Abstract
The nail is a specialized keratinized appendage found on the dorsum of each finger and toe. It protects the distal phalanx against trauma, is used for fine grasping and scratching, and has esthetic value. The diagnosis of nail diseases can be difficult because a single disease can cause widely varying changes of the nail and, conversely, because a given nail malformation can be the expression of a variety of diseases. Numerous disorders may affect the nail, including cutaneous and systemic diseases, tumors, infections, hereditary disorders, physical factors, and drugs. In this chapter, the four most common causes of nail disease are discussed: fungal infection, psoriasis, paronychia ( Table 21.1 ), and ingrown toenail.
Fungal Infection
- 1.
Confirm the diagnosis with PAS stain, culture or KOH preparation
- 2.
Cure requires oral therapy
Definition
Onychomycosis and tinea unguium are synonyms for infection of the nail with dermatophytic fungi. The most common etiologic dermatophytes are Trichophyton rubrum and T. mentagrophytes .
| Physical Examination | Laboratory Test | |||||
|---|---|---|---|---|---|---|
| Frequency (%) a | Pits | Brown Stains | Differential Diagnosis | KOH | Culture | |
| Fungal infection | 0.4 | Absent | Present | Psoriasis Trauma Aging Secondary to eczema | Positive | Positive |
| Psoriasis | < 0.1 | Present | Present | Fungus Trauma Aging Secondary to eczema Alopecia areata (pits) | Negative | Negative |
| Paronychia | 0.3 | Absent | Absent | Herpes simplex | Negative Positive | Bacterial Candida albicans |
a Percentage of new dermatology patients with this diagnosis seen at the Hershey Medical Center Dermatology Clinic, Hershey, PA.
Incidence
The prevalence of onychomycosis is 22 per 1000 population. Some 20% of persons in the United States between 40 and 60 years of age have onychomycosis. The most common sites of infection are the toenails, especially in the elderly.
History
The onset of onychomycosis is slow and insidious. The condition is often asymptomatic, but it can also cause pain in the affected toe, nail-trimming problems, discomfort when wearing shoes, and embarrassment because of the nail’s distorted appearance.
Physical Examination
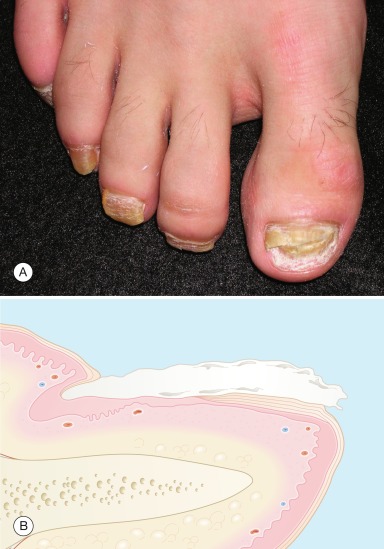
Toenail infection is more frequent than fingernail infection, and it is uncommon for all 10 nails to be involved. Dermatophytes most often infect the distal nail bed and undersurface of the distal nail, with resulting discoloration (white, yellow, or brown) of the nail plate and accumulation of subungual debris with separation of the plate from the nail bed ( Fig. 21.1A ). Less often, dermatophytes infect the top surface of the nail plate and cause a white, crumbly surface (superficial white onychomycosis) to develop. Neither type of infection produces much inflammatory reaction. Proximal white subungual onychomycosis, infection of the proximal nail plate, is a marker of human immunodeficiency virus (HIV) infection.
Onychomycosis is associated with tinea pedis and tinea manuum.
Differential Diagnosis
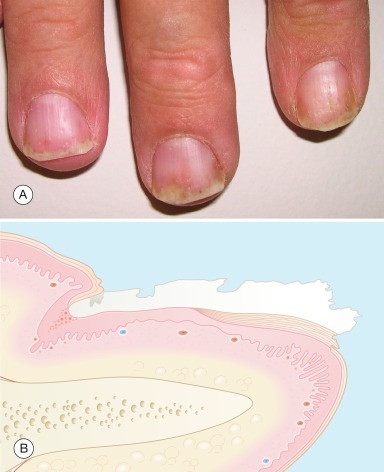
Often, the nail changes of onychomycosis cannot be distinguished clinically from those of nail dystrophy caused by psoriasis (see Fig. 21.4 ), eczema of the digits, trauma, and aging. Associated skin findings and fungal studies differentiate these entities.
- ●
Psoriasis
- ●
Eczema
- ●
Trauma
- ●
Aging
Laboratory and Biopsy
The most sensitive method of confirming the diagnosis of onychomycosis is a periodic acid-Schiff (PAS) stain of nail clippings.
A potassium hydroxide (KOH) preparation or fungal culture can alternatively be done. Compared with skin scrapings, more time must be allowed for the KOH to dissolve thin nail specimens before microscopic examination. If the infection is in the nail bed or the deeper portion of the nail plate, scrapings should be obtained from as far back under the nail as possible ( Fig. 21.1B ).
Therapy
Topical antifungal agents (ciclopirox, tavaborole) are ineffective (< 20% clearing) in treating onychomycosis. Oral therapy with terbinafine (Lamisil) or itraconazole (Sporanox) should be given. Studies suggest that terbinafine is the most effective agent. The nail will not look completely normal at the end of treatment. Because terbinafine and itraconazole remain in the nail for months after therapy, retreatment should not be considered for approximately 6 months for fingernails and 12 months for toenails. In many individuals with asymptomatic onychomycosis of the toenails, systemic therapy is neither requested nor suggested. The risks and cost may outweigh any possible benefit.
Asymptomatic onychomycosis of toenails needs no treatment.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


