-epidermal eccrine sweat glands
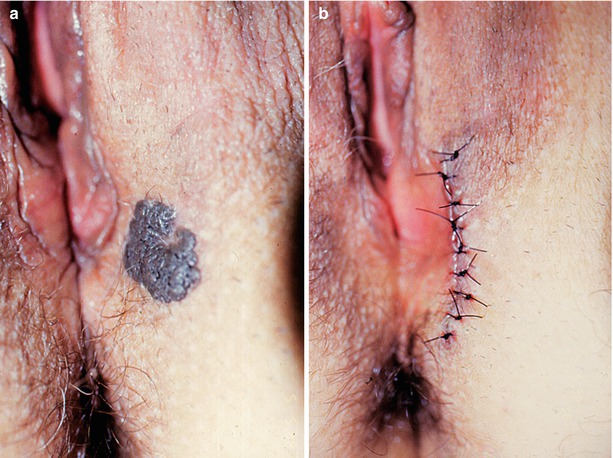
Fig. 11.15
(a) This is practically identical to the previous case. (b) This was also a case of syringoma. We consider exeresis of the tumour and histopathology to be good practice. There are both aesthetic and emotional aspects related to the presence of a lesion on the genitals. It is unusual for somebody to have a genital lesion and not think that this is associated with an STD. The previous case was worse, as the partner underwent two peniscopies to screen for HPV and it was established with certainty that he had contaminated his partner with HPV

Fig. 11.16
Another case where histopathology was used to diagnose syringoma on the vulva

Fig. 11.17
Patient referred from a health centre after intramuscular administration of 500 mg of ceftriaxone to treat bartholinitis. She was very anxious and was complaining of pain and a tumour on her vulva. At the beginning of the consultation she denied any situation association with sexual activity. However, when there was just one doctor in the room and the patient was feeling more confident she reported that she had been raped by three men and had suffered violent injuries to her vulva. This is a learning point: many patients need time and confidence to talk about intimate details. Health teams should be careful to create an adequate environment in order to listen to their patients. Every one of us takes the time we need to speak

Fig. 11.18
This patient came to the clinic in an anxious state as he had been accused by his partner of having transmitted HPV to her. He just had some numerous sebaceous cysts on his scrotum. It is worth remembering that not everything on the genitals is an STD. It is not uncommon for a patient to receive colpocytological (PAP) results suggesting HPV and their partner not present anything. However, the complete routine should not be delayed, including serological screening and finding out the patient’s vaccination status
Fig. 11.19
(a) Patient presenting a cyst containing a serous substance on his penis. (b) Totally cured after exeresis

Fig. 11.20
Patient seen at a private health clinic referred for treatment of warts on his penis. He actually presented small vegetative verrucous lesions on his penis, which are characteristic of condyloma acuminata. Histopathological examination proved this hypothesis to be correct. During the appointment, in line with our normal routine, we examined the penis, the scrotum and the perineal and perianal regions. We found some abnormalities in this area, however, they were just sebaceous granules (a), eliminating the possibility of this being a case of HPV infection in the perianal area

Fig. 11.21
Many men present these anatomical formations on the penis (arrows). Sometimes they are iatrogenically given “treatment” for HPV. As well as physical iatrogenesis, some of these patients are affected emotionally, as they are “labelled” as having an STD that develops into cancer. These anatomical formations are physiological

Fig. 11.22
This patient presented this genital epidermal cyst and a history of recurring genital herpes
Fig. 11.23
(a, b) This patient arrived at the clinic with a case of edema on his foreskin and an ulcer on his penis. He reported that he had a cockscomb-type vegetative lesion on his penis. To cure this, he applied an unknown liquid sold by a pharmacy salesperson in his neighbourhood. He reported that soon after the first two applications the ulcer appeared, developing pain, necrosis and edema. As well as being caustic, this product caused topical irritation. We did not find out what the liquid was as the patient did not return for follow up
Fig. 11.24
(a, b) Patient referred to the STD clinic for treatment of a genital ulcer with a hypothetical diagnosis of lymphogranuloma. This was actually a case of paraphimosis. The patient claimed that it had been this way for 2 days and that when he went to the health centre he was referred to our clinic

Fig. 11.25
This is very similar to the two previous cases, although it was not paraphimosis but dermatitis caused by a primary irritant through the topical use of a solution for the treatment of mycosis. The product contained the metalloid iodine. Soon after using this medication to treat the itching caused by the mycosis, the patient noticed this severe edema

Fig. 11.26
What follows is a series of cases involving edemas on the penis with four different causes. All of these cases were seen at the STD clinic at the Federal University of Ceará University Hospital in the city of Fortaleza. The importance of anamnesis, clinical examination, classic STD laboratory examinations and an epidemiological approach are essential in deciding the therapeutic approach to be taken. (a) The edema appeared after the appearance of a genital ulcer noticed around 7 days after sexual relations with an occasional partner without protection. VDRL was 1:2 and serological screening for HIV and hepatitis B was negative. The patient was treated for syphilis and the symptoms disappeared the following week. (b) Edema on the penis that appeared after unprotected sex with his girlfriend, his exclusive partner. During the consultation he reported pain in his penis but no secretions or adenomegalies. He reported that he normally had a lot of difficulty externalizing his glans (phimosis). He was referred to the urology department and advised to apply a gold saline compress and an oral anti-inflammatory. The glans reduced in size after a urological procedure and the patient was later referred for postectomy. (c) Patient complaining of edema and an ulcer on his penis that had appeared 24 h previously. He reported that the edema had appeared after an attack of severe genital itching. He reported itching in other areas of the body and that this worsened at night. When asked if other family members had displayed similar symptoms, he said that they had. In the photo there are traumatic ulcers on the penis, glans and hand. We also found lesions on the buttocks, abdomen and underarms. We recommended treatment for scabies with oral ivermectin 6 mg, 2 pills once a week repeated after 1 week, and advised that all symptomatic family members seek medical attention. (d) Patient presenting edema on his foreskin for 3 days. He had been experiencing stinging and purulent urethral discharge for 10 days, which began 6 days after having unprotected sex. Bacteriological examination of the urethral discharge was positive for intracellular Gram-negative diplococci in polymorphonuclears. We recommended oral ciprofloxacin 500 mg and oral azithromycin 1 g, both in a single dose. We advised his to use cold saline compresses and an oral anti-inflammatory. The symptoms disappeared within 3 days
Fig. 11.27
(a, b) Young adult presenting a serious case of hypertrophy of the papillae, which can be easily confused with HPV infection. This patient had been seriously emotionally abused by their sexual partner, who accused him of having HPV

Fig. 11.28
Another case of hypertrophy of the papillae. It is obvious that in some situations the patient can present condyloma acuminata lesions in the middle of the papillae, and only these should be treated. However, care must be taken during examination to avoid causing iatrogenesis

Fig. 11.29
The same situation of hypertrophy of the papillae, also known as hirsuties coronae glandis
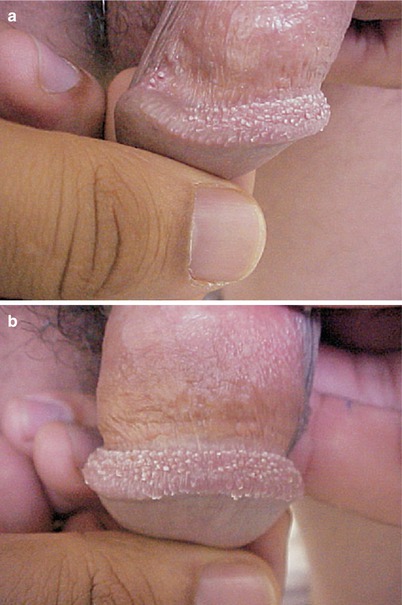

Fig. 11.30
(a–c) Hirsuties coronae glandis, which is often confused with condyloma acuminata, or HPV infection

Fig. 11.31
Another patient referred to the UFF STD clinic to treat HPV lesions. These were actually anatomical elements—Fordyce granules that have nothing to do with HPV infection. The patient insisted that he did not want to continue with this “problem”. He was given an explanation of what they are and that the best solution was to do nothing to avoid aggravating the area

Fig. 11.32
Twenty-year-old patient with a high economic and cultural level presenting hyperchromic lesions on his glans and the inside of his foreskin. The patient as well as his father, who is a health professional, requested that a biopsy of the lesion be carried out, as they wanted to confirm or exclude the possibility of HPV infection, as this hypothesis was causing them stress. Histopathological examination of a small fragment revealed that this was a case of melanocytic nevus, which is not an infectious disease and not related in any way to HPV. This was the cause of so much distress for the patient, his father and his girlfriend

Fig. 11.33
Young adult patient seen at the UFF STD clinic referred for a peniscopy as his sexual partner presented oncological colpocytology (PAP) results showing cells with koilocytosis, suggesting HPV. The patient reported that he had already been examined by a urologist who had referred him for treatment for HPV at our clinic. This situation is actually physiological (pearly penile papules in the peroneal groove and Fordyce granules, which are sebaceous glands on the penile shaft) and is in no way related to HPV infection. Guidance on sexual and reproductive health should be given. We discovered from the patient history that he had not been vaccinated against hepatitis B. Therefore, we prescribed a course of injections for this. On March 9, 2011, an excellent article was published online in Nature 471 describing alterations in human DNA that had made certain anatomical formations disappear, such as “spines” on the penis. These ridges exist in chimpanzees (and in various mammals) and increase sensitivity, making ejaculation happen faster. It is believed that these “spines” also remove the sperm of any rivals that have copulated with their mate previously. Therefore, this mechanical removal could help to ensure that pregnancy occurs as a result of the most recent coitus. On the other hand, the smoother penis of modern man may be linked to the adoption of monogamous relationships. Without these anatomical formations, man has made coitus last longer. Who knows, perhaps the formation of pearly penile papules/Fordyce granules/hirsuties coronae glandis are remnants of these old penile “spines”?
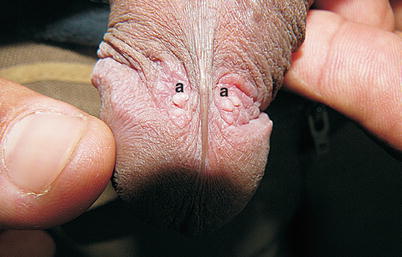
Fig. 11.34
Twenty-one-year-old single patient, a student, seen at the STD clinic of the Federal University of Ceará University Hospital in Fortaleza, complaining of genital warts he had suffered from for around 4 years. He reported having just one sexual partner in the last 2 years. He did not report any previous STDs. Examination of the genital area (peniscopy) after application of acetic acid 5% did not reveal any lesions suggesting HPV or any other infectious agent. He was informed that this was not an STD and that it was simply an enlargement of the glands in this region (a). Unfortunately, cases like this are sometimes “diagnosed and treated” as thought they were HPV infection. As well as physical trauma (to the local area), people can undergo significant emotional, social and marital stress, etc.

Figs. 11.35 to 11.38
Pearly penile papules. These are normal anatomical structures situated on the edge of the glans (the corona) or on the frenulum (arrow). They are common, with a reported incidence in 19% of the population. These are isolated skin-coloured papules that are 1–2 mm in diameter and form a circle on the edge of the glans, sometimes with a keratotic (spiculated) surface, and are often misdiagnosed as molluscum contagiosum or condyloma acuminata. They have a regular appearance resembling a riverbed covered in pebbles, which is different to condyloma acuminata. Both conditions can take on a whitish appearance after application of acetic acid. Histology reveals the lesions to be angiofibromas. No treatment is required. In Fig. 11.37, although the patient’s skin is black, the papules are very white and prominent. He reported difficulty in explaining to his partner that this was anatomically normal and was not a disease. In extreme cases, exeresis is recommended for emotional and aesthetic reasons

Fig. 11.39
Vestibular papillomatosis was given various names in the past, including terms such as vulvar papillomatosis and microwarts. The term vestibular papillomatosis was recently established by the International Society for the Study of Vulvovaginal Disease (ISSVD). Vestibular papillomatosis is described as small papular projections that are generally located on the posterior part of the vestibule, and is considered to be a normal anatomical variant. Vestibular papillomatosis is quite normal. Stimulated by hormones during puberty, in some women a prominently thick rough surface can be found on the labial epithelium. This condition is very common in the second and third trimesters of pregnancy. These structures can be seen in asymptomatic women who generally complain of itching or burning, associated particularly with coitus. Its clinical relevance is controversial. In some cases vestibular papillomatosis may be associated with HPV infection. In cases of vulvovaginal infection, these structures can increase in volume. Secretions in the vaginal introitus can also be completely physiological. This was the case here.
11.5 Behçet’s Disease
11.5.1 Concept
Inflammatory disease with primary vasculitis affecting various systems and causing oral aphthous ulcers (always), recurring genital ulcers, uveitis, retinal vasculitis and skin lesions. It can also lead to arthritis, neurological alterations and thrombophlebitis.
11.5.2 Etiological Agent and Epidemiology
It has unknown etiology but is related to the presence of HLA-B51 and commonly found in populations in the Mediterranean and Middle East. It is prevalent in Turkey, Iran, Iraq, Saudi Arabia, Japan and South Korea. It mainly affects young men (from 20 to 40 years). Secondary immunological abnormalities towards bacterial and viral antigenic stimuli may be associated with its etiology.
11.5.3 Clinical Manifestations
Diagnosis follows the criteria established by the International Study Group for Behçet’s Disease (Table 11.1), with the obligatory presence of one major criterion and two minor criteria.
Table 11.1
Criteria by the International Study Group for Behçet’s disease
Major criteria | Clinical picture |
|---|---|
• Recurring oral ulcers | Small, large or herpetiform aphthous lesions, observed by the doctor or the patient, recurring at least three times over the period of a year |
Minor criteria | |
• Recurring genital ulcers | Aphthous ulceration or scarring observed by the doctor or the patient |
• Ocular lesions | Anterior or posterior uveitis or retinal vasculitis |
• Cutaneous lesions | Erythema nodosum, papulopustular or pseudofolliculitis-type lesions, or acneiform eruptions |
• Positive pathergy test result | Formation of a papule, 2 mm or larger, within 24–48 h of intradermal insertion of a needle in the forearm |
The genital ulcers are painful, and in women may require fenestration of the labia.
11.5.4 Laboratory Diagnosis
Eminently clinical. IL-10 values are related to the intensity of clinical manifestations.
11.5.5 Treatment and Control of Cure
Genital lesions are treated with topical local injectable corticosteroids. This disease is recurring and may require systemic treatment with corticosteroids or immunosuppressants.
11.5.6 Differential Diagnosis
Differential diagnosis includes mouth ulcers, recurring aphthous stomatitis, herpes, syphilis, bullous pemphigoid, pemphigus, Crohn’s disease and lymphogranuloma venereum, among others.
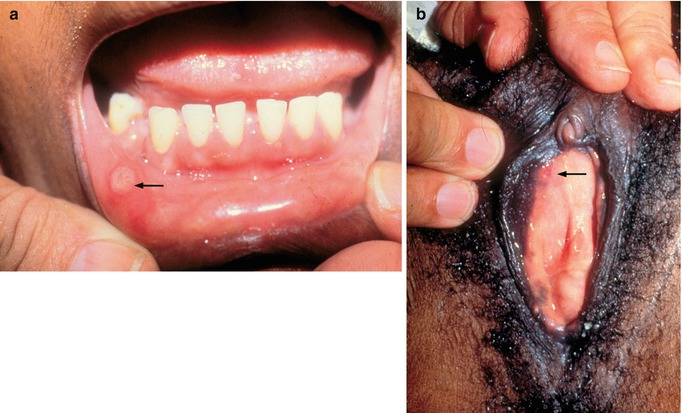

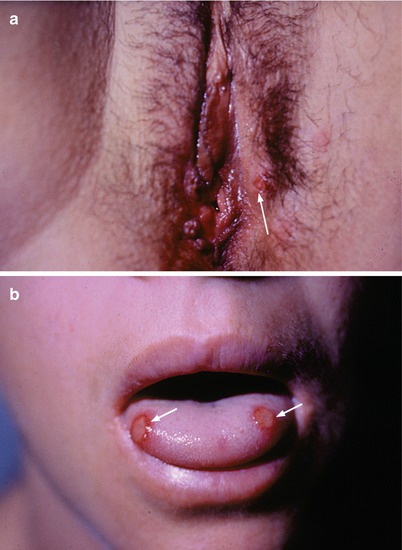
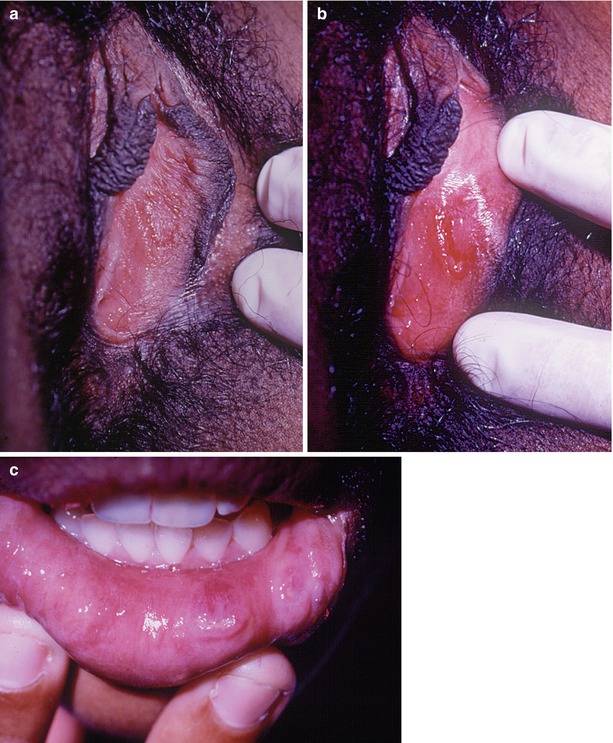
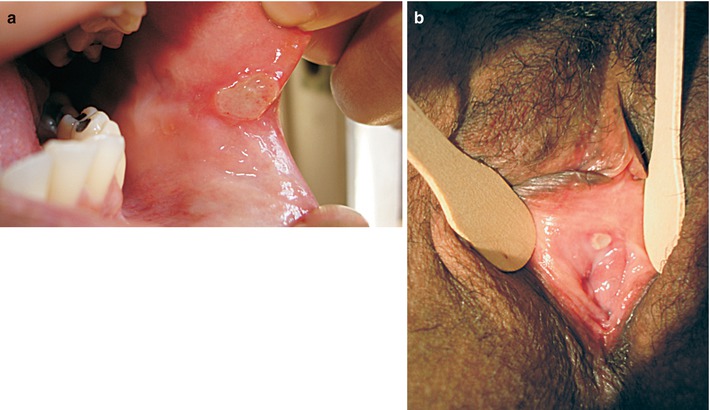
Fig. 11.40
(a, b) Patient over 50 years old presenting a minor case of Behçet’s disease, or Behçet’s syndrome (arrow)
Fig. 11.41
(a, b) Behçet’s syndrome. Young patient with a well-confined chronic ulcer with raised borders and a clean base. This was a very painful lesion. Serological screening for syphilis and HIV was negative, as was bacterioscopy of the lesion. It was treated with a corticosteroid after many treatments, including the syndromic approach for ulcers, but with no success. (c) While examining the oropharynx, we noticed a small ulcer on the palate, over to the left, which was visible after removal of the patient’s superior prosthetic denture. The patient did not present iritis uveitis, which is part of the triad of symptoms associated with Behçet’s syndrome
Fig. 11.42
Behçet’s ulcer (arrow). Unfortunately, many patients only receive correct diagnosis after initial approaches to treat STD ulcers have been applied
Fig. 11.43
(a, b) Vulvar and oral lesions associated with Behçet’s disease (arrow)
Fig. 11.44
(a–c) Another case of orogenital Behçet’s syndrome. Normally diagnosis is not simple and almost always a number of unsuccessful treatments are attempted with no success. Recurrence is a constant factor
Fig. 11.45
(a, b) Although considering Behçet’s Syndrome could be the classic approach, this case does not fit in with this kind of clinical picture. The patient reported that this was the third time that this problem had occurred. It was not possible to establish the etiology and the lesions disappeared after a week without the patient using any medication. All routine examinations were negative. In 2 years of follow up the patient did not present any recurrence
Fig. 11.46
(a, b) Perineal amyloidosis. Vegetative genital lesions are frequent, however etiological elucidation can be difficult as it involves clinical aspects that are unknown to gynaecologists. A 57-year-old white female smoker who had been pregnant eight times, given birth twice and undergone two abortions and had started her menopause at 48, was referred to the UNICAMP (Campinas University) Gynaecology Clinic after having been evaluated by various professionals, including a dermatologist and an oncologist, with no diagnosis being established. She presented two prominent violet-coloured lesions with a soft and fleshy consistency and a small inner haemorrhagic area, measuring approximately 2 cm and 5 cm respectively, stretching from the furcula to the left gluteal fold. The lesions were pruritic and presented spontaneous discharge of a bloody and fetid secretion. The patient presented the following previous pathologies: diabetes, arterial hypertension and congestive heart failure, which developed after an acute myocardial infarction 5 years previously. Her symptoms included: dyspnoea, chest pain and edema of the lower limbs. She was taking NPH insulin, digoxin and furosemide. A diagnosis of eosinophilic granuloma had been suggested and two local biopsies were carried out that surprisingly confirmed a diagnosis of “primary cutaneous amyloidosis”. Electron micrographs were obtained which revealed intracytoplasmic production of filamentous deposits (amyloid) in fibroblasts. Therefore, this excluded the possibility of this being a case of precursor lesions of plasmacytic dyscrasias, as the plasmocytes did not present any relationship with the etiology of the lesion
11.6 Erythema Multiforme, Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis
11.6.1 Concept
Acute syndromes with etiologies that are not always defined, sometimes related to infections or medication, sometimes to genetic predisposition (human leukocyte antigens (HLA)), with cutaneous, mucosal and sometimes systemic lesions.
Some authors describe a spectrum of manifestations including the mildest form, erythema multiforme minor (EMm), erythema multiforme major (bullous) (EMM), Stevens-Johnson syndrome (SJS), mixed clinical presentations of SJS/TEN and the most serious form which is the highly lethal toxic epidermal necrolysis (TEN), also known as Lyell’s syndrome.
11.6.2 Etiopathogeny
This condition is defined as a standard cutaneous reaction to intolerance to a stimulus, which in mild cases (erythema multiforme) is more frequently caused by infection by the human herpes virus (HSV), and in serious cases (Stevens-Johnson syndrome and toxic epidermal necrolysis), intolerance to drugs, especially beta-lactam antibiotics, sulfonamides, allopurinol, non-hormonal anti-inflammatories and aromatic anticonvulsants. The relation of some HLAs with determined drugs gives rise to genetic predisposition. The pathogenesis is not totally clear, but it involves a cell-mediated immune reaction leading to the destruction of cells infected with HSV or cells with the antigens related to the drugs with the presence of varying degrees of apoptosis. Patients with AIDS are more frequently affected.
11.6.3 Clinical Manifestations
The oral and genital mucosae are often affected across the whole spectrum of these different clinical presentations, with the skin being affected in the majority of cases. This can involve a range of cutaneous lesions: erythematous patches, target lesions (central purpuric patch surrounded by a pale raised halo and a peripheral erythema), epidermal detachment and blisters, which may be extensive in TEN, similar in appearance to a large burn. Exulcerations and pseudomembrane formations with ophthalmological, oropharyngeal-esophagial, laryngeal-tracheal-bronchial and genital (balanitis and vulvovaginitis) legions predominate on the mucosa, sometimes developing synechiae, particularly in TEN.
General wellbeing (high fever or hypothermia) and some organs (the lungs, kidneys and heart) are frequently affected in SJS and TEN, which may lead to death.
In order to assist non-specialist doctors with the classification of these syndromes, Bastuji-Garin et al. [5] have standardized their clinical presentations (see Table 11.2).
Table 11.2
Classification and characteristics of erythema multiforme major (EMM), Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN)
Classification/clinicalcharacteristics | EMM | SJS | SJS/TEN | TEN (with macules) | TEN (without macules) |
|---|---|---|---|---|---|
Epidermal detachment(% skin surface) | <10% | <10% | 10–30% | >30% | >10% |
Typical target lesions | Yes | – | – | – | – |
Atypical target lesions | Raised | Flat | Flat | Flat | – |
Patches | – | Yes | Yes | Yes | – |
11.6.4 Laboratory Diagnosis
There is no laboratory examination that can confirm these diseases and diagnosis is clinical and based on the patient’s anamnesis.
11.6.5 Treatment and Control of Cure
Treatment is symptomatic and principally offers general support in easing the hydroelectrolytic and caloric disturbances that can occur. There is no consensus on the use of corticosteroids and some authors say these should be limited to the first 48 h. Other studies advocate the use of human immunoglobin. Antiviral therapy and antibiotics can be used depending on the probable etiology or complications. It is imperative that the use of any suspicious or non-essential drug be suspended.
11.6.6 Differential Diagnosis
A range of clinical presentations can resemble EM, SJS and TEN, particularly bullous pemphigoid, pemphigus, Behçet’s syndrome and collagenosis. The possibility of urethritis, conjunctivitis and stomatitis with other etiologies should also be excluded. In isolated genital lesions that do not occur in TEN, differential diagnosis includes ulcerative STDs and genital thrush.
Fig. 11.47
(a–e) This patient presented these monthly symptoms during menstruation. After receiving various treatments, biopsies, investigations and diagnostic hypotheses, dipirona was finally identified (used for dysmenorrhoea) as the cause of the orogenital symptoms. The patient reported that she started to take this medicine regularly the previous year
Fig. 11.48




(a, b) This patient reported recurring symptoms of genital herpes, but the situation shown here shows the genital symptoms after use of sulfa-based local medication for the “treatment” of the ulcers caused by HSV
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
