Abstract
The following case studies are presented to reinforce what you have learned from reading Principles of Dermatology .
Chapter Contents
Case 1 – White Spots
What Is the Most Likely Diagnosis?
What Test Would You Do?
How Would You Treat This Patient?
Case 2 – Bleeding Growth
What Is Your Differential Diagnosis of This Lesion?
What Would You Do Now?
How Would You Determine the Prognosis of This Patient?
Case 3 – Recurrent Vesicles
What is Your Diagnosis?
What Laboratory Tests Would You Do?
What Are Your Recommendations to This Patient?
Case 4 – Papulovesicular Rash
What Is Your Differential Diagnosis?
How Would You Treat This Patient?
How Would You Prove Your Diagnosis?
Case 5 – Fever and Purpura
What Do You See?
What Is the Most Likely Diagnosis?
How Would You Prove It?
How Would You Treat It?
Case 6 – Firm Nodule
What Is the Most Likely Diagnosis?
What Should Be Done Next?
Do You See Any Other Skin Lesions of Note?
Case 7 – Generalized Itching Papules
What Do You See?
What Is the Most Likely Diagnosis?
How Would You Confirm It?
Case 8 – Hair Loss
What Is Your Differential Diagnosis?
What Would You Do Now?
How Would You Treat This Patient?
Case 9 – Pearly Nodule
What Is Your Differential Diagnosis?
How Would You Treat It?
What Precautions Should This Patient Take in the Future?
Case 10 – Generalized Erythema
What Is the Most Likely Diagnosis?
If You Suspect a Drug Reaction, What Is the Most Likely Drug?
How Can You Prove It?
Case 11 – Ulcer Behind the Ear
What Is Your Differential Diagnosis of This Ulcer?
What Would You Do Now?
What Is the Best Treatment?
Case 12 – Scaling Rash
What Is Your Differential Diagnosis?
What Test Would You Do Next?
Case 13 – Lip Ulcer
How Would You Complete the Physical Examination?
What Is Your Most Likely Diagnosis?
How Would You Confirm It?
Case 14 – Pustules and Papules Surrounding an Ulcer
Describe What You See
What Is Your Differential Diagnosis?
What Is the First Diagnostic Test You Would Do?
How Would You Treat It?
Case 15 – Scaling Rash on Head, Trunk, and Arms
What Is Your Differential Diagnosis?
What Would You Do Now?
How Would You Treat This Patient?
Case 16 – Crusted Erosions on the Dorsum of the Hands and Forearms
What Is Your Differential Diagnosis?
What Would You Do Now?
How Would You Treat This Patient?
Case 17 – Nodule on the Lower Leg
What Is Your Differential Diagnosis?
What Diagnostic Work-Up Would You Do Now?
What Is Your Diagnosis and How Would You Treat This?
What Is the Most Likely Diagnosis?
This patient has a typical history for tinea versicolor. Scratching the affected areas elicited a fine, crumbly scale, further heightening the suspicion of tinea versicolor.

What Test Would You Do?
The potassium hydroxide (KOH) preparation is diagnostic, revealing numerous short hyphae and spores.
How Would You Treat This Patient?
Fluconazole was prescribed in a single 200 mg dose and repeated again in 2 weeks. The skin gradually repigmented over the following 3 months. Prevention of recurrence can be achieved with periodic washing of the affected areas with zinc pyrithione or selenium sulfide shampoo. Localized areas may be treated with Micatin cream.
What Is Your Differential Diagnosis of This Lesion?
This 6-mm nodule has the blue-black color and eroded surface typical of a nodular malignant melanoma. The differential diagnosis includes blue nevus, nodular pyogenic granuloma, and hemangioma.
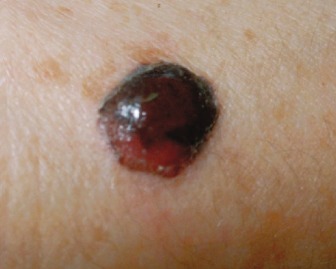
What Would You Do Now?
An excisional biopsy revealed histopathologic changes typical of a nodular melanoma invading to a depth of 3.7 mm. The remainder of the skin examination and a general physical examination were normal. A sentinel lymph node biopsy was free of tumor. A 2.0-cm margin of normal skin was excised around the biopsy scar.
How Would You Determine the Prognosis of This Patient?
The prognosis of malignant melanoma is related to tumor thickness. Because this is a thick melanoma, the patienťs prognosis is poorer despite having negative sentinel lymph nodes.
What Is Your Diagnosis?
These grouped vesiculopustules on an erythematous base are typical of herpes simplex virus (HSV) infection. In addition, the history of a recurrent vesicular eruption in the same place is classic for this viral infection. No other diagnosis should be seriously considered.

What Laboratory Tests Would You Do?
A Tzanck preparation is all that is necessary to confirm the clinical diagnosis. If still in doubt, a viral culture can be obtained.
What Are Your Recommendations to This Patient?
Acyclovir, valacyclovir, or famciclovir may be used in patients with frequent recurrences. These medications reduce the duration of viral shedding and time to healing of lesions when administered early in the course of a recurrent episode.
What Is Your Differential Diagnosis?
This acute eczematous eruption confined to the area beneath the dressing is typical of contact dermatitis. A less likely cause would be a fungal or bacterial infection since pustules are absent.

How Would You Treat This Patient?
The dermatitis cleared when the povidone-iodine dressings were replaced with saline compresses and a topical steroid cream.
How Would You Prove Your Diagnosis?
The patient had no history of iodine sensitivity. However, he had been applying the povidone-iodine dressing for 2 weeks, which is sufficient time to develop sensitivity to this compound. A patch test to 10% povidone-iodine solution was positive, confirming the diagnosis of allergic contact dermatitis.
- 1.
Topical medicaments are an important cause of allergic contact dermatitis and should be suspected when an eczematous eruption occurs in areas that conform to application of the medication.
- 2.
Avoidance of the allergen is the treatment of choice. Topical steroids hasten resolution of allergic contact dermatitis.
- 3.
Patch testing confirms the diagnosis of allergic contact dermatitis.
What Do You See?
The lesions (shown here on the thigh) are palpable and purpuric. Petechiae are also present.

What Is the Most Likely Diagnosis?
In a patient with fever and palpable purpura, sepsis is the first and most important diagnosis to consider. In an infant or young child, bacterial meningitis is the most likely diagnosis, particularly if the child has signs of meningeal irritation or altered consciousness.
How Would You Prove It?
Blood and cerebrospinal fluid (CSF) should be obtained immediately for bacterial cultures. In addition to culturing the CSF, a Gram-stain, cell count and differential, glucose, and protein should be performed.
How Would You Treat It?
This is a medical emergency and empiric antibiotic therapy must be administered promptly beginning with vancomycin plus cefotaxime or ceftriaxone.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


