Abstract
Rosacea is a common chronic facial dermatosis, most often affecting individuals with lighter skin phototypes and first appearing during middle age. Proposed pathomechanisms include abnormal cutaneous innate immune responses and neurovascular dysregulation. Clinical features are varied, from frequent facial flushing and telangiectasia to papules and pustules to phymatous changes and ocular inflammation. To assist in management, rosacea has been classified into four clinical subtypes: (1) erythematotelangiectatic (ETTR); (2) papulopustular; (3) phymatous; and (4) ocular. Treatment options for ETTR include vascular laser therapy and topical α-adrenoreceptor agonists. Topical and oral antibiotics, in particular low-dose doxycycline, as well as topical ivermectin are used to treat papulopustular rosacea. General skin care (e.g. sun avoidance), patient education on the need for maintenance therapy, and psychologic support are important aspects of the therapeutic approach to rosacea.
Keywords
rosacea, acne rosacea, erythematotelangiectatic rosacea, papulopustular rosacea, phymatous rosacea, ocular rosacea, rhinophyma, granulomatous rosacea, lupus miliaris disseminatus faciei, flushing, perioral dermatitis, periorificial dermatitis, aberrant cutaneous innate immunity, Demodex , neurovascular dysregulation
Introduction
The term “ rosacea ” encompasses a constellation of clinical findings, with the key components being persistent facial erythema and inflammatory papulopustules. Additional features are facial telangiectasias, a tendency for frequent facial flushing (sometimes referred to as “pre-rosacea”), non-pitting facial edema with erythema, ocular inflammation, and phymatous changes. The latter predominantly affect the nose and rarely the ears, forehead, chin, or eyelids. In 2002, rosacea was classified into four clinical subtypes : (1) erythematotelangiectatic; (2) papulopustular; (3) phymatous; and (4) ocular.
There is also a granulomatous variant in which more monomorphous and persistent skin-colored to dull red–brown facial papules are seen. Some authors consider rosacea conglobata , characterized by an eruption of inflammatory cystic lesions that heal with scarring and rosacea fulminans (pyoderma faciale) to be within the rosacea spectrum. In rosacea fulminans, an explosive onset of inflammatory papules and pustules is superimposed on a background of facial erythema, usually occurring in young women and sometimes during pregnancy .
History
Robert Willan is credited with the earliest medical descriptions of “acne rosacea”, detailing what is nowadays classified as papulopustular rosacea . Like acne vulgaris, rosacea was originally thought to have a “seborrheic” pathogenesis. It was Radcliff-Crocker who later postulated that repeated flushing leads to dilated leaky facial blood vessels with subsequent inflammatory skin changes.
Epidemiology
Some publications regarding the frequency of rosacea within the general adult population may be invalid because of inadequate disease definitions . In a 1989 study of over 800 office workers in Sweden, the prevalence of rosacea was found to be 10% . The majority of affected individuals had facial erythema and telangiectasias without inflammatory skin lesions, presumably representing erythematotelangiectatic rosacea (ETTR); changes consistent with papulopustular rosacea (PPR) were observed in 1.8%. Utilizing a consensus definition of PPR , a population study of 1000 individuals in Ireland detected a point prevalence of 2.7% . A similar rosacea point prevalence rate of 2.3% was noted in a review of 90 880 German workers, although in this study clinical subtypes were not defined .
The prevalence of rosacea in patients with skin of color is not well studied but appears to be less common than in those with skin phototypes I and II . Epidemiologic studies from countries where darkly pigmented individuals predominate population-wise suggest that the prevalence is far lower than in countries where the population is predominantly fair-skinned .
Recently, a national study of all adults in Denmark found that the risk of dementia, particularly Alzheimer disease, was increased for adults with rosacea who were >60 years of age . A causal relationship has not been claimed and the results need to be confirmed by additional studies.
Pathogenesis
In rosacea, several different but interrelated pathomechanisms have been proposed ( Fig. 37.1 ), with predominant pathways reflecting clinical features. Both environmental triggers and genetic predisposition play a role, with up to 20% of patients in some studies reporting a family history of rosacea. Two of the major abnormalities are neurovascular dysregulation and an aberrant innate immune response , both of which can lead to cutaneous inflammation.
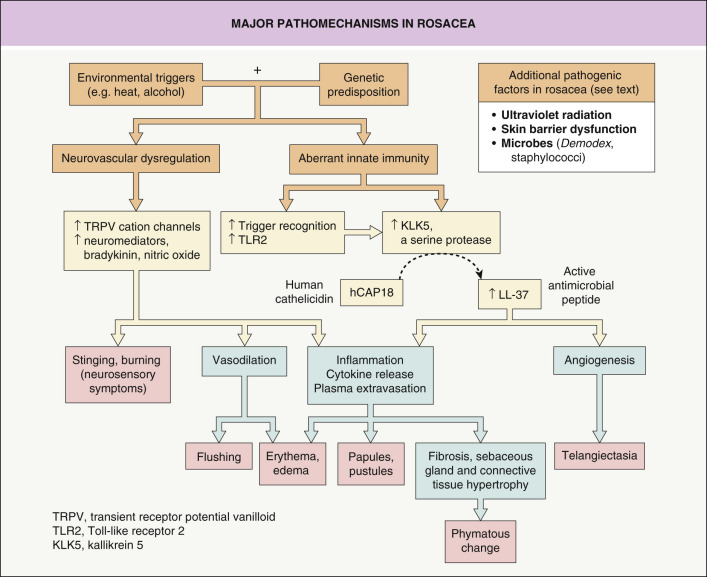
Several clinical features of rosacea, including transient erythema, persistent centrofacial erythema, telangiectasias and flushing, point to the important role the vascular system plays in its pathogenesis. An increase in blood flow within skin lesions of rosacea has been demonstrated , and patients with rosacea flush more readily in response to heat. Histopathologic studies of lesional skin found an elevated expression of vascular endothelial growth factor (VEGF), CD31, and the lymphatic endothelial marker D2-40 (podoplanin), implying increased stimulation of vascular and lymphatic endothelial cells .
In patients with rosacea, including ETTR, sensations of stinging or burning of the skin are commonly reported and affected individuals also exhibit lower heat pain thresholds, as compared to controls . Stimulation of cutaneous nerve endings expressing transient receptor potential vanilloid (TRPV) cation channels by trigger factors (e.g. spicy food, heat, alcohol) can lead to dysesthesia, flushing, and erythema . Heightened TRPV activity within the skin of patients with rosacea is associated with neurogenic inflammation, an inflammatory response induced by sensory nerves in which neuromediators are released at the site of inflammation. The latter can result in vasodilation, plasma extravasation of proteins, and recruitment of inflammatory cells (see Fig. 37.1 ).
Evidence that an aberrant innate immune response also plays a role in the pathogenesis of rosacea includes upregulation of LL-37 via enhanced processing of cathelicidin by the trypsin-like serine protease kallikrein 5 . When injected into mouse skin, cathelicidin peptides induced proinflammatory and angiogenic activity, leading to the proposal that dysfunction of the innate immune system could unify many of the clinical features of rosacea, especially the inflammatory lesions (see Fig. 37.1 ) . In histopathologic studies of PPR, inflammatory changes were noted to be most pronounced near the bulge region of the pilosebaceous follicle , the site of stem cells whose expression profile overlaps with that of the innate immune system.
Based upon a higher prevalence in those with skin phototypes I and II (see above), ultraviolet light has been proposed as an additional contributing factor to the pathogenesis of rosacea. Exposure to UVB can induce angiogenesis and it increases the secretion of angiogenic factors (e.g. VEGF) from keratinocytes . UVR also induces production of reactive oxygen species, which upregulate matrix metalloproteinases that lead to vascular and dermal matrix damage . Although clinically ETTR can resemble telangiectatic photoaging, a case–control observational study provided evidence that they are distinct entities ; as expected, some patients have both disorders. In contrast, PPR does not appear to be significantly related to cutaneous photodamage or UV exposure .
Several clinical features of rosacea imply skin barrier dysfunction . Rosacea patients often report facial dryness, and studies have confirmed a lowered threshold for skin irritancy . Both ETTR and PPR patients have increased transepidermal water loss, a marker of epidermal barrier dysfunction, and it has been suggested that disruption or abnormality of the stratum corneum allows penetration of sensory irritants . In addition, patients with PPR have an abnormal skin surface fatty acid profile as well as reduced epidermal hydration levels; the latter were noted to improve following treatment with minocycline and resolution of inflammatory lesions .
Demodex mites ( folliculorum and brevis ) are normally present on the face as commensal microbes, but in rosacea, greater numbers of these mites are detected by skin surface biopsy techniques . In routine histologic sections, the mites often appear prominently within pilosebaceous follicles and follicular infestation with multiple mites can be associated with an intense perifollicular infiltrate of predominantly CD4 T helper cells . Antigenic proteins from a bacterium ( Bacillus oleronius ) isolated from Demodex mites can stimulate inflammation in patients with PPR . It has been suggested that Demodex mites and their associated bacteria upregulate local proteases, thereby potentiating dysregulation of the cutaneous innate immune response (see above) .
Lastly, it seems unlikely, based upon current evidence, that Helicobacter pylori infection plays an etiologic role in the pathogenesis of rosacea .
Clinical Features
Rosacea usually has its onset during middle age, with women often affected at a younger age than men. While rosacea is not commonly observed in children , the rosacea-like conditions periorificial dermatitis and steroid-induced rosacea are fairly common.
From a clinical perspective it is useful to classify rosacea into the following four subtypes ( Table 37.1 ) . However, this classification is intended as a guide given that there is some overlap amongst the subtypes and a patient can have more than one subtype.
- •
Erythematotelangiectatic rosacea (subtype 1; ETTR): Individuals have a tendency to flush combined with a background of persistent facial erythema ( Fig. 37.2 ) and sometimes telangiectasias. These patients typically have skin phototypes I or II and it may be difficult to differentiate ETTR from telangiectatic photoaging, but there are some relative differences (see Table 37.3 ) . In addition, when patients complain of significant flushing other causes of flushing should be considered as outlined in Tables 106.2 & 106.3 .

Fig. 37.2
Erythematotelangiectatic rosacea.
Persistent erythema of the medial and lateral cheeks is seen. In this patient, there are no telangiectasias, indicating mild (grade 1) disease.
- •
Papulopustular rosacea (subtype 2; PPR): Patients have a centrofacial eruption of multiple, small (<3 mm), dome-shaped, erythematous papules that appear singly or in crops ( Figs 37.3 & 37.4 ). A minority of these inflammatory lesions have a central pustule. Characteristically, the papules and pustules are in varying stages of evolution. Although the patient may complain of mild discomfort or pruritus and the lesions may be slightly tender, the social distress caused by the appearance of the eruption often far exceeds the physical symptoms. Individual papules or pustules last about two weeks and are then replaced by blotchy postinflammatory erythema which gradually fades over ~10 days. Residual scarring is not a feature of PPR.

Fig. 37.3
Moderate papulopustular rosacea of the forehead.
Note the superficial nature of the inflammatory lesions.

Fig. 37.4
Moderate to severe papulopustular rosacea.
There is a typical centrofacial distribution of erythema, telangiectasias, papules and pustules. In addition, the skin has a scaly, crusty surface and this is often a sign of more severe disease.
A halo of erythema may surround larger inflammatory lesions and tiny telangiectatic vessels may be visible within this rim. Occasionally, when there is more severe disease, scaling or superficial crusting may be seen and this has been referred to as “rosacea dermatitis” ( Fig. 37.5 ). Lastly, some patients will have some degree of persistent erythema of the cheeks that may represent a combination of postinflammatory erythema, telangiectasias, and vasodilation.

Fig. 37.5
Rosacea dermatitis.
When there is more severe disease, scaling and superficial crusting may be seen as on the cheek of this woman.
Courtesy, Kalman Watsky, MD.
- •
Phymatous rosacea (subtype 3): In this form of rosacea, sebaceous gland hypertrophy is accompanied by fibrosis. Rhinophyma is by far the most common clinical presentation, occurring primarily in men ( Fig. 37.6 ). Involvement of other anatomic sites has been reported, but it is rare ( Table 37.2 ). Patients with rhinophyma may have other features of rosacea, usually mild to moderately severe PPR. However, phymatous rosacea may arise de novo without any preceding skin changes and therefore should not be viewed as “end-stage rosacea” . The earliest clinical sign of rhinophyma is the appearance of patulous follicles (“dilated pores”) on the distal portions of the nose. It has been suggested that telangiectatic vessels in this same location may predispose to hypertrophic changes ( Fig. 37.7 ). In severe cases of rhinophyma, the tissue hypertrophy leads to nasal distortion, with soft fleshy nodular growths resulting in significant disfigurement. Although basal cell carcinomas have been reported to arise in skin affected by rhinophyma, there is insufficient evidence to suggest that this condition predisposes to malignant change.

Fig. 37.6
Rhinophyma.
Hypertrophy of sebaceous glands and connective tissue as well as patulous follicles are seen. The changes are more prominent in the mid to lower nose. In addition, there is evidence of papulopustular rosacea.
Courtesy, Kalman Watsky, MD.
Table 37.2
Types of phymatous rosacea.
TYPES OF PHYMATOUS ROSACEA
Phyma
Clinical features
Rhinophyma
- •
Apparent initially as dilated patulous follicles at the distal end of the nose
- •
When marked, can lead to debilitating nasal deformity
Gnathophyma
- •
Rare occurrence, with central chin typically involved
- •
May give rise to asymmetrical swelling
Otophyma
- •
Usually affects the lower half of the helices and lobes of the ears
Metophyma
- •
Cushion-like, firm swelling of central forehead
Blepharophyma
- •
Swelling of the eyelids
- •
Usually seen as a component of edematous rosacea but may accompany severe papulopustular or ocular rosacea

Fig. 37.7
Tortuous, telangiectatic vessels on the distal aspect of the nose contribute to its hyperemic appearance.
This hyperemia may predispose to the subsequent hypertrophic changes of rhinophyma. Note the early sign of patulous follicles (“dilated pores”).
The edematous changes sometimes seen in patients with severe inflammatory rosacea ( Fig. 37.8 ) should not be confused with phymatous rosacea. Such changes, unlike those of phymatous rosacea, often improve following successful management of the inflammatory lesions; however, some degree of lymphedema may persist.

Fig. 37.8
Inflammatory rosacea with edematous changes.
An intensely erythematous plaque is present on the medial aspect of the cheek. This may improve once the underlying inflammation is treated appropriately.
- •
- •
Ocular rosacea (subtype 4): This entity may or may not be accompanied by cutaneous changes of rosacea. Without cutaneous manifestations, the diagnosis of ocular rosacea can be difficult to establish with certainty. Patients with ETTR and PPR appear to be particularly vulnerable to the development of ocular inflammation, with up to 50% affected ( Fig. 37.9 ). Symptoms are nonspecific and include dryness, a gritty sensation, an inability to wear contact lenses, tearing, crusting of the eyelid margins, frequent styes (hordeola), and sometimes pruritus. Patients usually do not associate these ocular symptoms with their rosacea and may not volunteer such information unless specifically asked. The clinical signs of ocular rosacea are diverse – there may be tiny concretions at the bases of the cilia (conical dandruff; see Fig. 37.9A ) or mild scaling of the eyelid margins. When the disease is more active, there is evidence of blepharitis, often with eyelid swelling and conjunctival injection; the overall appearance is that of a “red eye” (see Fig. 37.9C ). Cysts arising from the meibomian glands (chalazia) present as firm nontender swellings of the cutaneous tarsal surface, while hordeola are similar but are tender and often painful swellings. Patients often refer to a hordeolum as a “stye”. Severe ocular disease (e.g. keratitis, corneal neovascularization, uveitis, scleritis, iritis) is rarely seen in patients with rosacea.
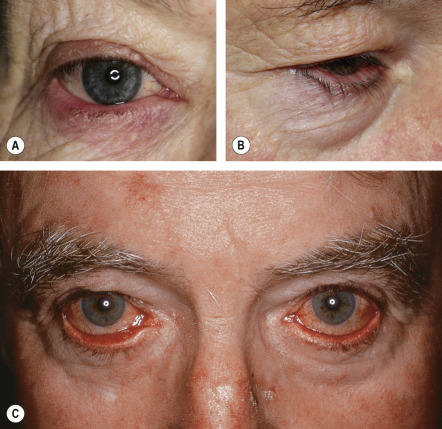
Fig. 37.9
Ocular rosacea.
A Tiny concretions of keratin (conical dandruff) are visible at the bases of some of the eyelashes of the lower eyelid. There is also evidence of blepharitis of the lower eyelid and conjunctival injection. B Erythema of the mucosal portion of the lower eyelid and ectropion. C Marked injection of the conjunctivae, leading to the appearance of red eyes. Ectropion is also present.
| CLASSIFICATION, CLINICAL FEATURES AND MANAGEMENT OF SUBTYPES OF ROSACEA | ||||
|---|---|---|---|---|
| Subtype | Predominant clinical features | Severity | Management | |
| Grade | Features | |||
| Erythematotelangiectatic (ETTR) |
| 1 | Occasional mild flushing; faint persistent centrofacial erythema; few telangiectasias |
|
| 2 | Frequent troublesome flushing; moderate persistent centrofacial erythema; several distinct telangiectasias | |||
| 3 | Frequent severe flushing; pronounced persistent centrofacial erythema; many prominent telangiectasias; possible edema | |||
| Papulopustular (PPR) |
| 1 | Few papules and/or papulopustules; mild persistent centrofacial erythema |
|
| 2 | Several papules and/or papulopustules; moderate persistent centrofacial erythema | |||
| 3 | Extensive papules and/or papulopustules; pronounced persistent centrofacial erythema; inflammatory plaques or edema may be present | |||
| Phymatous |
| 1 | Puffiness; mildly patulous follicles; no clinically apparent hypertrophy of connective tissue or sebaceous glands; no change in contour |
|
| 2 | Moderate swelling; moderately dilated patulous follicles; clinically, mild hypertrophy of the sebaceous glands or connective tissue; change in nasal contour without nodular component | |||
| 3 | Marked swelling; large dilated follicles; distortion of contour due to hypertrophy of the sebaceous glands and/or connective tissue, with a nodular component | |||
| Ocular |
| 1 | Mild itch, dryness or grittiness; fine scaling of eyelid margins; telangiectasia of eyelid margins; mild conjunctival injection |
|
| 2 | Burning or stinging; crusting, irregularity, erythema and/or edema of eyelid margins; definite conjunctival injection; chalazion or hordeolum | |||
| 3 | Pain, photosensitivity, blurred vision; severe eyelid changes with loss of lashes, severe conjunctival inflammation; corneal changes, with potential loss of vision; episcleritis, scleritis; iritis | |||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


