Salvage Hip Surgery in Skeletally Mature Neuromuscular Patients
Brian Snyder
Pathophysiology of Hip Subluxation
Pathophysiology and pathoanatomy differs from developmental hip dysplasia
Hips are normal at birth
Muscle imbalance → bony deformity→ hip dysplasia
The lateral and posterolateral acetabulum is most often deficient
Natural history = increasing dysfunction with remaining growth and progressive subluxation
Progressive subluxation adversely affects hygiene, sitting, upright posture ± gait
Leads to pain in early adolescence
Surgical Considerations
Coexisting hip and spine pathology (hip/spine syndrome)
Fixed deformities (contractures, instability, and dysplasia) of the hip joint result in pelvic obliquity with subsequent development of secondary lumbar scoliosis
“Windswept” hips
Adduction one hip, abduction of the other
Pelvic obliquity ± torsion/rotation (torsional dystonia)
Presence of scoliosis and significance?
Chicken versus egg
↑ Pelvic obliquity → compensatory lumbar scoliosis
↑ Lumbar curve → pelvic obliquity → “windswept” hips
Salvage surgery is designed to help reduce pain, but pain can be present after surgery for 6 to 12 months, and this needs to be communicated to the families preoperatively
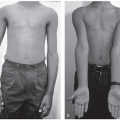
Physical Examination
Assess hip range of motion—symmetric adduction contracture = loss of hip abduction ± flexion contracture; internal and external rotation with hips in extension = femoral version
Asymmetric abduction = windswept hip deformity, pelvic obliquity, scoliosis
+ Galeazzi, Ortolani signs = hip instability (subluxation/dislocation)
Look for skin problems in deep creases and assess prominence of dislocated hip
Assess scoliosis and upper extremity contractures and consider access issues for time of surgery
Decision-Making for Hip Salvage Surgery
Total hip replacement
Reserved for Gross Motor Function Classification System (GMFCS) I/II patients with severe femoral head deformity
Chiari pelvic osteotomy
Consider for GMFCS III/IV with moderate femoral head deformity but reducible head
Femoral head resection (Castle procedure)
Consider for our medically complex children, supine positioning, quick surgery <1 hour, prophylax with radiation to prevent heterotopic ossification
McHale valgus subtrochanteric osteotomy and Castle procedure
Consider for GMFCS III/IV children who enjoy standing to create a pelvic support osteotomy to facilitate standing post-op
“Schoenecker” Girdlestone procedure through a surgical dislocation approach
Most common surgical approach for GMFCS IV/V children with minimal standing and significant pain
Preoperative Medical Considerations
Pulmonary assessment—look for presence of restrictive lung disease
Forced vital capacity (FVC) < 25%—higher risk of complications
Upper airway obstruction—tonsillectomy/adenoidectomy
Nutrition—poor nitrogen balance = poor wound healing
Absolute neutrophil count >1200, serum albumin >3
G-tube—often helps with postoperative course
Seizure control—be mindful of medications which increase bleeding and delay clotting
Gastrointestinal (GI) disorders—dysphagia, constipation—make sure clean out preoperatively
Osteopenia—poor purchase bone implants
Dual-energy x-ray absorptiometry (DEXA) scan to measure bone density
Vitamin D supplement ± bisphosphonates (if previous fragility fractures)
Perioperative Management
Epidural anesthesia intraoperatively, 2 to 3 days postoperatively
Antifibrinolytic tranexamic acid administered to decrease intraoperative blood loss
Diazepam for postoperative muscle spasms
Hinged hip abduction brace or A-frame short leg cast for 3 weeks
NO SPICA
Be vigilant for skin breakdown, pressure ulcers
Chiari Osteotomy
Operative Indications
Chiari osteotomy is a “salvage” osteotomy for acetabular dysplasia in the painful, unstable hip
Indicated for hips where congruous reduction is not possible because of arthrosis or femoral head asphericity that prevents use of more standard rotational periacetabular osteotomies
Indicated for household ambulators (GMFCS III/IV)
Goals are improved femoral head coverage, stable articulation
Contraindications
Severe arthrosis
Significant proximal femoral head migration
Cannot perform this bilaterally at 1 surgical setting for fear of creating pelvic discontinuity
Equipment
Standard retractors for hip and pelvic surgery, cerebellar retractors or Charnley if available
A series of angled osteotomes including Ganz and Mast chisels
Radiolucent retractors
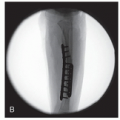
Large fragment long pelvic screws or Steinman pins and Kirschner wires (K-wires) can be used for osteotomy fixation
Positioning
The patient is positioned supine on the operating room table
Sloppy lateral with a bump can also be helpful if possible
Free drape the operative extremity from the costophrenic margin superiorly, medially to the ipsilateral border of the perineum, and laterally to the border of the buttocks
Surgical Approach
The ilioinguinal approach is the exposure of choice for this osteotomy
The incision begins approximately 1 to 2 cm below the iliac crest and extends medially 1.5 to 2 cm distal and medial to the anterior superior iliac spine (ASIS)
The lateral fibers of the external oblique muscle overhang the lateral ilium and are reflected off the ilium with electrocautery or a #15 blade. Care is taken to clear the iliac apophysis of soft tissue and maintain meticulous hemostasis
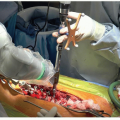
Distally the interval between the sartorius and tensor fascia lata (TFL) is identified. The TFL fascial compartment is opened, and muscle is stripped directly off the intermuscular septum with a Cobb or periosteal elevator (Figure 39.1)
The TFL is retracted laterally, and the intermuscular septum and sartorius muscle are retracted medially
At this level, the lateral femoral cutaneous nerve of the thigh lies within the sartorial muscle compartment and is not visualized; however, the nerve lies under the fascia between the two muscles and care must be taken to avoid injury during the approach and when closing to avoid a painful neuroma
Blunt dissection of TFL is continued proximally to the ilium and to the level of the anterior inferior iliac spine (AIIS)
Continue subperiosteal dissection anteriorly from ASIS inferiorly to the AIIS. Identify the direct head of the rectus femoris inserting into the AIIS, and locate the bifurcation of the indirect head
At this point, the iliac apophysis is split in the midline, the gluteal muscles are subperiosteally dissected off the outer table ilium and the iliacus muscle is dissected subperiosteally off the inner table of the ilium, and a moist sponge is packed tightly between the ilium and dissected muscles to aid in retraction and hemostasis
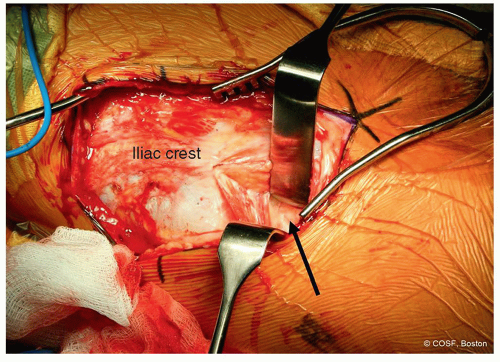
Figure 39-1 ▪ The anterior hip interval between tensor fascia lata and sartorius is developed; staying lateral in the tensor compartment decreases the risk of iatrogenic lateral lfemoral cutaneous nerve injury as highlighted by black arrow. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
Now the outer table is dissected away subperiosteally from the abductor musculature inferiorly until firm resistance is met. This resistance indicates the insertion of the indirect head of the rectus femoris on the lateral aspect of the hip capsule
Return back to the bifurcation of the direct and indirect heads of the rectus femoris tendon. Ligate the indirect head at the bifurcation and follow it posterolaterally to the suspected inserted into the lateral hip capsule
Dissect posteriorly along the outer and inner tables of the ilium to the level of the greater sciatic notch. Use a lane retractor to subperiosteally elevate the superior gluteal artery and sciatic nerve away from the apex and anterior margin of the notch
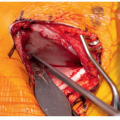
Incise the periosteum along the superior border of the indirect head of rectus femoris. This will allow subsequent release of the abductor minimus off the superior capsule to allow for proper chisel placement for the Chiari osteotomy (Figure 39.2)
At this point, use fluoroscopy to ensure that you have not been misled by a pseudoacetabulum and your dissection has carried you down to the acetabular margin. Visualization at this point of the operation is paramount
Techniques in Steps
Creating the Osteotomy
Essentially, the osteotomy is creating a transverse acetabular “fracture” where both the anterior and posterior acetabular columns are cut and the ilium is displaced posterolaterally over the hip joint capsule forming a shelf
The osteotomy is a curvilinear in the supra-acetabular region. It begins at the anterior ilium at the level of the AIIS and traverses the capsular edge of the acetabulum to terminate at the sciatic notch (Figure 39.3)
We use a modification advocated by John Hall where the osteotomy is truly curvilinear. The posterior limb of the osteotomy is curved distally aiming a centimeter below the apex of the sciatic notch to increase posterior coverage, thus making the osteotomy more dome-like in appearance (Figure 39.4)
The start of the osteotomy is determined anatomically and radiographically
Anatomically, the osteotomy is started anteriorly at the capsular margin; this point is double-checked with fluoroscopy to ensure that we are not within the false acetabulum
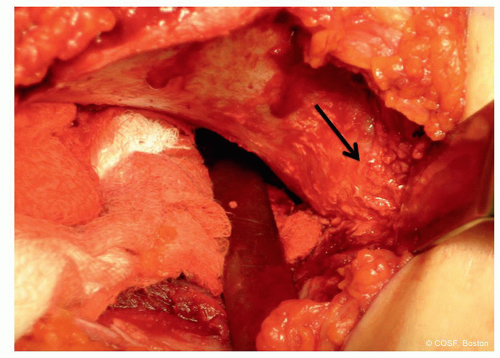
Figure 39-2 ▪ Dissection down to the lateral capsule is critical to facilitate an acceptable Chiari osteotomy; this often confirmed clinically, by taking down the indirect head of the rectus tendon to expose the lateral capsule, as noted by black arrow, and radiographically to guarantee that the dissection is inferior enough. (Courtesy of Children’s Orthopaedic Surgery Foundation.)
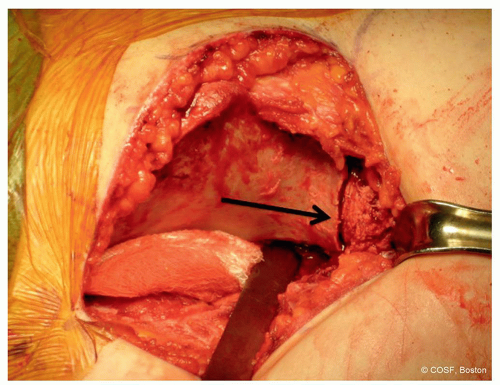
Figure 39-3 ▪ Historically the osteotomy has been described as a straight osteotomy; with a Gigli saw; however, we have adopted the modifications described by Dr Hall, which endorses much of a semicircular osteotomy as noted by black arrow. (Courtesy of Children’s Orthopaedic Surgery Foundation.)Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access