Fig. 16.1
Bony facial morphology at the level of the cheekbone in axial section. Compare the (a) dolichocephalic Caucasian face and the (b) brachycephalic Asian face
The goals of reduction malarplasty are as follows:
- 1.
Reduction of facial width
The main objective of reduction malarplasty is to make facial contour more slender and narrow. Usually, facial width is determined by bizygomatic distance which connects the articular tubercles on bilateral sides. Hence, reduction or transposition of the zygomatic arch is an effective method to narrow facial width. As zygomatic body is hypertrophied concurrently in most of these cases, reducing only zygomatic arch may not be able to correct boxy appearance; thus, combined and harmonious reduction of zygomatic arch and body is essential. [1]
- 2.
Change a boxy facial contour into a three-dimensional contour
Changing in the shape and position of the zygomatic body can create a midface fullness that appears more three-dimensional and youthful.
- 3.
Attain a smooth facial line
Individual having smooth facial line looks more feminine and young. In cases of protruded cheekbones in outward direction, the facial line connecting the temple-zygoma-cheek-mandibular angle constitutes a very rough and uneven line (Fig. 16.2). Zygomatic reduction is a good option for the patients who desire a youthful, soft, and feminine facial contour.
Fig. 16.2
Anterior and posterior facial contour lines. The anterior facial contour line connects the temple, zygomatic body, cheek, and mandible body (red line), while the posterior facial contour line connects the temple, zygomatic arch, mandible angle, and chin (blue line). If the anterior contour line is too convoluted, the patient gives a “strong,” “offensive,” “old,” “tired,” “masculine” impression. The posterior contour line reflects the facial width and facial size
Patient Assessment and Consultation
Direct physical examination is the most important process to evaluate the patient’s problems and establish a surgical plan. Clinical photos are necessary, as is radiologic examination including frontal view, submentovertex view, and Waters’ view. A computed tomography (CT) scan with 3D reconstruction is also helpful to evaluate the shape of the zygomatic complex. The key variables to consider are the volume and position of the zygomatic body and the bizygomatic width. The amount of ostectomy required during the surgery is determined according to the volume of the zygomatic body. A wider resection of the zygomatic body should be planned when the volume is large. However, excessive reduction may cause a flat or deficient look. Therefore, maintaining an adequate volume of the zygomatic body in the anteroposterior dimension and transverse plane after the surgery is essential.
To make the midfacial width narrow, the lateral margin of zygoma should be trimmed or moved medially. If the outer margin of zygoma is placed laterally, the amount of osteotomy and medialization should be maximized. The maximal malar projection (MMP) point is the most protruded portion of the outer contour of zygomatic complex in the basal three-quarters view. If osteotome line is placed lateral to the MMP point, or the reduction of the zygomatic body is performed only by shaving, this point stays unchanged although the outer margin of the zygomatic body is narrowed. It results in an unnatural, two-dimensional appearance. Therefore, making adequate projection and positioning MMP point at ideal position is the key for desirable postoperative result.
The ideal MMP point may vary among different ethnicities and subjective favors; however, the following are two simple methods of determining the ideal position of the MMP (Fig. 16.3) generally.
Fig. 16.3
Determining the ideal position of the maximal malar projection (MMP). (a) Hinderer analysis. (b) Wilkinson analysis
Hinderer Analysis
The MMP is determined at the point of intersection of two lines. One imaginary line connects the lateral canthus and the oral commissure, and another line connects the nasal alar base and the tragus. The new location of MMP is a point placed in juxtaposition to the crossed lines in the outer upper quadrant [2].
Wilkinson Analysis
An imaginary line is dropped vertically downward from the lateral canthus to the degree of the mandible. The MMP is located at one-third the distance from the lateral canthus to the angle of the mandible [3].
Once the surgical plans for the zygomatic body are determined, the bizygomatic width is measured. As arch medialization is critical in the reduction of posterior facial width, the degree of arch impaction should be decided. The posterior basal portion of the arch that is posterior to the osteotomy cannot be medialized and should be carefully shaved for less visible step. Too much arch medialization without adequate reduction of zygomatic body will result in a flat and boxy face. To prevent this outcome and create a harmonious midface contour, the degree of reduction of the zygomatic body and arch should be coordinated and balanced.
There are many variables that surgeons should consider during surgery, and these should be decided by evaluations described above. Variables in reduction of zygomatic body are amount of (1) ostectomy, (2) medialization, (3) setback, and (4) vertical repositioning. Variables of zygomatic arch reduction are the amount of arch medialization and degree of shaving of the articular tubercle posterior to the osteotomy line.
As facial soft tissue is also an important component in reduction malarplasty, it should be considered for the pleasant aesthetic result. If the patient has thin skin with minimal cheek soft tissue, changes after reduction malarplasty will be obvious with minimal possibility of soft tissue drooping. This patient is an ideal candidate for reduction malarplasty. However, problems of visible bony step around the osteotomy and palpable plate through the skin are more probable. Surgeons should put more effort to make a smoother transition between bony osteotomy. On the contrary to these cases, if the patient has abundant soft tissue or thick skin, the risk of cheek drooping has risen. Surgeons should explain about the possibility of cheek drooping and consider appropriate additional procedure such as liposuction or lifting. If patient’s malar fat pad is thick, the zygomatic body should be overcorrected than generic cases to meet enough reduction.
Surgical Techniques
The surgical approach and technique for reduction malarplasty was introduced in 1983. Onizuka et al. [4] introduced chiseling and/or shaving method to reduce the protruding portion of the malar bone through intraoral incision. After that, various surgical techniques have been devised, such as bone shaving, infracture of the zygomatic arch [5], and osteotomy/ostectomy of the zygomatic body [2, 6–9]. Bone shaving method is the simplest and easily practicable method when it is used for localized protrusion of a zygomatic body. However, excessive shaving of the zygomatic body may cause exposure of cancellous bone, and it can result in postoperative irregularity [10] as cancellous bone is absorbed unpredictably. Thus, the amount of shaving is limited, and the overall size of the zygomatic body cannot be reduced only with shaving method. Furthermore, shaving method cannot be applied to the zygomatic arch as thickness of arch is not enough to be reduced through shaving [11]. The in-fracture technique [5] is one of the useful methods in reducing the protrusion of the zygomatic arch. Surgeons usually conduct osteotomy of the zygomatic arch, avoiding a full-depth cut and maintaining the continuity of the periosteum (greenstick) [10] and pushing the zygomatic segments medially. Its major advantages are simplicity and speed; however, it carries the risk of an uncontrolled amount of in-fracturing in the zygomatic arch, and it has a limited effect on a prominent zygomatic body. An L-shaped osteotomy of the zygomatic body is the preferred method for patients with moderate to severe malar protrusion due to wide zygomatic arch and prominent body. An L-shaped osteotomy is made in the anterior part of the zygomatic body, and a separate osteotomy is made in the posterior part of the zygomatic arch. With or without removal of bone [6], a zygomatic segment is moved to the desired position and fixed with wires or plates and screws. The L-shaped osteotomy technique can change both the zygomatic body and arch and has the advantage of controlling the degree of reduction as well as the shape after reduction. As patients usually desire change in the zygomatic body and arch, L-shaped osteotomy is currently the most frequently used and preferred method in zygomatic reduction (Fig. 16.4).
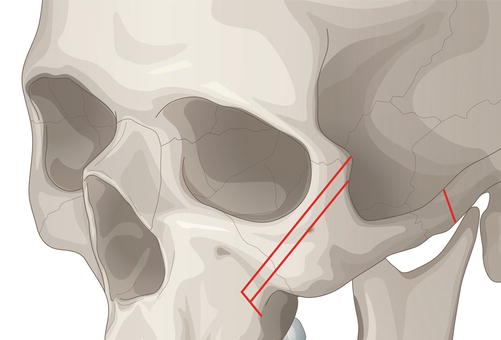
Fig. 16.4
Design of bone cuts in malar reduction. An inverted L-shaped osteotomy line is marked over the malar eminence. A second, parallel line is drawn lateral to the first line to represent the strip of bone to be resected. A posterior bone cut is made ~2 to 3 cm anterior to the tragus
The approach for reduction malarplasty can be simply divided into two types: the external approach (coronal incision, temporal incision, preauricular incision) and the intraoral approach. The external and the intraoral approaches have their respective advantages and drawbacks [11]. As zygomatic reduction developed from the treatment of zygomatic fracture, the coronal approach was first used to expose the entire zygomatic body and arch. However, it requires a long operation time, and it may cause bleeding and visible scarring. The intraoral approach has the advantage of hidden scars, limited bleeding, and short operation time. However, it provides limited operative exposure, resulting in difficult osteotomy, limited space for fixation, and the risk of infraorbital nerve injury. Side effects include cheek drooping due to wide dissection and volume reduction, which can be avoided by minimizing the dissection. The osteotomized segment should be rigidly fixed and postoperative elastic dressing provided to prevent cheek drooping. The intraoral approach can be used solely; however, it is usually combined with preauricular incision or temple incision to minimize the dissection and the possibility of cheek drooping.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


