HPV infection Biology
Lesions associated with HPV affect genital and non genital sites.
9.6 Most Common Genital Sites
Man: Glans, foreskin, frenulum, balanoprepucial sulcus, urethral meatus and scrotum.
Woman: Vulva, perineum, urethral meatus and cervix.
In both sexes there is frequent involvement of the anus, rectum and mouth.
To help visualization of subclinical lesions, acetic acid 3–5% is used, making whitish (acetowhite) the suspicious area. However, such aceto reaction is not pathognomonic of injury associated with HPV infection. Several reasons can attribute the white reaction to the acetic acid, without meaning a virus disease.
9.7 Some HPV Types and Their Manifestations
HPV 1a, b, c → Plantar warts.
HPV 2 → Vulgar warts.
HPV 3a, b → Flat juvenile warts, mild form of EV.
HPV 6, 11 → Condyloma acuminata, cervical intraepithelial neoplasia, larynx papillomas, Buschke-Löwenstein tumor, penis cancer, cervix cancer.
HPV 7 → Common warts of the hands (butchers).
HPV 13a, b → Focal epithelial hyperplasia in oral mucosa.
HPV 16, 18 → Intraepithelial neoplasia (cervix, vagina, vulva, penis, anus), cancers, Condyloma acuminata, bowenoid papulosis.
HPV 30 → Larinx squamous carcinoma.
HPV 38 → Malignant melanoma.
HPV 57 → Intraepithelial neoplasia, skin warts, nasal inverted papilloma.
9.8 Impact of HPV in Men and Women in the World1–5
Estimated global annual new cases of HPV-related disease in men and women1–5. (1) Forman D, et al. Vaccine. 2012;30(Suppl 5):F12–23. (2) Executive summary: the state of world health, 1995. World Health Organization website. http://www.who.int/whr/1995/media_centre/executive_summary1/en/index.html. Accessed March 12, 2013. (3) Greer CE, et al. J Clin Microbiol. 1995;33:2058–63. (4) Human papillomavirus and HPV vaccines: technical information for policy-makers and health professionals, 2007. World Health Organization website. http://whqlibdoc.who.int/hq/2007/WHO _IVB_07.05_eng.pdf. Accessed March 12, 2013. (5) Health Protection Agency (HPA). Health Protect Rep. 2012;6:9–15. http://www.hpa.org.uk/HPR/archives/2012/hpr2212.pdf. Accessed March 12, 2013. (a) Estimated gender ratio of genital warts: 54% men, 46% women. Meta-analysis publication available in: http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0069238sobre The Aetiological Role of Human Papillomavirus in Oesophageal Squamous Cell Carcinoma os autores resumem: “Methods: Case-control studies investigating OSCC tissue for presence of HPV DNA were identified. 21 case-control studies analyzing a total of 1223 cases and 1415 controls, met our inclusion criteria. HPV detection rates were tabulated for each study and all studies were assessed for quality. The random effects method was used to pool the odds ratios (OR). Results: From all OSCC specimens included in this meta-analysis, 35% (426/1223) were positive for HPV DNA. The pooled OR for an HPV-OSCC association was 3.04 (95% CI 2.20 to 4.20). Meta-regression analysis did not find a significant association between OR and any of the quality domains. Influence analysis was non-significant for the effect of individual studies on the pooled estimate. Studies conducted in countries with low to medium OSCC incidence showed a stronger relationship (OR 4.65, 95% CI 2.47 to 8.76) than regions of high OSCC incidence (OR 2.65, 95% CI 1.80 to 3.91). Conclusions: Uncertainty around the aetiological role of HPV in OSCC is due largely to the small number and scale of appropriately designed studies. Our meta-analysis of these studies suggests that HPV increases the risk of OSCC threefold. This study provides the strongest evidence to date of an HPV-OSCC association. The importance of these findings is that prophylactic vaccination could be of public health benefit in prevention of OSCC in countries with high OSCC incidence.
It is estimated that the incidence of recurring respiratory papillomatosis is of 4.3/100,000 children [3].
9.9 Laboratory Diagnosis (Figs. 9.188–9.205)
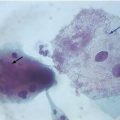
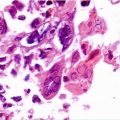
Cytology and histology can microscopically identify the most characteristic cytopathic effect: koilocytosis.
Electron microscopy and molecular biology techniques can be used to characterize the viral presence within the cells—hybrid capture or polymerase chain reaction (PCR), especially in real-time.
Colpocitology results suggestive of HPV should be regarded with caution and require combined analyses with clinical and colposcopic data. Currently the proposed Pap smear report system (Bethesda System) considers that cases suggestive of HPV cytopathy due to koilocytosis should be classified as low-grade squamous intraepithelial lesion (LSIL).
Lesions without koilocytosis but with nuclear atypical processes previously suggesting dyplasias are regarded as virtually associated with low-grade (LSIL) and high-grade (HSIL) viral action.
Biomarkers that detect and quantify the transcripts of viral oncogenes E6 and E7 are being considered for the assessment of oncogenic activity associated with viral progression of cervix infection/neoplasia. The use of protein p16ink4a, which identifies the high-grade intraepithelial lesions in cases of diagnostic doubt, is well established within the histopathological diagnostic routine. Some studies also demonstrate the usefulness of this marker associated with another one, Ki-67 (marker of tumoral proliferation) in immunocytochemistry for diagnosis of high-grade lesions. The identification of these oncoproteins activity may also be an element of prognostic evaluation in cases of squamous intraepithelial lesions of the uterine cervix.
9.10 Evaluation of Laboratory Methods
The routine use of the HPV test for molecular biology is increasingly indicated for diagnosis and prognosis of HPV infection and lesion cases. Some recent studies consider this test ideal for primary screening of squamous intraepithelial lesions of the uterine cervix. Another possibility of high-level evidence is the use with adjuvant in oncotic cytology in cases of atypical squamous cells of undetermined significance (ASC-US) for indication of colposcopy. Another indubitable indication is its HSIL post-treatment use in uterine cervix by cervical conization as a prognosis of the lesion persistence or recurrence. It is the degree of the cellular alteration and not the presence/absence of HPV what dictates the clinical conduct.
The viral persistence, which is considered a major risk factor for HSIL, is determined by two positive PCR tests for the same viral type at an interval of 1 year. It makes no sense, with the current knowledge, testing every 3 or 6 months.
Sensitivity and specificity of tests take into account the histopathological HSIL diagnosis (gold standard).
Exam | Specificity % | Sensitivity % |
|---|---|---|
Oncology cytology | 88–89 | 50–60 |
Colposcopy | 90–99 | 40–70 |
Hybrid capture | 90–95 | 95–98 |
Real-time PCR | 94–96 | 97–99 |
9.11 Treatment and Control
Warts:
Application by patient:
Imiquimod (cream 5%): topical use. It is not indicated for internal use (vaginal/anal). Application must be in each lesion, three per week, for a period of 4–16 weeks. Side effect as local irritation/burning is not uncommon. It can be used alone or associated with physical removal method through surgical exeresis or electrocoagulation. The ideal practice is to make the application shortly before bedtime and wash the area with common soap and water 8 h after application. As a routine, client is informed to wash the area where imiquimod was applied 7 h later rather than 9 h later, which minimises the collateral effects.
Podophyllotoxin 0.5%: topical use. Used in cycles as follows: twice a day, for 3 days, with an interval of 4 days without application. More than four cycles should not be used. Local irritations are frequent, and patient should be oriented to suspend the use in such case. Not indicated for pregnant women.
Sinecatechins Oitment (Veregen®) 10% w/w in 15 g tubes (Canada). In the USA, this product is commercialized with a concentration of 15%. Used only on skin, three times a day (morning, afternoon and evening). The treatment must be done until lesions disappear. But treatment should not exceed 16 weeks. The side effects are similar to those of imiquimod’s. The application of sinecatechins oitment should be suspended in case of intense side effects.
Application by physician:
Podophyllin 10–25% (we prefer in tincture of benzoin. But it can be oily or alcoholic): topical use. The teratogenic origin is not indicated for the mucous membranes. The region must be washed 4 h after application. Care must be taken with excesses—application should be repeated every week.
Trichloroacetic acid—TCA (30–90%): topical use. Weekly serial applications until involution of lesions.
Surgical removal: perhaps the simplest and most effective method. There are many ways to carry out the lesion excision: with delicate surgical scissors and later soft cauterization of the bases through laser or electric scalpel (electrocoagulation).
Cryotherapy with liquid nitrogen: weekly serial applications until the lesions’ regression.
Cryocauterization
Cryotherapy destroys warts by thermal-induced cytolysis. Healthcare professionals must be trained on the proper use of this therapy because over and undertreatment can result in complications or low efficacy. Pain after application of the liquid nitrogen, followed by necrosis and sometimes blistering, is common. Local anesthesia (topical or injected) might facilitate therapy if warts are present in many areas or if the area of warts is large.
Cryotherapy with liquid nitrogen or cryoprobe. Repeat applications every 1–2 weeks.
Fluorouracil (5-FU)
Fluorouracil (5-FU) is an antineoplastic agent, cytostatic, analogue of Uracil and therefore a pyrimidine antagonist, which inhibits the synthesis of viral DNA/RNA, and with immunostimulating action. The medication comes as a cream 5%. It is indicated for use in both skin and mucous membranes. It can produce side effects such as erythema, swelling, burning, itchiness, pain, ulceration and dysuria. Two treatment schemes are recommended: daily use for 5 days or weekly application for 10 weeks. Wash lesions 4 h after external applications. Vaginal and cervical lesions should use 3–5 mL of cream with applicator deeply at bedtime. Insert a vaginal tampon and protect the vulva with Vaseline or zinc oxide. The use in vulva produces vestibulitis, and in the vagina can cause chronic ulcerations and adenosis, reason why we do not recommend its routine use.
For some people, the combination of treatments can reduce recurrences. However, they may increase complications.
After 6 months without presenting clinical manifestation of the disease, patient must be discharged.
Podophyllotoxin and podophyllin should not be applied to pregnant women. Podophyllin and trichloroacetic acid should not be applied by patients at home.
Squamous intraepithelial lesions: can only be accompanied if they are low-grade lesions, especially among young women. Cases of low-grade intraepithelial lesions confirmed by biopsy, persistent and in women over 30 years of age may require destructive therapy or surgical excision. The high-grade lesions confirmed by biopsy should be submitted to excision by conization.
Prophylactic vaccine against HPV: immunogenic materials used are virus-like particles (VLP) HPV-specific types 6, 11, 16 and 18. These particles represent only the viral capsomers without any genetic content. This causes the immunogenetics to be maintained without the slightest possibility of causing infections. Such methodology is widely and safely used in other vaccines, such the hepatitis B. The first vaccine was approved in 2006 and has four VLPs (6, 11, 16 and 18). Thus, it protects against Condyloma acuminata (anogenital warts) and concomitantly intraepithelial neoplasias and cancer of the vulva, vagina, cervix and anus. The posology is three doses IM: 0 day, 60 days and 180 days. The second vaccine was approved for use in women and girls over 10 years of age and has proven effectiveness for the intraepithelial neoplasias and cervical cancer. This vaccine contains two VLPs (16 and 18). Must also be applied in three IM doses: 0, 30 and 180 days. In September 2009, the U.S. agency that regulates food and drugs administration (FDA) approved quadrivalent vaccine against HPV 6, 11, 16 and 18 in men from 9 to 26 years of age. In Europe, the similar committee, EMEA, also approved a very important decision: the extension of the use of the same vaccine for women over 45 years of age. Earlier, the World Health Organization awarded its seal to this product. The HPV 16 and 18 bivalent vaccine has also been approved by FDA. Nowadays, it is proved that the protecting effect of these prophilatic vaccines surpasses 9 years. In 2010, during the international event Eurogin Monte-Carlo, Joura EA et al. (Impact of Gardasil® in women who have undergone definite therapy, SS 4–3) have shown that there are benefits in using quadrivalent vaccine against HPV in women who have had cervix or vulvar diseases and were properly treated, once they have reported significantly lower rates of new diseases caused by HPV in the genital area. More recently, international study has shown good results with the quadrivalent vaccine in preventing penile and anal lesions in research involving only men. All this proves that these vaccines bring great benefits for the human species, with low side effects. Some countries have already managed to vaccinate large portion of their teens. More recently, FDA has approved the nine valent HPV vaccine against types 6, 11, 16, 18, 31, 33, 45, 52 and 58. The nine valent vaccine was 97% effective in the prevention of cervical cancer in vulva and vagina caused by additional types 31, 33, 45, 52 and 58, as well as of diseases caused by the previous four types of HPV vaccine in clinical studies.
Therapeutic vaccine against HPV: there are studies about the therapeutic vaccines, which differ from the prophylactic vaccines due to the ability to act against infection and lesion manifestations established through the immunocellular via, assisting in the viral elimination. This process is mediated by T cells and not B cells as occurs in the prophylactic vaccines.
9.12 Complications
Complications are extremely related to the intraepithelial/cancer lesions of the uterine cervix, and with a variable frequency also with the vagina, vulva, anus, penis, oropharynx, and oesophagus.
Most cancers have multifactorial etiology. HPV seems to be insufficient to produce alone the malignant transformation. Several factors may be involved, mainly with co-infection with chlamydia and herpes virus. Smokers also have increased risk for malignant progression of HPV infection.
Large condylomatous masses may require large surgeries. Thus, deformities may occur.
Giant condyloma is an entity known as Buschke-Löwenstein tumor and means manifestation by strongly aggressive HPV 6/11, regarding the genital region damage. Histopathologically it is not malignant.
Complications for people who come across of the HPV three letters in emotional, sexual, social, marital, financial, and professional areas, in most cases, are difficult to identify and solve. However, the professionals who serve people suspicious of or confirmed HPV infection/disease diagnosis should be alert and available to minimize these complications.
9.13 Diferential Diagnosis
Condyloma latum (condyloma planum/papular syphilides—secondary syphilis), molluscum contagiosum, benign tumors and malignant neoplasias of non-viral origin.
9.14 Observations
Treatment of systemic and local secondary infections promotes the remission of lesions. The same happens in the post-delivery women with HPV lesions, especially genital warts.
Numerous therapies are a sign that none of them is sufficient for an ideal control. All, without exception, have high rates of HPV recurrence (> 50%).
With the current knowledge, it is not true to say “once with HPV always with HPV”.
Moast intraepithelial lesions, especially those of low-grade, also tend to evolve. However, the clinical, laboratory and emotional monitoring should not be neglected.
The cesarean delivery should be considered when there are lesions obstructing the birth canal, disabling any type of episiotomy, and also high-grade or vegetant cervical lesions, due to high risk of lacerations and bleeding.
Re-examining the patient 3 months after the disappearance of the lesions is a good behavior.
As we believe in sexual transmission and in the association with STD, we are favourable to classical medical examination of sexual partners. This is different from “peniscopy” only.
Emotional verbal untrue or exceeded concepts assaults may be worse than clinical lesions. In this particular topic we indicate the short-movie Lara’s Show (https://www.youtube.com/watch?v=GgwlpwLyT-k).
Read the book “HPV, Que. Bicho É Esse?” (http://virushpv.wordpress.com)—Larah’s program (in English) based on the novel “HPV, Que. Bicho É Esse?”
In 2010, an international study about histological samples from several countries was published, and showed the participation of isolated HPV 6 HPV (mainly) and HPV 11 in several penis cancer cases, although the most prevalent type is HPV 16. So far HPV has been detected in about 60% of cases of penile cancer. It has also been found, as the only present type, HPV 6 in pieces of histological cervical cancer.
The physician must not exaggerate the severity of the diagnosis or prognosis, nor complicate the treatment, exceeds the number of visits, examinations or any other medical procedures.
Primary screening for HPV-DNA to prevent cervical cancer.
In the recent years there are some concern about the effectiveness of Pap smear as primary screening for cervical câncer, meanly in the development countries, where the incidence of cervical câncer is stable. An alternative defended by researchers is the use of DNA-HPV test, due to its high sensitivity to detect high-grade lesions and the possibility of auto-collect. Although rare, benign or malignant clinical manifestations are observed in very different areas from the usual ones, such as esophagus [4].

Fig. 9.1
Typical clinical manifestation of Condyloma acuminata: genital wart

Fig. 9.2
Although the lesions may be agglutinated, the multicentricity is remarkable. Notice the distance

Fig. 9.3
It is very difficult to ensure that the more keratinized, the lower the power of contamination. However, in our practice, we found several patients with clinical keratinized forms, dry, who have sexual partners, sometimes more than one examined, with no HPV lesions
Fig. 9.4
(a) Although isolated lesions occured, satellites (including in the urethral meatus and penis shaft), this case presents itself as a true mountain range, a collar that surrounds virtually the entire glans. (b) Whenever possible, we prefer to treat genital warts by exeresis. However, in situations like this, a possible scar sequel can be disastrous. So, trying to decrease the number and size of lesions with trichloroacetic acid 60–90%, with imoquimod can be a good tactic

Fig. 9.5
The pathogenesis of HPV causes hyperplasia in the infected tissue, manifested as an excrescence as observed, once again, with this case, similar to the previous one, but smaller

Fig. 9.6
Patient with Condyloma acuminata in penile foreskin. Popularly, this disease is known in many regions as “cockscomb”

Fig. 9.7
(a–c) Condyloma acuminata in the urethral meatus. It is worth noting that the lesion is better visualized when the urethral meatus walls are separated
Fig. 9.8
(a) At first it seems that the condylomatous lesions are only around the urethral meatus. (b) Observing more carefully, it may be noted that the bases of the Condyloma extend to the urethral mucosa

Fig. 9.9
Pregnant 15-year-old patient showing Condyloma acuminata lesions in vaginal introitus. Classical attention: do not use podophyllin, because this drug is highly toxic, causing serious problems on fetus, annexes and pregnant woman also. However, we often observe women doing podophyllin solution self-application, at home, prescribed by health professionals
Fig. 9.10
(a) This case of Condyloma acuminata was part of a randomized, double-blind, multicenter study involving four groups: (1) surgical exeresis with electrocoagulation of the bases; (2) Interferon α2b 2,500,000 UI in subcutaneous skin of the abdomen, on alternate days, in a total of eight applications; (3) Combination of procedures 1 and 2; (4) Placebo (interferon α2b diluent liquid). (b) At the end of the treatment. (c) Two weeks after treatment with interferon only. The result of this research, which involved 100 patients (25 in each group), was as follows: surgical exeresis: cure of 56%; Interferon: cure of 48%; exeresis + interferon: 72%; and placebo: 4%. The cure criterion used in the study was the absence of Condyloma lesions after colposcopy for a minimum period of 6 months after treatment. Details of the article are available on: http: http://www.dst.uff.br//revista16-2-2004/4.pdf

Fig. 9.11
After many failed attempts of caustic treatment in public health unit, this patient was referred to our service, also public, for final treatment. We have examined and re-examined, and decided to refer patient for evaluation of an urologist, then conducted patient to another service, due to a shortage of surgical conditions in our service (operating room and anesthesia). However, all STD cases routine procedures were conducted. At examination, the rapid tests for HIV and syphilis were non-reactive. Subsequently, feedback reported that the lesions were removed in a surgical environment

Fig. 9.12
(a) Another successful case of interferon α-2b protocol. (b) When it works, and in our experience only 48% does, the great advantage of interferon is the absence of residual scars. Disadvantages: high price, side effects (fever, headache, general malaise as the flu) and low cure rate. In very special cases, it may be a reasonable option therapeutic association
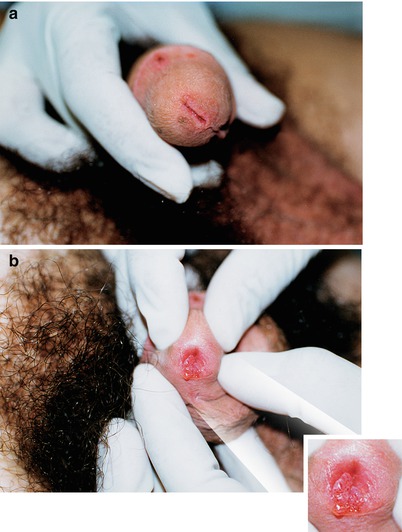
Fig. 9.13
(a) Young man, only partner of woman with vulvovaginal Condyloma acuminata, who was undergoing treatment with another professional, was referred to our service. While gathering medical history, we learned he was monogamous. His last sexual contact with another woman occurred more than 8 years ago. We were informed that he had already made two peniscopies in the last 2 months, with normal results. In photo (a), it is not possible to notice any suspicion of HPV. (b) However, when urethral meatus was opened, multiple Condyloma virus were seen. Thus, it is evident that the clinical examination must include the exhibition of both the urethral meatus and the navicular fossa

Fig. 9.14
(a) Patient presenting Condyloma acuminata, recurrent genital ulcer (genital herpes). (b) This photo shows the careful application of trichloroacetic acid in condilomatous lesion, and herpetic lesions with erythematous halos. It is worth mentioning that this patient spontaneously sought our service for treatment of genital ulcers. Patient reported that the wart on the penis stem did not bother him, unlike the penile wounds. In the service routine the serology for syphilis, hepatitis B, hepatitis C, HIV, anti-HBS were non-reactive. Hepatitis B vaccination schedule was prescribed

Fig. 9.15
Patient referred to peniscopy, because his partner had HPV in uterine cervix. No HPV lesion was found in the penis or scrotum, however, condylomatous injuries were found in the anal margin. The patient denied homosexual relationship. He reported mutual oral sex with his partner, including in the affected area. In the service routine the serology for syphilis, hepatitis B, hepatitis C, HIV, anti-HBs were non-reactive. Vaccination schedule against hepatitis B was prescribed, as well as for the partner

Fig. 9.16
Child with extensive condylomatous lesion. The therapeutic option was the exeresis of injuries in surgical environment and under narcosis. We consider that the treatment in ambulatory enviroment is very painful and stressful for everyone: child, family and medical staff. Notice that in (a) the removal by dissection with cold scalpel was the option. The base was wide and suture with categute was carried out. It was not possible to establish connection with sexual abuse, but we notified Child Protective Services. In the service routine the serology for syphilis, hepatitis B, hepatitis C, HIV were non-reactive. The vaccination card showed that the vaccines were updated, including the hepatitis B vaccine

Fig. 9.17
Female patient presenting Condyloma only in the anal area. She, however, had eventually anal sex, and lesions existed in inner mucosa after the anal sphincter. It is important to point out that, when examining a patient with suspected or presenting Condyloma, the physical examination must include the genitals, mouth and anus
Fig. 9.18
(a) Teenager showing multiple lesions of Condyloma acuminata, complaining of burning and urethral secretion. (b) Vegetant lesion by HPV in urethral glans, not reaching the mucous membrane of the urethra itself. Notice that the urethral secretion is not evident, because patient urinated a few moments before the examination. (c) He was oriented to wait in the waiting room, without urinating so we could collect urethral material for tests. Direct bacterioscopy showed intracellular Gram-negative diplococci in polymorphonuclear. Culture in Thayer-Martin medium and other biochemical tests identified Neisseria gonorrhoeae. (d, e) After surgical exeresis of the lesions, electrocauterization of the bases for complete hemostasis was carried out with delicate curve scissors. Procedure made in ambulatory under local anesthesia


Fig. 9.19
Teenage examined at the STD Department of UFF (Fluminense Federal University), Niterói-RJ, with extensive condylomatous lesions in penis. Notice condylomatous mass in penis shaft near the root, with a diameter of approximately 6 cm. Presents also smaller lesions of Condyloma acuminata spread throughout the genitals (a–d). It is possible to observe dermatomycosis in the pubic area too (a). The excessive time taken to solve the problem must be mentioned. The patient and his mother reported that have been looking for help for more than 7 months on the basic health system, but were not successful (according to patient information). Reported that the the lesion was small at first and that soon after that looked for medical help. Several solutions were applied, but it took many days, even weeks until next sessions. Thus, the condylomatous mass kept growing. The unfortunate data are: the serologies for syphilis and HIV were requested only after 7 months of follow-up on the case. Although the mother had informed that teenager had received vaccinations against hepatitis, we have required serological tests, and anti-HBs marker was non-reactive. Hepatitis B vaccination schedule was prescribed. The serology for syphilis and HIV were non-reactive. Forty-eight hours after our first examination at Hospital Orêncio de Freitas, from the municipal health system, in Niterói, with surgical team led by urologist and anesthesiologst, exeresis of lesions was carried out in surgical center environment with narcosis complemented with local anesthesia (e–l)

Fig. 9.20
Similar case to the one shown in Fig. 9.13. However, this one shows that Condyloma acuminata lesions, besides the urethral mucosa, are also external
Fig. 9.21
(a, b) Middle-aged patient with verrucous lesions on the penis for more than 8 years. Lesions are extremely keratinized, characteristic of verruca vulgaris. Trying to treat such injuries with podophyllin solution or trichloroacetic acid solution is not successful most of the time. The cryocauterization (CO2, liquid nitrogen) can really help. Surgical removal can quickly remove the warts, but the scarring sequels cannot be forgotten

Fig. 9.22
As in the previous case, warts are very keratinized. In our practice, these lesions are not easily transmitted. They are very dry. On this case in particular we can assert that we have examined five sexual partners of this young woman and none of them showed suspicious or typical HPV lesions

Fig. 9.23
HPV lesions that although verricous, are more flattened: high relief rugose. As some lesions are at the root of penis, some of them might be outside the coverage of the male condom

Fig. 9.24
In many cases the Condyloma lesions are resistant to various therapeutic methods, and become recurrent. This can lead to such distress that the patient himself uses formulas indicated by friends. In this case the patient “pulled” the lesions with nail plier. Notice associated dermatomycosis at hypogastric region skin also

Fig. 9.25
Condyloma acuminata in the urethral meatus. In many cases, it takes some time until patient be aware of the lesion. Frequently, the problem is noticed during medical examination and peniscopy, because sexual partner presents genital changes by HPV

Fig. 9.26
Patient with aids using HAART irregularly, examined at the STD Department of UFF with extensive HPV condylomatous lesion resistant to numerous treatments

Fig. 9.27
(a) Twenty-four-year-old patient referred to treatment of reddish plaques lesions in penis treated with antifungals. (b) Also presented high relief rugose lesions. Biopsy was carried out in two distinct points (reddish and high relief rugous lesions). In both biopsies the result was positive for cellular cytopathic effect compatible with HPV infection conclusive of flattened Condyloma. Patient was medicated with imiquimod three times a week. (c) The lesions disappeared in a few weeks

Fig. 9.28
Extensive perianal condylomatous lesion in a 15-year-old pregnant patient. In cases like this, we must remember that the topical use of podophyllin is formally contraindicated. Numerous lesions cover the anus when we try to expose the anal orifice. We believe that a proctologist must carry out the surgical procedure for these lesions removal. After all, there are often also intra-anal lesions

Fig. 9.29
There was such an anguish in this case, that patient spilled battery water over the penis to “burn” the lesions. This is a very corrosive product. It should be mentioned that most car batteries are currently completely sealed up

Fig. 9.30
The lesions often become macerated due to the humidity of the area. That’s what happened with these lesions of Condyloma acuminata in the foreskin. One should always seek differential diagnosis or co-infection with syphilitic flat Condyloma. In this case, all serologies were non-reactive and the final diagnosis was Condyloma acuminata

Fig. 9.31
In patients with so voluminous condylomatous lesions, the first step is to treat the secondary infections to improve local immunology. Often, treating associated gonorrhea, chlamydia, trichomoniasis, and vaginitis, the number and volume of the lesions can be decreased. The same procedure must be adopted for syphilis and HIV. On the other hand, assaulting these lesions directly, concomitantly with other infections is not the best conduct, because the dead tissue facilitates the dissemination of the infection. Obviously a good professional wants to treat people with this process immediately. However, we must control our anxiety. Acting impulsively can cause a disastrous result for the client

Fig. 9.32
In the therapeutic process, close attention must be given to the sequelae of the lesion adjacent areas, mainly the clitoris and the urethra
Fig. 9.33
(a) Condylomatous lesions and pregnancy. This patient showed signs of good involution after childbirth. (b) After pregnancy, as “magic”, the lesions often begin to recede spontaneously. Treating Condyloma acuminata in pregnancy is usually a big challenge. However, full attention must be given to diagnosis of associated infections as cervicitis, vaginitis, syphilis, HIV
Fig. 9.34
(a) This is one of the patients who have benefited from the use of interferon α2b for Condyloma acuminata. (b) Complete remission after treatment. Although it works in some cases (48%), we believe that the cost-benefit relation is not always useful. Nowadays, the drugs applied by the patient, at home, such as imiquimod, podophyllotoxin, sinecatechins, can bring good results

Fig. 9.35
Vegetant lesions of HPV infection Note, however, that the lesions are hyperchromic and with plane surface

Fig. 9.36
Although similar, this is another case of vegetant, verrucous and keratinized HPV lesions. Notice the good separation between the lesions
Fig. 9.37
(a, b) Patient had these warts for more than 7 years. Thus, as in the two previous cases, various topical solutions applications were used, all without any success. According to the patient, he has been at approximately 10 different hospital ambulatories/clinics (public), more than 50 times, looking for treatment. Here at the STD Department of UFF, we did not spend more than 20 min to surgically remove all visible lesions. The patient was observed for more than 1 year and showed no recurrence. The fixed sex partner was examined and did not present clinical and colpocytologic manifestations of HPV infection. The anti-HIV, anti-HCV, anti-HBs and HBsAg serologies were non-reactive. Patient received prescription for vaccination schedule against hepatitis B

Fig. 9.38
(a) Patient was referred to us for a peniscopy procedure, because its only partner showed Condyloma in the genital (according to patient information). Colposcopy was negative. However, when we mentioned that the mouth should also be examined, patient reported that he let a mustache grow, as he was ashamed of a wart on the “corner of the mouth”. (b) During the examination, the patient reported that as an average (no math), every 10 times he had intercourse with his partner in 10 used the penis and in 1 had oral sex (he in her)
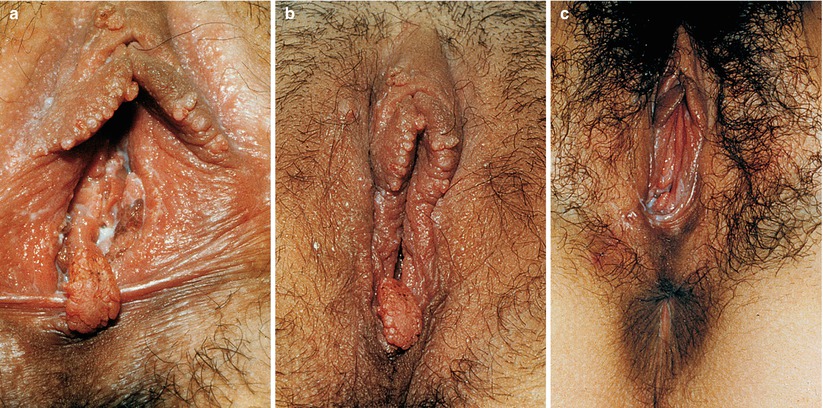
Fig. 9.39
(a) Vulva with Condyloma acuminata and vulvovaginitis by candida. This is the patient’s partner of previous case. (b) Process receding. (c) Case totally cured of HPV condylomatous vegetant lesions. Podophyllin 25% solution was used in tincture of benzoin. The anti-HIV, anti-HCV, anti-HBs and HBsAg serologies were non-reactive. Vaccine scheme against hepatitis B was prescribed

Fig. 9.40
Condyloma acuminata in mouth. Exophytic and rounded lesions, of irregular surface, arranged linearly on jugal mucous, and another identical lesion in the lateral border of the tongue in a patient practitioner of fellatio, whose partner had identical lesions on the penis

Fig. 9.41
Condyloma acuminata in mouth. Multiple verrucous aspect lesions located in the jugal mucosa of a patient with aids
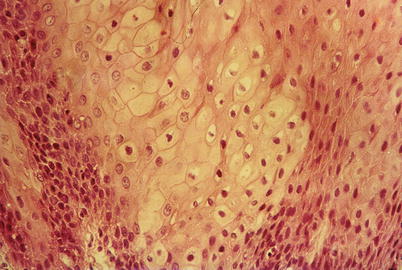
Fig. 9.42
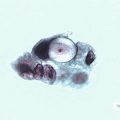
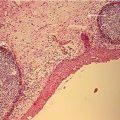
Condyloma acuminata. Histological aspect of lesion removed from tongue, observed in optical microscopy, showing epithelial cells with intense intracellular edema, present in germinal extract, showing koilocytes often present in epithelial growth induced by HPV

Fig. 9.43
HIV-positive patient with HPV infection in labial commisure. Patient denied having warts in any area of the body throughout life. The genitoscopy was negative for HPV and showed only mild fungal balanitis

Fig. 9.44
Condyloma acuminata in tongue. No genital injury. However, had medical history of sexual partners diagnosed with genital warts. Patient reports oral sex often

Fig. 9.45
HIV patient infected with extensive condylomatous lesions (HPV) in the oral cavity

Fig. 9.46
Patient examined at the STD Department of UFF with leukoplastic lesion (arrow) in hard palate evolving for more than a year. Has been forwarded to a colleague of the oral pathology ambulatory, Faculty of Dentistry at UFF, where the lesion resection was carried out and histopathological diagnosis of Condyloma acuminate was found. The research for PCR revealed HPV 11

Fig. 9.47
Six-year-old boy, with great oral unique vegetant lesion, suggestive of HPV infection. His sister and brother-in-law were patients of the STD Department of UFF and a suspicion of sexual abuse was raised. A complete physical examination was carried out to look for other signs of violence, as well as investigation through interview with psychologist and social worker, without any evidence of abuse. The discovery of the source of contact occurred when the child took an applicator of gynecological cream lying on the office’s table and began to rub it on the affected gingiva. At that very moment his mother said “he always does that with his sister’s tubes”
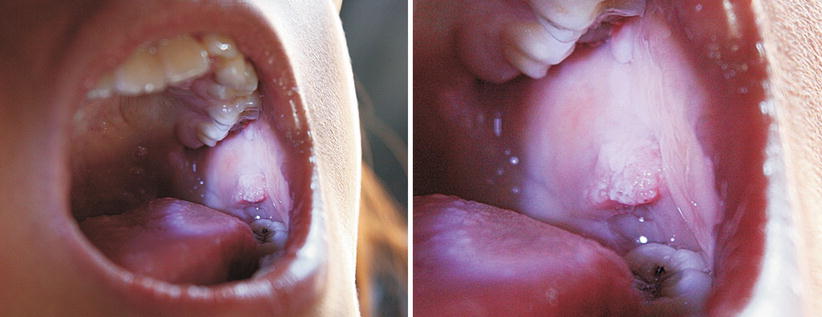
Fig. 9.48
Eight-year-old indigenous with multiple HPV lesions in the oral cavity. Some small, on lips, and other larger (see photo) on the buccal mucosa. This is a case of focal epithelial hyperplasia, also known as Heck’s disease. This is a benign disease and more commonly found in indigenous populations, among the natives of the State of Roraima, Brazil. It is correlated with human Papillomavirus types 13 and 32
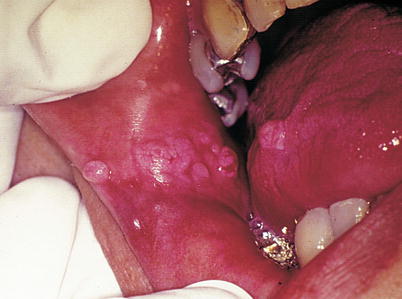
Fig. 9.49




Condyloma acuminata. Exophytic and rounded lesions, of irregular surface, linearly arranged on jugal mucous and another identical lesion in the lateral border of the tongue in a patient who had oral sex with frequency, whose partner had identical lesions on the penis
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
