Pierre Robin sequence is defined by the clinical triad: mandibular hypoplasia, glossoptosis, and airway obstruction. Mandibular distraction osteogenesis (MDO) is a standard treatment of Robin sequence associated with severe airway obstruction and is the only intervention that directly corrects the underlying anatomic pathologic condition. Compared with tongue-lip adhesion, MDO has demonstrated more success in treating airway obstruction in infants with Pierre Robin sequence, including patients with syndromic diagnoses and concomitant anomalies. This article provides a current, comprehensive review of neonatal mandibular distraction and offers treatment guidelines based on a combined surgical experience of more than 400 patients.
Key points
- •
In properly selected patients, neonatal mandibular distraction osteogenesis can resolve tongue-based airway obstruction and obviate tracheostomy in Pierre Robin sequence patients with severe airway obstruction.
- •
Understanding mandibular morphology in Robin sequence is crucial to plan and to properly place osteotomies and vectors.
- •
The complication rate associated with neonatal mandibular distraction is low in both occurrence and level of acuity.
- •
Specific indications for neonatal mandibular distraction have not been codified, but it is a critical next step toward the standardization of care.
Introduction
Pierre Robin sequence is defined by the clinical triad: mandibular hypoplasia, glossoptosis, and airway obstruction. In his 1923 publication, Robin first described the eponymous constellation of respiratory distress associated with glossoptosis in the presence of mandibular micrognathia. , Cleft palate is not a criterion for the diagnosis of Robin sequence despite the fact that up to 90% of affected patients have a concomitant U-shaped or V-shaped cleft of the posterior palate. With Robin sequence, nosologic confusion is evidenced by the wide variability in defining the clinical entity, which is highlighted in a survey of American Cleft Palate-Craniofacial Association providers. Inaccurate use of the correct Robin sequence definition hinders communication between specialists and thwarts the development of standardized care protocols.
A multidisciplinary approach to Robin sequence evaluation and treatment is critical and includes neonatologists, geneticists, pulmonologists, developmental pediatricians, otolaryngologists, plastic surgeons, pediatric gastroenterologists, nurse feeding specialists, and speech-language pathologists. Although there are multiple conservative interventions available for infants expressing mild to moderate airway obstruction, this article addresses the implementation of mandibular distraction in severely affected infants and neonates. Direct laryngoscopy/bronchoscopy, and polysomnography (PSG) should be performed, whenever possible, for patients under consideration for surgical intervention.
Although drug-induced sleep endoscopy (DISE) from nasal aperture to bronchus is the yardstick to assess glossoptosis and other associated airway anomalies, the degree of glossoptosis may not correlate with the severity of respiratory dysfunction.
PSG remains the gold standard to quantify the severity of airway obstruction and to identify the presence of central sleep apnea. However, PSG interpretation is not standardized for neonates. , A severe obstructive index in neonates has been reported from greater than 6 to greater than 24, thereby representing a wide range of interpretation in the literature. Most craniofacial surgeons select an apnea-hypopnea index (AHI) of 11 to 29 as their minimum for surgical intervention. Thus, PSG indications for neonatal mandibular distraction osteogenesis (MDO) for Robin sequence are currently based largely on clinical judgment. Establishment of reference values for neonates will provide a helpful construct to further standardize polysomnographic findings in the complex Robin sequence population. The senior authors’ protocol of care includes PSG on all neonates under consideration for MDO unless the patient is intubated or PSG is not tolerated/possible. A maxillofacial computed tomography (CT) scan is obtained to evaluate the quality of the bone stock as well as mandibular and temporomandibular joint (TMJ) morphology. Concomitantly, under the same anesthetic before MDO, a pediatric otolaryngologist performs a DISE. Neonates with Robin sequence may also have secondary airway abnormalities that compound respiratory distress, such as laryngomalacia, bronchial stenosis, bronchomalacia, or tracheomalacia, , which may influence the decision to proceed with MDO.
Previously, laryngomalacia was deemed a contraindication to successful distraction in Robin sequence patients. However, Tholpady and colleagues demonstrated that properly selected patients with Robin sequence and laryngomalacia can successfully undergo MDO and avoid tracheostomy. It is important to note that close collaboration with an experienced pediatric otolaryngologist is critical to proper patient indications, and certain patients will require supraglottoplasty before, concurrent with, or after MDO.
Surgical management
Robin sequence patients with severe airway obstruction, who fail nonsurgical management, are considered for surgical intervention, including tracheostomy, tongue-lip adhesion (TLA), MDO, or subperiosteal release of the floor of mouth. Tracheostomy is a direct, effective method to establish the airway, which relies on subsequent mandibular growth to facilitate decannulation. As tracheostomy is associated with multiple morbidities, including laryngeal stenosis, tracheomalacia, chronic pneumonia, and extensive nursing care, it is usually reserved for patients in which no other intervention is deemed to be a viable option. More recently, tracheostomy has been shown to be associated with increased financial costs compared with MDO. Despite these limitations, tracheostomy is still a life-saving intervention, especially for medically complex patients with multiple sites of airway obstruction. , ,
TLA is a staged surgical technique that translates the base of the tongue anteriorly until airway obstruction is definitively alleviated by lower jaw growth. Although there is supportive evidence that TLA can relieve airway obstruction caused by Robin sequence, most comprehensive analyses demonstrate that clinical outcomes are inferior to mandibular distraction. , The success of TLA is predicated upon compensatory “catch-up” growth of the mandible to relieve airway obstruction, which remains a debated concept. ,
Clinically introduced and popularized by McCarthy and colleagues, MDO is a safe and effective intervention for relieving airway obstruction in infants with severe Robin sequence. , , , , Its use, even in neonates weighing less than 4 kg with severe airway obstruction, slowly became more popular after the first publications of Collares and colleagues (2000), Denny and colleagues (2002), and Monasterio and colleagues (2002). The benefit of neonatal distraction lies in direct anterior translation of the mandible and tongue base, thus increasing airway patency as glossoptosis is decreased. Current indications for MDO include PSG demonstrating no or limited central sleep apnea and either an AHI greater than 20 (New York University [NYU])/greater than 6 (Hospital de Clinicas de Porto Alegre [HCPA]), or Sa o 2 less than 90% more than 1% of sleep time (HCPA), or significant carbon dioxide retention, and absence of severe neurologic or cardiac pathologic condition or secondary airway pathologic condition, which could preclude successful restoration of the airway. Because MDO can be effective for correction of tongue-based airway obstruction and tracheostomy avoidance, it has become the first-line surgical option for Robin sequence patients at many institutions. , , , , ,
MDO has been found to be a superior intervention to relieve tongue-based airway obstruction compared with TLA by multiple studies. In nonsyndromic patients, MDO results in shorter time to extubation, a higher postoperative oxygen saturation level, a greater decrease in AHI, and a lower incidence of tracheostomy when compared with TLA. In a subsequent comparative study that included both Robin sequence syndromic diagnoses and significant medical comorbidities, superior airway outcomes were demonstrated using MDO compared with TLA despite a 5-fold increase in syndromic diagnosis and large increase in central nervous system anomalies in the MDO cohort. These data points have been corroborated by other institutional studies and meta-analyses. , , ,
Surgical considerations in mandibular distraction
As most Robin sequence cases have primary hypoplasia of the mandibular body, a horizontal vector is commonly used. In contrast, several other institutions do use a vertical vector for the mandibular distraction. , Duarte and Collares, comparing pre-MDO and post-MDO, showed horizontal vectors resulted in an increase of 11% for ramus, and 36% in body length, whereas the vertical vectors showed an elongation of 34% in ramus and 27.5% in body length. Vertical vectors were used in 30% of their series with no TMJ damage. They stated vertical vectors should be carefully considered when the ramus is impaired. Ultimately, substantial airway enlargement occurs after mandibular distraction, and no difference in final airway volumes has been demonstrated between the use of horizontal or vertical vectors. However, prudent judgment should be exercised when committing to the vertical vector in the Robin sequence patient population, as it risks iatrogenic damage to theTMJ. This iatrogenic injury can result either directly by placement of the device and screws too close to the condyle or indirectly by forcing the vector of distraction into the glenoid fossa. TMJ ankylosis in the infant is a morbid complication reported in a small percentage of cases and can be a challenging sequela to treat. , However, iatrogenic TMJ ankylosis can be avoided by using a horizontal vector. , , ,
Considerations for Osteotomy Technique
Among craniofacial surgeons performing MDO, 39% of surgeons perform an inverted L ramus osteotomy, 37% perform a mandibular angle osteotomy, 17% perform a mandibular body osteotomy, and the remainder perform a horizontal ramus osteotomy. Although the inverted L-osteotomy requires the most dissection and the other osteotomies are simpler to perform, the inverted L-osteotomy and the horizontal ramus osteotomy design provide the best opportunity to preserve developing tooth buds and lower-lip sensibility. Although piezoelectric saws can theoretically accomplish this as well, clinical outcomes in the neonatal population are pending.
Surgical Techniques
MDO can be performed with external or internal devices. The choice between techniques is dependent on the volume of mandibular bone as well as the desired vector of distraction, and the surgeon/institutional surgical preference is based on experience. Despite the differences in the techniques, there are certain shared surgical principles.
Surgical exposure
Mandibular distraction is performed through an extraoral approach for direct exposure to the mandible without the risk of oral contamination. A transoral approach is certainly a viable option; however, precision in vector and screw placement can be compromised by this approach. A Risdon incision is placed 1 cm inferior to the mandibular border. Sharp dissection is performed to and through the platysma, and a small superior and inferior platysma flap is mobilized to facilitate layered closure at the end of the procedure. Wide subperiosteal exposure of the ramus, angle, distal body, and sigmoid notch is obtained. The condyle is not dissected.
Corticotomy/osteotomy
A subtotal osteotomy (corticotomy) is performed before placement of the device. This subtotal osteotomy will preserve native mandibular form and position, facilitating accurate device positioning. After the device is secured, the osteotomy is completed. The bony edges are then broadly separated, and any remaining bony bridges are separated. This separation will avoid “premature consolidation” of the bony edges, which is more likely an incomplete osteotomy.
Internal Devices: Mandibular Distraction Osteogenesis: New York University Technique
Internal devices are more easily tolerated by infants, but require repeat surgery for removal. Most craniofacial surgeons use internal devices (79.9%), and there are a variety of osteotomy techniques, distraction devices, and surgical approaches. The senior author’s (R.L.F.) preferred technique is described in detail with an accompanying surgical video in the reference by Diep and colleagues. This reference delineates and the surgical video demonstrates the preferred patient markings, extraoral approach, inverted L-osteotomy, and semiburied distraction device used by the senior author (R.L.F.).
Osteotomy
A coronoidectomy is performed with a sagittal saw or 2-mm Kerrison punch. A near-complete vertical ramus osteotomy is then performed from the sigmoid notch to the antegonial notch. A full corticotomy is made over the buccal face of the mandible and along the superior and inferior aspects of the lingual surface of the mandible, leaving a small lingual bony bridge along the horizontal axis of the jaw. The purpose of the near-complete osteotomy is to maintain alignment of the mandible during placement of the distractor devices. Importantly, the vertical ramus osteotomy avoids injury to the inferior alveolar nerve and the developing tooth buds. Alternatively, one can consider using an ultrasonic bone cutter to make the described inverted L-osteotomy or a mandibular body osteotomy. , ,
Hardware application
A 20-mm semiburied, uniplane distraction device (Micro Zurich mandibular distractor; KLS Martin, Jacksonville, FL, USA) with a ratchet is primarily used. In cases of extreme micrognathia, longer devices are occasionally used. The ratchet system on the device is protective, as it prevents backing of the activation by parental error or inadvertent manipulation by the infant. The device is affixed to the lower border of the mandible, and the activation arm exits percutaneously behind the earlobe. To affix the footplates to the mandible, high-profile screws are used, as they are easy to apply and more easily removed compared with 1-mm screws. When using a ratchet system distractor, high-profile screws can impinge on the ratchet during full activation; thus, the placement and type of screws should be carefully considered by the craniofacial surgeon. , ,
Once the device is secured to the mandible, the distractor is activated for several millimeters, and there should be no resistance on the device once activated. The osteotomy on the lingual surface may be completed by activation of the device alone. Completion of the mandibular osteotomy should be confirmed by palpation using an osteotome or a suction cannula, as direct vision will not suffice for confirming that the osteotomy is complete. Once a full osteotomy is confirmed, the bony edges are opposed, and the initial Risdon incision is closed meticulously in layers. , ,
Distraction and postoperative management
After a latency period of 5 days, activation is commenced at a rate of 1 mm per day to the maximal permissible length of the distraction device, or until the deemed appropriate maxillomandibular distraction is achieved. In the interim, serial cephalograms are obtained to closely monitor the distraction progress, to confirm symmetric bilateral advancement, and to identify any device failures. Last, the devices are removed in a second operation after 6 weeks of consolidation. , ,
Following completion of mandibular distraction, the patient should be followed by a plastic surgeon and a pediatric otolaryngologist or pulmonologist to monitor mandibular development and the recurrence of obstructive breathing patterns. In addition, a follow-up PSG is obtained within 3 months of distractor removal. ,
External Devices: Mandibular Distraction Osteogenesis: Porto Alegre Technique
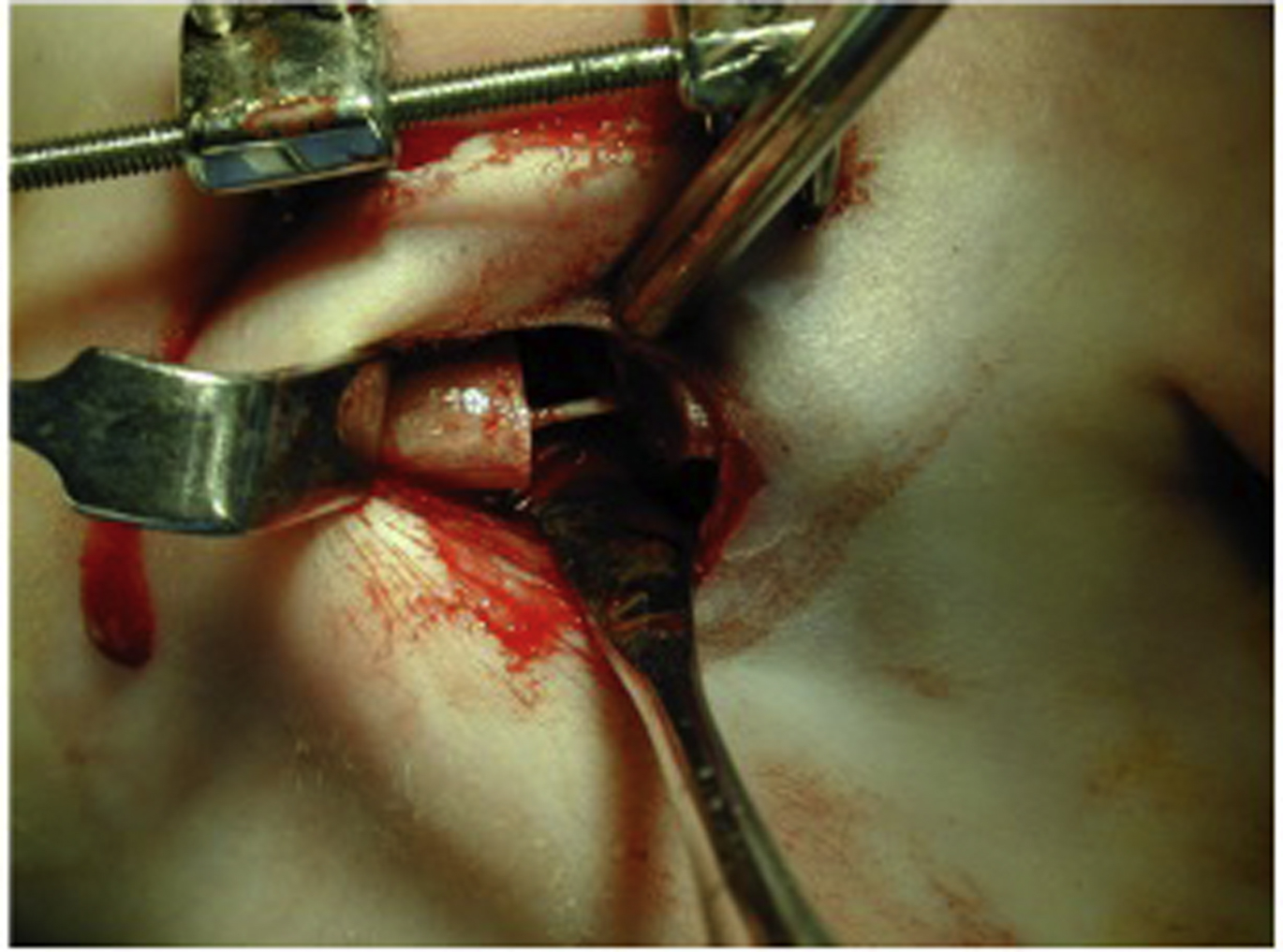
External devices are easy to adjust and remove, facilitate shorter surgeries, and have the capability of remodeling and adjusting the vector mid-distraction. The preferred surgical technique by the senior author is demonstrated. They also have the versatility to be reused as devices, and the overall treatment costs tend to be lower, which is of particular interest in developing countries. External devices are well tolerated by neonates ( Fig. 1 ).

The main disadvantage of external devices is poor scarring, although it is mostly inconspicuous in neonates. In reviewing clinical outcomes of MDO, it is key to interpret findings judiciously, as analyses of internal device outcomes may not be extrapolated to external devices.
Osteotomy
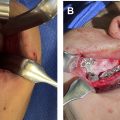
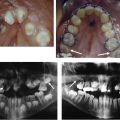
A near-complete osteotomy is then performed with a thin reciprocating saw. A full corticotomy is made over the retromolar area and the posterior/inferior border of the mandible, leaving a lingual bony bridge to keep the segments aligned for pin placement along the chosen vector. An inverted L on the ramus/angle is preferred over a vertical/oblique osteotomy, on the distal body/angle, to protect the inferior alveolar nerve and the developing tooth buds ( Fig. 2 ). In 30% of the authors’ cases, they use a horizontal osteotomy on the ramus, for vertical vectors, which also keeps the nerve and tooth buds safe ( Fig. 3 ). The horizontal/oblique vectors range from 10° to −20°, and vertical vectors have an inclination of 80° to 120° both related to the mandibular plane.