Anatomic studies have identified that patients with Treacher Collins syndrome and some cases of bilateral craniofacial microsomia are characterized by multilevel airway obstruction as a result of hypoplasia and clockwise rotation of the maxillomandibular complex. Patients often remain tracheostomy-dependent despite multiple airway surgeries. Counterclockwise craniofacial distraction osteogenesis aims to correct the facial skeletal deformity and expand the upper airway volume by rotating the subcranial complex en bloc around the nasofrontal junction. Early results have demonstrated significant increases in the nasopharyngeal and oropharyngeal airway volumes with successful decannulation in a majority of patients who have undergone this operation.
Key points
- •
The skeletal deformity of Treacher Collins syndrome and some cases of bilateral craniofacial microsomia are characterized by a high occlusal plane in addition to mandibular and midface hypoplasia.
- •
This bimaxillary rotational deformity results in upper airway narrowing of the oropharynx and nasopharynx and can result in tracheostomy dependence.
- •
Counterclockwise craniofacial distraction osteogenesis (C3DO) increases the airway volume at both the nasopharyngeal and oropharyngeal levels through rotation of the entire subcranial skeleton.
- •
In cases without an adequate condylar to skull base relationship, such as in Pruzansky types IIB and III mandibular deformities, a staged approach with enucleation of the second molar follicles and temporomandibular joint reconstruction with costochondral graft is required before C3DO.
- •
C3DO can result in successful decannulation of tracheostomy-dependent patients with a rotational deformity, when previous attempts of single jaw surgery or choanal atresia surgery have been unsuccessful.
Background
Treacher Collins syndrome is an autosomal dominant condition characterized by abnormal development of craniofacial structures derived from the first and second branchial arches. Clinical features can include hypoplastic zygomas, micrognathia, microtia, conductive hearing loss, coloboma of the eyelids, down-slanting palpebral fissures, and cleft palate. Severe presentation is characterized by hypoplasia and clockwise rotation of the maxillomandibular complex, contributing to upper airway obstruction and tracheostomy dependence. , The prevalence of obstructive sleep apnea in Treacher Collins syndrome patients has been reported to range from 25% to 91%, with a significant subset requiring tracheostomy. In the most severe cases, patients remain tracheostomy-dependent despite multiple surgical interventions, including isolated lengthening of mandible through distraction osteogenesis.
Three-dimensional airway analysis of Treacher Collins syndrome has revealed reduced airway volume at multiple levels, including the nasal and retroglossal region. Furthermore, the degree of maxillomandibular hypoplasia and clockwise rotation both contribute to the reduced airway volume. , The importance of counterclockwise rotation to treat obstructive airway disease is well recognized. , Tessier proposed the integral procedure in 1985 to correct the rotational deformity in Treacher Collins syndrome using a combination of Le Fort II and mandibular osteotomies. This operation was limited, however, by the need for extensive bone grafting, high rates of relapse, and challenge with overcoming the restrictive soft tissue envelope.
The counterclockwise craniofacial distraction osteogenesis (C3DO) shares some similarities to the integral procedure described by Tessier but leverages the gradual stretching of the surrounding soft tissue envelope characterized by distraction osteogenesis. C3DO combines subcranial and bilateral mandibular distraction around a nasofrontal pivot point to achieve counterclockwise rotation of the maxillomandibular complex and expansion of the entire upper airway. The goal of the operation is to achieve decannulation in tracheostomy-dependent children. Early results of this operation in tracheostomy-dependent children with Treacher Collins syndrome have demonstrated a large magnitude of palatal rotation and a high success rate of decannulation.
Indications
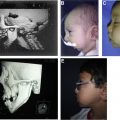
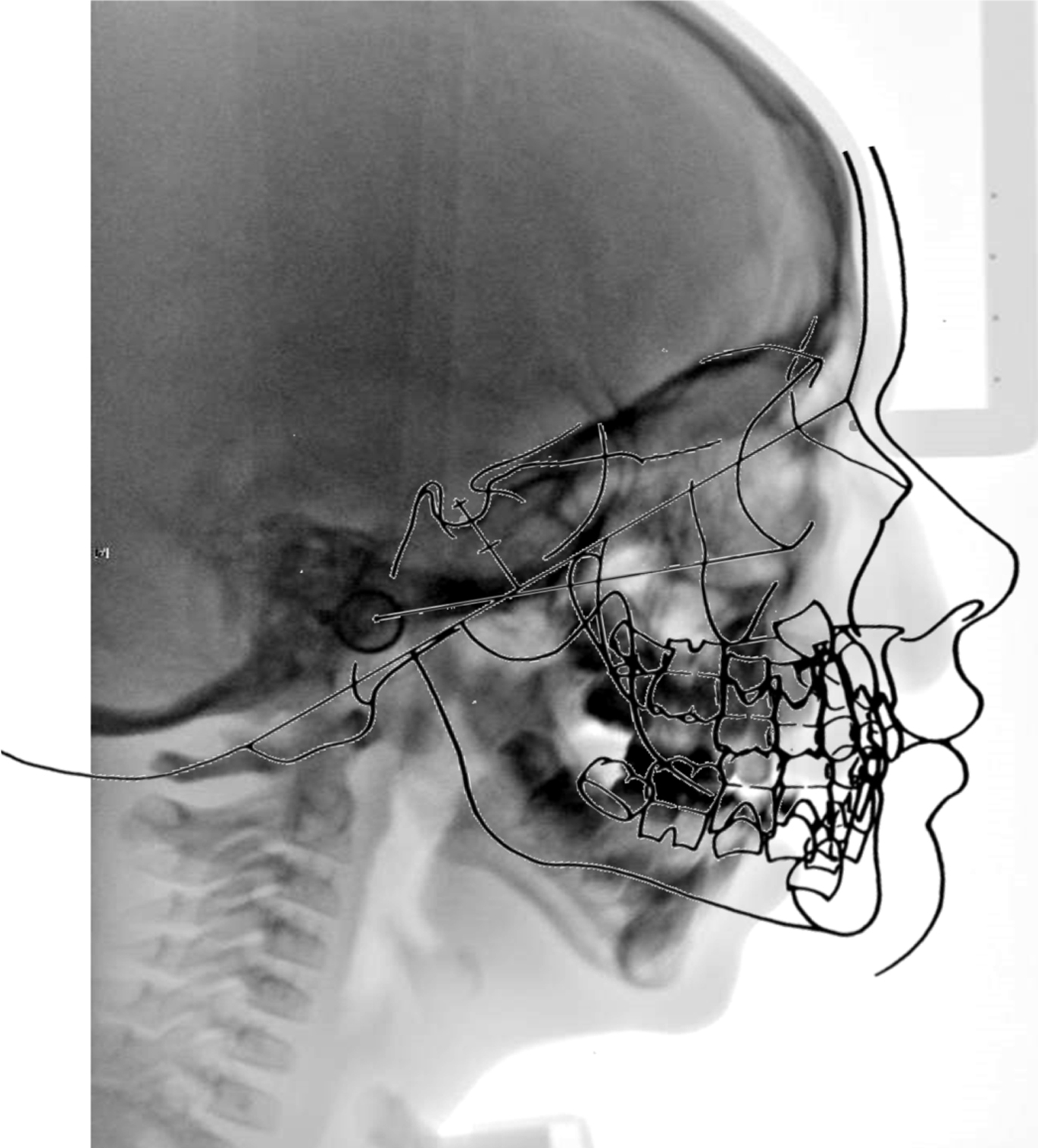
The primary indication for C3DO is severe airway obstruction with tracheostomy dependence in the setting of maxillomandibular deficiency and a high occlusal plane ( Fig. 1 ). Many patients who undergo this operation have had unsuccessful attempts to remove the tracheostomy tube using other procedures, including isolated mandibular distraction, and often are dependent on gastrostomy tube for feeding. In addition to Treacher Collins syndrome, severe presentations of other conditions, such as craniofacial microsomia and acrofacial dysostosis, also have benefited from this operation.
All patients require computed tomography (CT) imaging to assess the bony and soft tissue anatomy and undergo a formal airway evaluation by a pediatric otolaryngologist to characterize the airway anatomy and levels of obstruction. A combination of restricted nasopharyngeal volume, small choana, oropharyngeal obstruction from retroglossia, and a high palatal plane indicates the patient would benefit from rotational advancement of the maxillomandibular complex. CT-based virtual surgical planning (VSP) is used to plan the osteotomy and traction pin placements, and a craniofacial orthodontist fabricates an occlusal splint with traction posts to coordinate final jaw positioning. At the authors’ center, the C3DO operation is not performed before the age of 7, and the surgery preferably is performed closer to the age of 10. This timing optimizes bone stability, allows eruption of permanent molars and central incisors for splint stability, and from the authors’ experience provides airway improvement that lasts until the final orthognathic treatment at maturity.
A staged approach is required in patients with abnormal temporomandibular joints, such as Kaban-Pruzansky type IIB and type III mandibles. The first stage is enucleation of second molar follicles that is in the line of the eventual mandible osteotomy, along with iliac crest corticocancellous grafting to augment the posterior mandible and facilitate enucleation site healing. The second stage takes place approximately 9 months later to place bilateral costochondral grafts to establish a centric relation. The subcranial rotational surgery then is planned as a third stage approximately 9 months to 12 months after the second stage. Depending on the patient’s mandibular anatomy, the first 2 stages may be combined if there is adequate bone stock for fixation of the costochondral graft and planning of the final mandible osteotomy.
Surgical technique
Stage 1: Enucleation of Mandible Second Molar Follicles and Iliac Crest Bone Grafting
- •
Enucleation of tooth follicles is performed through an external approach using the Risdon incisions that are used for subsequent stages.
- •
Subperiosteal dissection then is performed along the inferior border of the mandibular body and up to the apex of the mandibular ramus remnant.
- •
A piezoelectric saw is used to create a bony window over the dental follicle to allow enucleation.
- •
The extraction site is burred to create a recipient bed for bone grafting, with care taken to avoid damage to the inferior alveolar nerve that typically is in close proximity.
- •
Both cancellous bone graft and a piece of medial cortical bone are harvested from the iliac crest.
- •
The cancellous bone graft is used to pack the extraction site, and the cortical graft is used to augment the posterior mandible and secured with a lag screw.
- •
All incisions are closed, and the extraction site is allowed to heal for approximately 9 months before the next stage.
Stage 2: Temporomandibular Joint Reconstruction with Costochondral Graft
- •
The authors use VSP and stereotactic navigation guidance to ensure accurate placement of costochondral grafts relative to the skull base.
- •
The Risdon incisions are reopened to expose the inferior border of the hypoplastic mandible.
- •
VSP cutting guides are used to shave off the prominence of the mandibular angle to allow for better apposition of the costochondral grafts to the mandible.
- •
VSP positioning guides are used to identify the desired angle of graft placement, and blunt finger dissection is used to create a pocket toward the skull base just lateral to the pterygoid plates.
- •
Stereotactic navigation then is used within the pocket to confirm the landing point of the graft on the skull base.
- •
A third or fourth costochondral graft is harvested with a length determined by VSP planning and 5 mm of cartilage cap with intact perichondrium.
- •
The VSP occlusal splint is used to establish the desired maxillomandibular relationship. Minor closure of an anterior open bite is possible if there is sufficient mandible mobility.
- •
Positioning guides are used to insert the rib graft in the appropriate orientation ( Fig. 2 ), and stereotactic navigation can be used again to confirm the placement of the graft.
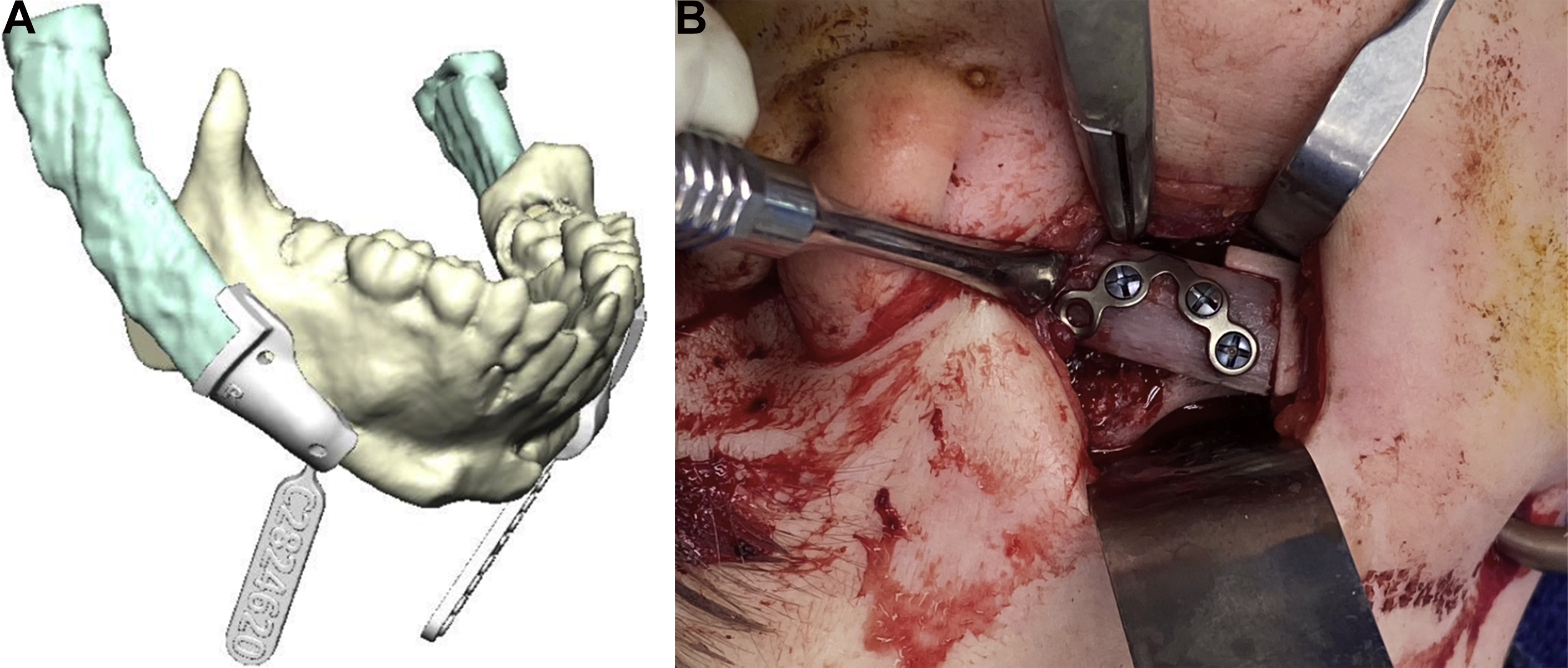
Fig. 2
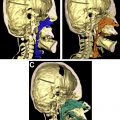
( A ) VSP for accurate positioning of costochondral grafts in a patient with severe mandibular hypoplasia. ( B ) Positioning of the graft with the use of the custom guide through a Risdon incision. Establishment of a temporomandibular relationship with costochondral grafts is performed in selected patients 9 months to 12 months before the C3DO procedure.
- •
Once the location has been confirmed, the rib graft is fixated with titanium plates and screws.
- •
The positioning guide then is removed, and the incisions are closed.
- •
Orthodontic bone anchors are secured anteriorly between the central incisors for placement of elastics postoperatively.
- •
The patient is maintained on a soft diet for a few weeks, and the C3DO surgery can be performed 9 months later.
Stage 3: Counterclockwise Craniofacial Distraction Osteogenesis
- •
A Le Fort II or Le Fort III osteotomy is performed, based on the degree of hypoplasia of the zygomas, through a coronal incision and subgaleal dissection.
- •
The anterior edge of the temporalis origin is released but the remaining muscle is left in place to prevent atrophy.
- •
Exposure of the nasofrontal region, lateral orbital rim, anterior part of the zygomatic arch, and the medial and lateral orbital walls is performed.
- •
Next, the nasofrontal osteotomy is performed with a piezoelectric saw, and a 5-mm wedge of bone is removed to create the hinge for rotation.
- •
The piezoelectric saw is used to continue along the medial orbital wall behind the medial canthus bilaterally.
- •
An osteotome is used to complete the medial orbital wall osteotomy down to the floor.
- •
A reciprocating saw then is used to release the zygomatic arch at its junction with the zygomatic body and cut from the inferior orbital fissure through the junction of the lateral and inferior orbital rims.
- •
Next, an osteotome is inserted into the inferior orbital fissure and directed medially to complete the orbital floor osteotomy toward the previously made medial wall osteotomy.
- •
An osteotome is placed in the suborbital edge of the inferior orbital fissure and directed inferiorly along the posterior wall of the maxillary sinus, finishing with a pterygomaxillary osteotomy. If needed, an intraoral mucosal access can be used to complete the pterygomaxillary disjunction.
- •
Due to the severe clockwise rotation deformity of the maxilla, this osteotomy needs to be immediately below the skull base to avoid damage to the maxillary molar follicles.
- •
The septal disjunction then is performed with an osteotome through the nasofrontal region, aiming toward the posterior nasal spine.
- •
Down-fracturing then is performed with gentle manual pressure and the midface is fully mobilized with Rowe-Kiley forceps.
- •
Steel wires (28 gauge) or 3-0 polydioxanone sutures are placed through bone holes at the nasofrontal osteotomy site to create a hinge for the rotational movement.
- •
Prior to closure of the scalp incision, lateral canthopexies should be performed if future zygomatic reconstruction is not required.
- •
Once the scalp is closed, the preexisting Risdon incisions are used to access the mandible.
- •
VSP can be helpful to avoid injury to the mandibular tooth follicles and the inferior alveolar nerve. Additionally, it can help to achieve precise positioning of the transfacial pins to allow for parallel placement of the external mandibular distractors.
- •
Preplanned cutting/positioning guides are adapted to the mandible and secured in place.
- •
The positioning guides are used to drill the predicted holes bilaterally for the transfacial pins
- •
The planned inverted-L osteotomies positioned behind the lingula are started with a piezoelectric saw, but the inferior cortex is left intact to maintain mandibular stability during pin insertion.
- •
The cutting guides are removed.
- •
Next, 2 pairs of 0.078-in transfacial pins are passed through the predrilled holes on 1 ramus and behind the tonsillar pillar into the pharynx. A Frazier suction tip then is passed through the contralateral ramal holes into the pharynx to receive the tips of the pins. The Frazier tip acts as a guiding device; with withdrawal of the Frazier suction, the pins are guided out the contralateral holes.
- •
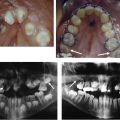
The mandibular osteotomies then are completed, and the patient is placed into the custom acrylic occlusal splint with extraoral traction posts from an embedded facebow. Suspension wires from the piriform rim and lateral maxillary buttress secure the splint.
- •
Maxillomandibular fixation is achieved using circummandibular and suspension wires from the piriform aperture and the lateral buttress.
- •
Multivector mandibular external distraction devices are attached to the transfacial pins.
- •
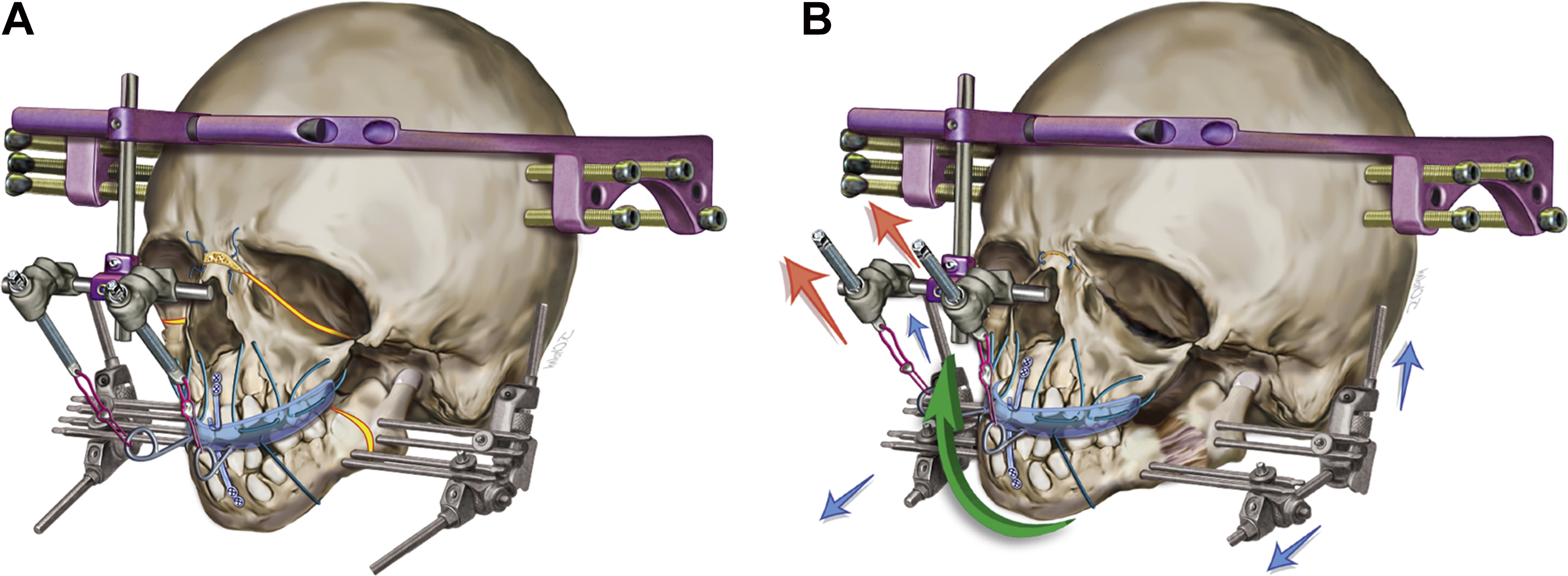
A halo external midface distraction device is secured using cranial pins.
- •
The activation posts are secured with 24-gauge wires to the traction posts on the splint and the vector is set at 45º upwards ( Fig. 3 A)