Stahl Ear
Akira Yamada
Arun K. Gosain
DEFINITION
Stahl ear was first described by Binder in 1889.1
Stahl ear is a congenital auricular malformation in which an abnormal third crus traverses the scapha, resulting in posterosuperior deformation of the helix.
ANATOMY
Type 1: Obtuse bifurcation of antihelix: Superior crus of antihelix is missing, and third crus is present. Therefore, the superior and inferior crura make an obtuse angle (FIG 1A).
Type 2: Trifurcation of antihelix (extra crus); this is classic Stahl ear. The third crus extends across the scapha from the antihelix (FIG 1B).
Type 3: Broad superior crus, broad third crus (protruded scapha fossa) (FIG 1C).
PATHOGENESIS
Etiology is unknown.
Abnormal course of an intrinsic transverse muscle may be associated with Stahl ear.
PATIENT HISTORY AND PHYSICAL FINDINGS
The third crus extends from the antihelix; the superior crus may or may not be present. The lower half of the auricle is usually normal.
NONOPERATIVE MANAGEMENT
If the patient presents before 1 month of age, nonsurgical correction of the deformity with ear molding techniques may obviate the need for surgery.
Ear molding techniques are most effective during the 1st month of life and are unlikely to work after the 2nd month of life.
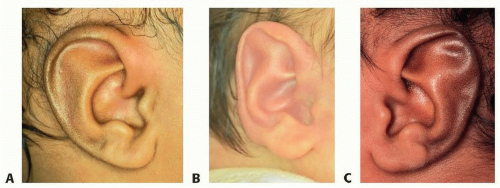 FIG 1 • A. Type 1 Stahl ear: Superior crus is missing. B. Type 2 Stahl ear: There are three crus (superior crus, inferior crus, and third crus). C. Type 3 Stahl ear: Wide third crus and protruded scapha fossa. |
SURGICAL MANAGEMENT
There are three major types of normal helix-lobule curve (FIG 2). If the patient’s helix-lobule curve falls into these three normal types, surgical correction of auricular shape may be directed toward deformities other than Stahl ear, such as prominent ear.
Preoperative Planning
The possibility of ear molding is excluded if the patient presents after age 6 weeks. Ear shape analysis (especially helix type) is performed on the patient by applying an ear template for both auricles. Photographs are taken subsequent analysis. Based on photographic analysis, the patient shown has type A helix on both the normal (FIG 3A) and Stahl ear sides (FIG 3B,C).
Two inflection points (abrupt change of the helix curve) are identified (FIG 3D), and the curve between the two inflection points is almost linear (FIG 3E).
These two inflection points are the important landmark for wedge skin incision during surgery.
Positioning
Supine position with slight head turn.
Both auricles should be prepped in the sterile field, and the contralateral ear used as a reference in unilateral correction.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








