Split Calvarial Bone Graft Harvest
Peter J. Taub
DEFINITION
Calvarial bone grafts are used for replacement of deficient bone.
These grafts are ideal for calvarial, orbital, nasal, and midfacial reconstruction.
Paul Tessier previously described, and extensively used, autologous bone grafts from the calvarium for facial and cranial reconstruction.1
ANATOMY
Because many primary craniofacial procedures are performed via a coronal incision, there is no additional access for the donor site.
Calvarial bone has a diploic structure including an inner and outer “table” of rigid cortical bone surrounding a center of softer cancellous bone.
A rich vascular system allows for rapid revascularization, and its intramembranous lineage is thought to undergo less resorption compared to endochondral bone grafts.
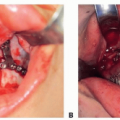
The natural curvature of the calvarium can be useful in reconstructing similarly curved structures, and additional bending is possible by incorporating kerfs on the concave surface (FIG 1).
PATHOGENESIS
Bone graft healing is affected by numerous variables.
Adequate blood supply is arguably the most important. Devascularized bone is unable to activate the process of remodeling and over a period of 6 to 12 months becomes necrotic and predisposed to infection and repeat fracture.
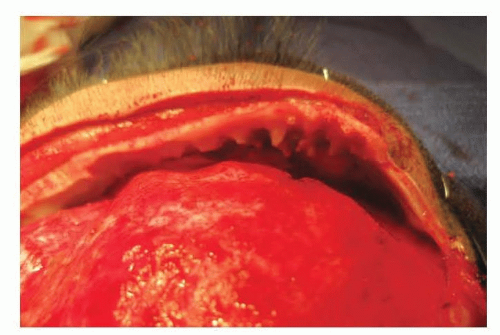
FIG 1 • Kerfs created on the concave surface of a calvarial bone graft to facilitate curvature of the bone.
Revascularization occurs through a process known as haversian remodeling. The process begins with osteoclasts traversing the fracture line. Vascular endothelial growth factor (VEGF) regulates the process of angiogenesis by increasing vascular sprouting, endothelial cell migration, and proliferation adhesion. Capillaries and osteoblasts follow to form vascularized lamellar bone.2
External radiation impairs secondary reconstruction by inhibiting bone healing and growth, limiting microvascular supply, and decreasing the integrity of surrounding soft tissue.3
Stability (elimination of motion) of the bone graft is critical to primary bone healing, whereas micromotion has been shown to facilitate bone healing through osteogenesis.4 Insufficient fixation leads to the deposition of fibrous tissue within the gap between bony segments, resulting in nonunion.
Patient age plays an important role in bone graft healing.
Younger patients demonstrate faster rates of healing than do adults, likely secondary to the increased angiogenic potential of younger bone.
Advancing age decreases angiogenesis, stem cell function, signaling cascades, and periosteal structure, all of which are essential to bone graft healing.
NATURAL HISTORY
Bone grafts heal via three mechanisms: osteointegration, osteoinduction, and osteoconduction.
Osteointegration refers to the connection between the surface of the native, living bone and that of the bone graft.
Osteoinduction refers to the process of stimulation of undifferentiated pluripotent cells into bone-producing cells through the release of growth factors.
For bone grafts, the architecture of the graft (cancellous vs cortical) dictates the success of incorporation. Cancellous bone graft incorporation tends to be more favorable compared to cortical bone, owing to its open architecture, which allows for more rapid revascularization and differentiation of osteoprogenitor cells into bone forming osteoblasts.5
Osteoconduction refers to bone formation from either adjacent bone or periosteum via the ingrowth of capillaries and osteoprogenitor cells from the recipient bed to, around, and through the graft. The graft acts as a scaffold for new bone formation.
PATIENT HISTORY AND PHYSICAL FINDINGS
Among bone replacement materials, autogenous bone grafts remain the standard. They are the only material that is truly osteogenic; cells from the bone graft contribute to new bone formation.
Bone grafts can be used for replacing acquired bone defects, such as following tumor extirpation or continuity defects following trauma; augmenting deficient skeletal surfaces, such as placement of bone graft for zygomatic or chin augmentation; or reconstructing congenital anomalies, such as alveolar cleft defects or hypoplastic mandibular rami.
IMAGING AND OTHER DIAGNOSTIC STUDIES
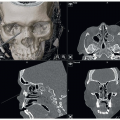
Preoperative evaluation should include a CT scan to assess the thickness of the parietal bones for harvesting grafts and of any potential midline abnormalities.
Younger patients may lack a true diploic architecture (FIG 2), whereas older patients may have areas of thin calvarial bone.
SURGICAL MANAGEMENT
Preoperative Planning
Care must be taken when choosing the site of bone harvest. In general, the flat parietal region is ideal for most applications.
The midline sagittal suture overlies the sagittal venous sinus and must be avoided. Similarly, the anterior coronal and posterior lambdoid sutures are sites of dural adherence and should be avoided.
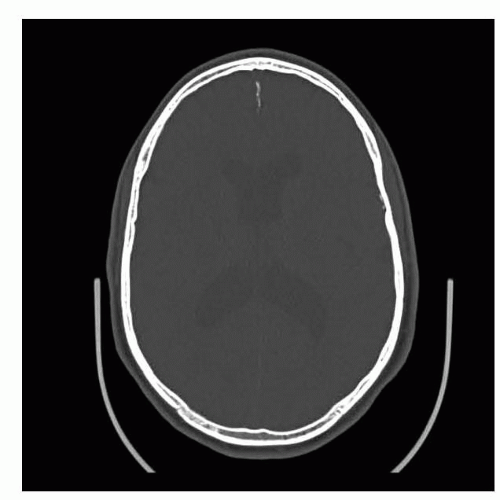 FIG 2 • CT scan demonstrating diploic architecture of calvarial bone. |
 FIG 3 • Preparation of the scalp for a coronal incision by shaving a strip of hair and excluding the remaining hair from the operative field. |
Positioning
The patient is best positioned supine with the head stabilized. This may be as simple as a foam “donut,” a horseshoe extension of the operating table, or a Mayfield clamp.
The torso should be restrained with a belt in case the table is rotated during the procedure.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree