Abstract
Drug abuse is a global problem and is directly responsible for minor to serious and fatal illnesses and injuries, as well as adverse sociologic consequences. It is estimated that in 2012, 162–324 million people, corresponding to 3.5–7% of the world’s population aged 15–64, had used an illicit drug at least once in the previous year. Skin injury may occur from accidental extravasation after intended injection into veins or intradermal or subcutaneous injections when patent vessels cannot be found (“skin popping”). Adulterants also contribute to skin toxicity, e.g. levamisole leading to ischemic vasculopathy. Cutaneous infections are common and range from abscess formation to necrotizing fasciitis. Self-induced skin injury, formication, and pruritus are additional complications of illicit drug use. Intravenous drug users can also develop infective endocarditis as well as HIV and hepatitis C viral infections.
Keywords
cocaine, morphine, opioids, methamphetamine, levamisole, formication, skin popping, skin tracks, vasculopathy, drug abuse
Introduction
According to the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), the essential feature of a substance use disorder is a cluster of cognitive, behavioral, and physiologic symptoms whereby an individual continues to use a substance despite significant substance-related problems. Diagnosis of substance use disorder is based on a pathologic pattern of behaviors including impaired control, social impairment, risky use, and the pharmacologic criteria of tolerance and withdrawal ( Table 89.1 ). This includes alcohol as well as prescription and illicit drugs.
| FEATURES OF DRUG DEPENDENCE |
|
Drug abuse is a global problem and is directly responsible for minor to life-threatening and fatal illnesses and injuries, as well as adverse sociologic consequences with loss of occupational productivity and higher rates of poverty, crime, prison occupancy, domestic violence, and child abuse or neglect. According to the National Drug Intelligence Center, in 2011, the estimated overall annual economic cost of drug abuse to American society was $193 billion. This included the costs of health care, lost work productivity, and crime.
Illicit drug use may be suspected or diagnosed on the basis of cutaneous findings. In fact, the skin is the tissue most evidently affected by intravenous drug addiction . The wide spectrum of complications results from local or systemic effects (including toxic or allergic) of the drug itself, adulterants, or infectious agents. Polydrug use and the consumption of alcohol along with illicit drugs are common behaviors in drug addicts .
Amphetamines
Amphetamines were initially sold as a non-prescription appetite suppressant and rapidly became a favorite street drug (“pep pills”, “Bennies”). Crystallized methamphetamine (“crystal meth”, “crystal”, “ice”, “glass”, “tina”), an addictive stimulant with a high potential for abuse and dependence, produces an even stronger “rush” or “flash” when the powder is injected intravenously or inhaled; it is often supplied as small “rocks”. Oral ingestion of tablets (Desoxyn ® ; “speed”, “meth”, “crank”; “yaba” [with caffeine]) or snorting powder merely produces a profound sense of euphoria. Smoking the base form (“snot”) extends the duration of the “high” for up to 24 hours. Amphetamines can lead to reduced appetite, restlessness, insomnia, and increased or distorted sensations; on physical examination, there may tachypnea, tachycardia and hypertension as well as flushing, sweating, and even uncontrollable movements or shaking. “Speed freaks” (high-intensity abusers) progressively use the drug to remain euphoric, and high doses or chronic use often lead to xerostomia, xerosis, pruritus, acne excoriée and formication, along with dental caries and loss of teeth (“meth mouth”). “Tweaking”, continuous drug use without sleep for 3 to 15 days, is frequently associated with irritability, paranoia, violence, and frustration due to an inability to recreate the euphoric high.
Methylenedioxymethamphetamine (MDMA), also known as “ecstasy”, “E”, “Adam”, “X”, “XTC”, “molly”, “hug”, or “beans”, is a synthetic stimulant and hallucinogen with a chemical structure similar to methamphetamine. MDMA causes a reduction in the concentration of serotonin transporters (SERTs) within the brain , and brain injury caused by heavy, prolonged use of MDMA may be long-lasting . High doses can cause malignant hyperthermia, leading to rhabdomyolysis, renal failure, and cardiovascular collapse. Due in part to an increase in energy and a reduction of sexual inhibition, crystallized methamphetamine and MDMA are a staple at raves and PNP (“party and play”) parties and have been associated with unprotected, promiscuous sexual activity and an increased risk of contracting sexually transmitted diseases. More recently, “bath salts” (e.g. “Ivory Wave”, “Cloud 9”, “Vanilla Sky”) that contain mephedrone, methylenedioxypyrovalerone (MDPV), or other synthetic chemicals related to cathinone (an amphetamine-like stimulant found in the khat plant) have become popular; they are often snorted but can be injected, smoked or ingested orally.
Benzodiazepines
Benzodiazepines are among the most frequently prescribed medications in the US and the UK, where surveys indicate that ~10% of the population uses benzodiazepine sedatives/anxiolytics regularly. Although they are only mild euphoriants, benzodiazepines, in particular flunitrazepam (Rohypnol ® ; “roofies”), are commonly misused by polydrug addicts, alcoholics, and recreational drug users. Benzodiazepines are ingested (often with alcohol), snorted, or occasionally injected. They can lead to a decrease in alertness and a lack of coordination. Other side effects of benzodiazepines include disinhibition, anterograde amnesia, depression and confusion, and with an overdose or intravenous use, hypotension and hypoventilation.
Cannabis
Cannabis (“marijuana”, “pot”, “grass”, “herb”, “weed”, “bud”, “Mary Jane”) is the most frequently self-administered illicit drug. However, medical marijuana is currently legal in over 25 states in the US and recreational use is legal in seven states . Cannabis is a mixture of dried shredded leaves and flowers of the Cannabis sativa plant, which contains the chemical delta-9-tetrahydrocannabinol (THC). It is usually smoked as a cigarette or through a pipe or bong. Marijuana cigarettes may be laced with other drugs, such as crack or heroin. The minimal amount of THC required to produce a perceptible psychoactive effect is ~10 mcg/kg body weight. Altered perception may be accompanied by an impairment of concentration, psychomotor coordination, and/or short-term memory. Arteritis has also been reported , and it may represent a particular form of Buerger disease, with cannabis acting as a cofactor in young smokers.
In many countries, including the US, there has been an increase in the use of synthetic cannabinoids (“K2”, “Spice”, “Black Mamba”), which also bind the THC receptor, but may have increased vasoactive and psychoactive effects, including psychosis. Cannabinoids can be sprayed onto dried plants or inhaled via vaporizer electronic cigarettes.
Cocaine
Cocaine (“coke”, “blow”, “toot”, “flake”, “snow”, “bump”) is an alkaloid stimulant and topical anesthetic which is extracted from the leaves of the Erythroxylon coca shrub. Crack (“base”, “rock”, “hard rock”, “sugar block”), a freebase form of cocaine, is more addictive than heroin. It is produced by dissolving cocaine in water and baking soda and then heating the mixture until it crystallizes. Cocaine is injected or snorted, while crack is smoked.
In addition to Raynaud phenomenon, cocaine use has been associated with cutaneous small vessel vasculitis (leukocytoclastic vasculitis), necrotizing granulomatous vasculitis, acute generalized exanthematous pustulosis, and Stevens–Johnson syndrome . Its use can also lead to a number of cardiovascular side effects – Buerger disease, hypertensive crisis, myocardial or cerebral infarction, and ventricular arrhythmias. Cocaine adulterated with levamisole has been associated with neutropenia and ischemic vasculopathy with necrotizing purpura and ulceration (see below).
Gamma-Hydroxybutyrate
Gamma-hydroxybutyrate (GHB; “liquid X”, “liquid ecstasy”, “liquid G”, “fantasy”, “gamma-oh”), a “party drug”, is a rapid-acting CNS depressant popular among revelers for its relaxant, euphoric, and purported aphrodisiac properties. GHB can lead to a loss of consciousness as well as induce amnesia, and like flunitrazepam it is used as a “rape drug”. Because it reportedly promotes muscle mass and has been shown to elevate human growth hormone in vivo, GHB is also misused by bodybuilders.
Lysergic Acid Diethylamide
Lysergic acid diethylamide (“LSD”, “acid”), a hallucinogen, is manufactured from lysergic acid found in ergot, a fungus that grows on rye and other grains. It is often sold in single-dose (20 to 80 mcg) squares of blotter paper. LSD causes an altered experience of time, sense and memory, usually within 30–90 minutes after ingestion. Changes in auditory and visual perception (e.g. moving geometric patterns) are typical. In addition to pupil dilation and tachycardia, patients may develop sweating, sialorrhea, piloerection, and a strong metallic taste.
Opioids (Includes Opiates)
Also known as diacetylmorphine, heroin (“junk”, “smack”, “horse”, “H”, “scag”, “skag”), the fastest acting of all opiates, is three times more potent than morphine and accounts for much of the illicit opiate abuse in the US. Because of its lipid solubility, it crosses the blood–brain barrier rapidly, prompting a “rush” within 7 to 8 seconds after intravenous injection or 10–15 minutes after being snorted or smoked. There has been a growing tendency to sniff, snort (“shebang”) or smoke (“chase the dragon”) heroin rather than inject it intravenously (“shoot up”) or subcutaneously (“skin pop”). Opiate addicts may alternate injections of heroin and cocaine (crisscrossing) or inject highly addictive “speedballs” that combine the two drugs. Methadone, an oral synthetic opioid with a half-life between 24 and 48 hours, is widely used as a substitute for heroin in narcotic treatment programs and for chronic pain.
Opioids remain the leading cause of fatal overdoses, including methadone and other more commonly prescribed opioids. Fentanyl (“TNT”, “Apache”), a narcotic analgesic that is 50 to 100 times more potent than morphine, is particularly prone to overdosing. Heroin, which nowadays is less expensive than illegal prescription opioids, is increasingly being laced with fentanyl and its analog carfentanil such that first responders routinely carry naloxone (Narcan ® ). Buprenorphine, a more potent and longer-lasting analgesic than morphine, appears to act as a partial agonist of µ and κ opioid receptors, but tolerance with chronic use may not develop, presumably due to the lack of δ-agonist activity.
Pentazocine is an oral benzomorphan opioid antagonist with a lower risk of drug dependence than opiates, and ingestion of pentazocine may precipitate withdrawal symptoms in persons physically dependent on opioids. However, when tablets are crushed, diluted, and then injected in combination with the antihistamine tripelennamine (Pyribenzamine ® ), the euphoric effects are similar to those produced by heroin. The side effects are similar to those of morphine, but pentazocine may be associated with a greater risk of hallucinations. Severe necrosis and secondary infection of the skin and subcutaneous tissue, including underlying muscle, may develop at repeated injection sites of pentazocine.
Desomorphine (“krokodil”) is a fast-acting morphine derivative that is eight times more potent than morphine . The drug can be synthesized by combining red phosphorus from match strikers with codeine and iodine derived from over-the-counter medications; unfortunately, it is frequently contaminated with these and other agents . Injection of this “flesh-eating drug” can cause serious damage to the skin, blood vessels, bone and muscles, leading to limb amputation in long-term users . Of note, the tissue injury is due to iodine, phosphorus, and other toxic substances that remain after synthesis, not the opioid itself .
Anabolic Steroids
Anabolic steroids promote the growth of skeletal muscle and the development of male sexual characteristics. They are ingested (oxandrolone, oxymetholone, stanozolol) or injected (nandrolone, testosterone, boldenone) intramuscularly by bodybuilders to increase muscle mass and by athletes to boost physical performance. Physical and psychological dependence can develop after habitual use. Cardiovascular disease, hepatic disorders (e.g. peliosis hepatis, hepatic adenomas), infectious diseases (due to needle sharing), and perhaps mood disorders are among the long-term complications of anabolic steroid misuse. The cutaneous side effects of these and other drugs are outlined in Table 89.2 .
| CUTANEOUS SIGNS OF DRUG ABUSE | ||
|---|---|---|
| Lesion type | Route(s)/associated drug(s) | Other associated signs |
| Skin tracks | IV | Lymphedema |
| Skin popping scars | sc or dermal | Lymphedema |
| Ulcerations | IV/cocaine IV/propoxyphene sc/barbiturates sc, IM/pentazocine (± tripelennamine) | Circumferential pigmented bands (IV administration) |
| Retiform purpura with ulceration | Snorting, IV/cocaine adulterated with levamisole Smoking/crack cocaine adulterated with levamisole | Neutropenia, leukopenia Arthralgias, pulmonary hemorrhage, seizures, glomerulonephritis Autoantibodies: ANA, ANCAs (including anti-PR3, elastase), anti-dsDNA, lupus anticoagulant |
| Sclerosis | sc, IM/pentazocine sc/barbiturates sc/cocaine | |
| Palmar and digital hyperkeratosis | Smoking/crack cocaine | Madarosis Linear and circular black plaques on the fingers and palms Cuts and blisters on the lips |
| Nasal verrucae | Snorting/cocaine or heroin | Nasal irritation Septal perforation |
| Pseudoaneurysm | Arterial injection | Petechiae/purpura Local suppuration Reduced peripheral pulses |
| Cellulitis | IV, sc, intradermal | Osteomyelitis and septic arthritis |
| Cutaneous Pseudomonas infection | IV, sc, intradermal/heroin sc/pentazocine ± tripelennamine | Folliculitis |
| Wound botulism ( Clostridium botulinum , especially type A) | IM, sc/black tar heroin or quinine-adulterated heroin | Lymphedema Skin popping scars |
| Excoriations & self-induced ulcers | Methamphetamine | Dry leathery skin Red dry nose Dental caries/loss of teeth Weight loss Paranoia |
| Formication or delusions of parasitosis | Cocaine (chronic) Methamphetamine | |
| Pruritus | Heroin Cocaine (chronic) Methamphetamine | With heroin: Flushing Pseudoacanthosis nigricans |
| Papulopustular acneiform eruption | MDMA (ecstasy) | |
| Acne vulgaris | Anabolic steroids | Coarse skin Hirsutism Male and female pattern alopecia Gynecomastia (in men) Testicular atrophy Clitoral enlargement |
| Methamphetamine Marijuana | Excoriations | |
| Perinasal and perioral irritant dermatitis | Sniffing of volatile solvents and inhalants | |
Pathophysiology of Addiction
Administration of addictive drugs, directly or indirectly, leads to an increase in dopamine activity within the mesolimbic system (reward circuit) as well as the frontal cortex, anterior cingulate, and hippocampus. This is thought to play a role in incentive salience and craving. In addition, MRI studies have documented progressive loss of frontal lobe volume in both cocaine- and heroin-dependent addicts and this may lead to unrestricted behaviors.
Epidemiology
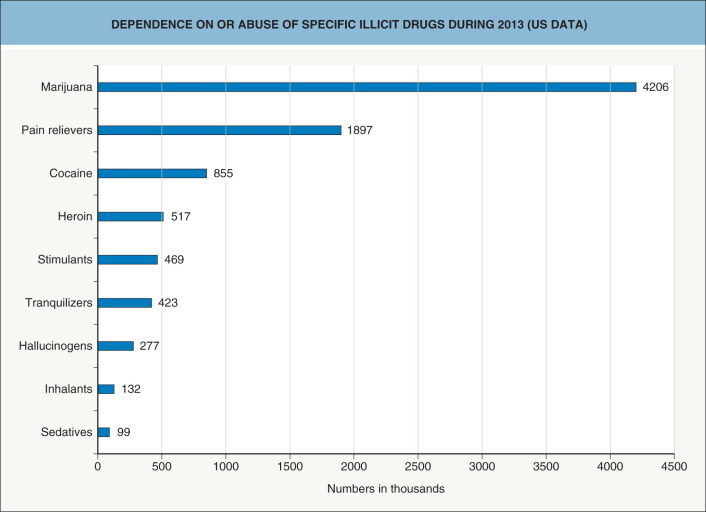
Globally, it is estimated that in 2012, an estimated 250 million people, corresponding to 4–5% of the world’s population aged 15–64, had used an illicit drug at least once in the previous year . Drug abuse is a problem in both high- and low-income countries ( Fig. 89.1 ). According to the National Survey on Drug Use and Health, in 2015, an estimated 27.1 million Americans 12 years of age or older were current (during the past month) illicit drug users, representing ~10% of this population.
Clinical Features
Scars
Intravenous drug users have a number of recognizable stigmata, identifying their habit to anyone with experience in illicit drug use . The most prominent of these are “skin tracks”, which represent scarred veins with overlying hyperpigmentation ( Fig. 89.2 ); inflammation from repeated non-sterile injections as well as injections of irritating drugs and adulterants lead to scarring. Intravenous drug users also have trails of punctures, hemorrhagic crusts, and ecchymoses along the veins of their extremities . The veins of the arms are often used initially for injections, and when these become scarred, drug is injected into the vessels of the hand, digits, lower extremities, neck, axillae, and eventually into any visible vein or palpable artery . Some parenteral drug users purposefully inject the veins in their legs, feet and groin in order to avoid the development of scars on exposed parts of the body.

When attempting to inject veins, accidental extravasation can occur, leading to local tissue injury. In addition, as patent vessels become scarce, drugs are injected intradermally or subcutaneously . The resulting “skin popping” scars are depressed, irregular or circular, and often dyschromic ( Fig. 89.3 ). In some users, indurated, hypertrophic or keloidal scars form at these sites . Drug users who cannot find intact veins may also rub powdered drugs into lacerations created with razor blades or knives.
Adulterants such as lactose, mannitol, dextrose, baking soda, and flour are used to dilute (“cut”) heroin and other powder drugs . Many adulterants, especially quinine and dextrose, are highly sclerosing and more damaging to tissue than pure heroin . Quinine is a popular adulterant because it has a bitter taste similar to heroin and it accentuates the narcotic euphoria. It is destructive to lymphatics and repeated injections can lead to chronic, non-pitting hand edema, referred to as puffy hand syndrome. Levamisole-adulterated cocaine is associated with the development of retiform purpura and cutaneous necrosis (see below).
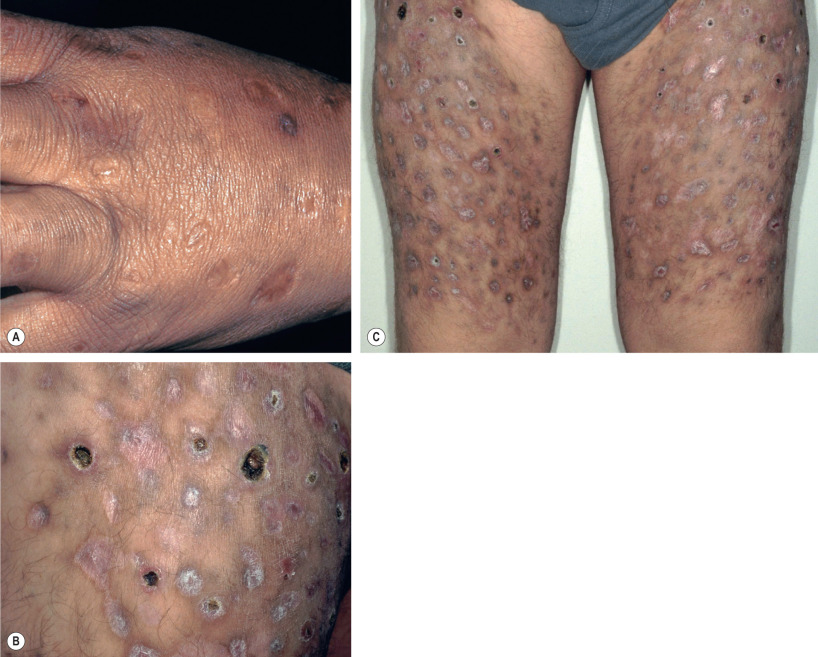
The risk of thrombophlebitis and skin necrosis from injections of propoxyphene is so high that even the most determined addict ceases use of the drug after only a few weeks (see Table 89.2 ) . Cocaine is highly vasoconstrictive and even inhaled freebase cocaine has induced skin and muscle infarction. Due to their alkalinity, barbiturates, when injected into the skin, cause tender, erythematous, indurated plaques, which break down into deep ulcers and frequently become infected. Injection of the antihistamine tripelennamine, usually injected in combination with pentazocine or another opioid, also induces tissue necrosis and ulceration. Pentazocine injection may cause brawny, sclerodermatous skin thickening and large, irregularly shaped, deeply penetrating ulcers that may extend to muscle and then heal with significant atrophy ( Fig. 89.4 ) . Pentazocine-related cutaneous sclerosis develops more commonly in addicts with diabetes mellitus .

Fibrous myopathy, joint restriction, muscle contractures, brachial plexus neuropathy, inflexible ankylosis, and suppurative tenosynovitis are musculoskeletal and neurologic complications from intracutaneous and intravenous injections .
Bacterial Infections
Unless they participate in needle exchange programs, parenteral drug users rarely use sterile technique and may share needles, predisposing them to infections ( Table 89.3 ). Skin and soft tissue infections are the most common disorders for which drug addicts seek healthcare or are hospitalized . Amongst 127 intravenous drug users, 41% had developed cellulitis, 32% an abscess with cellulitis, 16% an abscess alone, 10% infected skin ulcers, 7% necrotizing fasciitis, and 5.5% septic phlebitis with cellulitis . The most common presentation of cellulitis is an erythematous, tender, warm, edematous, indurated plaque ( Fig. 89.5 ); however, only tenderness and edema may be apparent initially, and in darkly pigmented skin, erythema may be difficult to appreciate. In contrast to the general population, cellulitis more frequently involves the upper extremity.
| INFECTIOUS COMPLICATIONS OF DRUG ABUSE | |
|---|---|
| Type of infection | Organisms and/or associated features |
| Bacterial | |
| Abscesses and cellulitis |
|
| Necrotizing fasciitis |
|
| Pyomyositis | |
| Septic thrombophlebitis |
|
| Septic arthritis |
|
| Osteomyelitis |
|
| Endocarditis |
|
| Fungal | |
| Candidiasis |
|
| Aspergillosis |
|
| Zygomycosis |
|
| Viral | |
| Hepatitis |
|
| HIV | |
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


