Treacher Collins syndrome (TCS) is a genetic disorder that presents with a variety of craniofacial deformities. One classic feature of TCS is a steep, counterclockwise rotation of the occlusal plane, and microretrognathia with bony deficiencies in both the body and ramus of the mandible. This morphology commonly necessitates reconstruction by the craniofacial surgeon. This article discusses strategies and considerations for surgically correcting the mandibular deformity associated with TCS using mandibular distraction osteogenesis and other related techniques. The proper implementation of these techniques can yield excellent results that greatly improve quality of life in this challenging patient population.
Key points
- •
Patients with Treacher Collins syndrome (TCS) and a tracheostomy or severe sleep apnea may be candidates for mandibular distraction osteogenesis, which can expand the oropharyngeal airway and lengthen the mandible.
- •
Reconstruction of the TCS mandible poses a unique challenge to craniofacial surgeons, because bony deficiencies and deformities are seen along both the body and ramus of the mandible. More recently described techniques, such as curvilinear distraction and counterclockwise distraction, offer surgeons improved surgical options when addressing the TCS mandibular morphology.
- •
Even with proper implementation of these techniques, the rates of complications and relapse in mandibular reconstruction in patients with TCS tend to be higher than in other craniofacial conditions. Proper surgical management and planning, including the use of virtual surgical planning (VSP) software, can help mitigate risks and improve outcomes.
- •
Because patients with TCS typically require multiple procedures throughout childhood, surgeons must work closely within a multidisciplinary team in order to optimize long-term functional and quality-of-life outcomes.
Background
Treacher Collins syndrome (TCS), also known as mandibulofacial dysostosis, is a rare autosomal dominant genetic disorder with variable expressivity. , Early descriptions of this condition by the ophthalmologist Edward Treacher Collins reported bilateral and symmetric abnormalities including orbital coloboma and periorbital dysmorphology. The clinical findings in TCS are caused by abnormalities of the first and second branchial arches, which can manifest with a variety of asymmetric craniofacial sequelae ranging from mild to severe. Although the molecular underpinning of TCS remains a subject of study, most cases have been linked to a variety of mutations within the TCOF1 gene on chromosome 5, which are thought to disinhibit the ribosome biogenesis pathway.
Clinical features
The clinical features of TCS, although variable, are distinct from other craniofacial conditions. Patients with TCS present with a convex facial profile, a prominent nasal dorsum, and a retrognathic lower jaw ( Fig. 1 ). A distinct feature is the ocular and periorbital findings, as described by Collins. Patients typically have dysmorphic orbits, downslanting palpebral fissures, and malar hypoplasia, resulting in an enophthalmic or birdlike appearance. Vision loss, congenital cataracts, and microphthalmia can be seen in severe cases. The most common periorbital abnormalities include (1) thin lower lid skin with lateral canthi malposition, (2) colobomas, (3) periorbital dermoids, (4) attenuated or absent orbicularis oculi muscles, (5) meibomian glands puncta, and (6) atresia of the lacrimal duct. Laxity of the lid margin and absence of lashes are also highly characteristic.

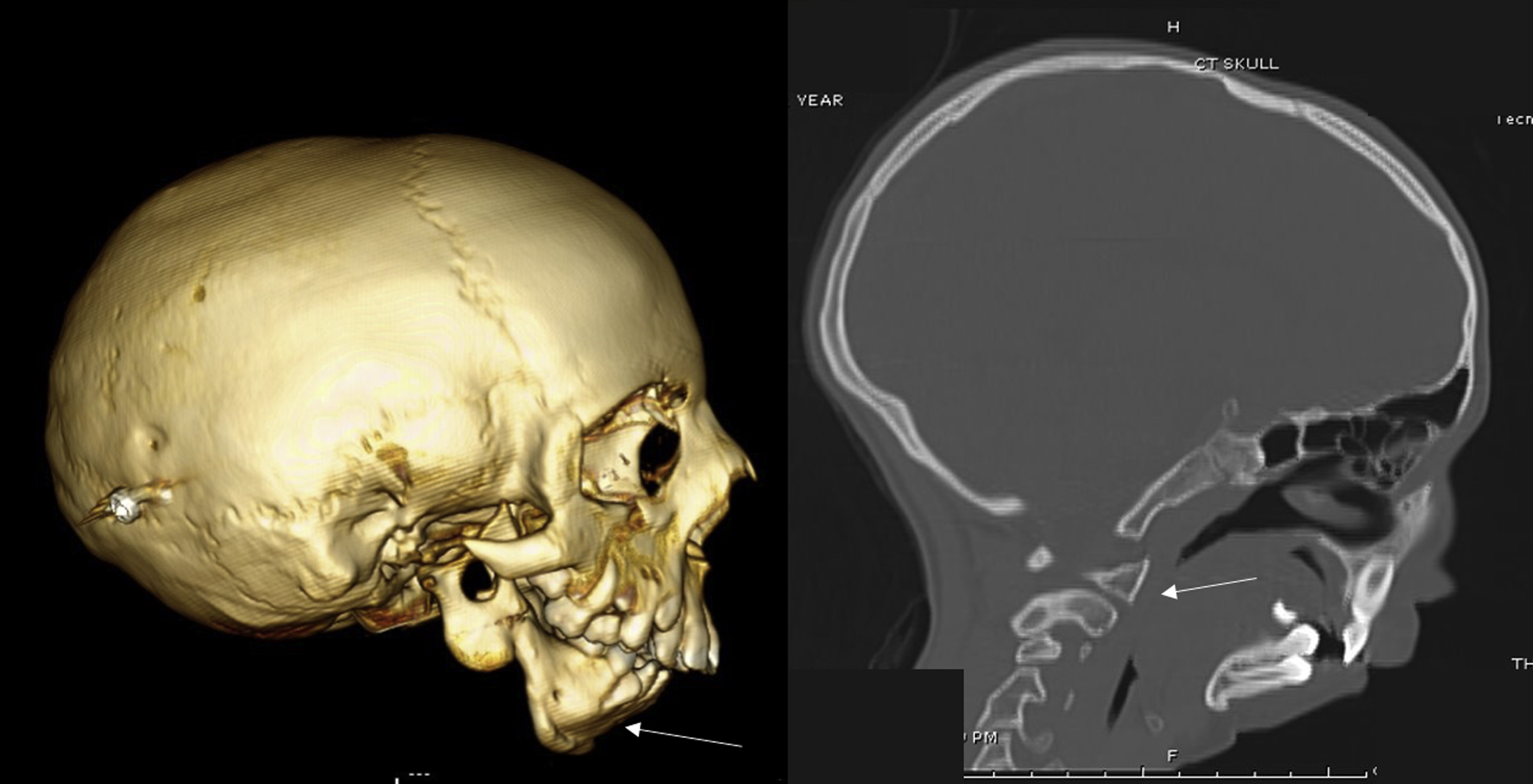
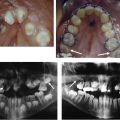
In addition to periorbital dysmorphology, patients with TCS also possess a characteristic dysmorphology of the maxilla and mandible ( Fig. 2 ). These features include decreased sella-nasion-B point, decreased height of the lower third of the face, and a steep, clockwise rotation of the occlusal plane leading to an Angle class II anterior open bite malocclusion. This dysmorphology stems largely from decreased ramal height, and significant condylar hypoplasia is also seen at higher rates among patients with TCS compared with normal controls. , Condylar hypoplasia can secondarily result in temporomandibular joint (TMJ) dysfunction. Importantly, these mandibular and maxillary dysmorphologies frequently cause marked glossoptosis with associated upper airway obstruction; obstructive sleep apnea (OSA) can be seen in as many as 95% of patient with TCSs, and, as a result, some require tracheostomy to ensure airway patency.
Other common features of TCS include microtia, cleft palate with or without cleft lip, and malar and zygomatic hypoplasia with decreased width of the midface. A bony cleft is often observed at the zygomatic arch with limited formation of the residual zygoma, including the glenoid fossa. Other craniofacial skeleton abnormalities include a reduced cranial base angle with decreased anteroposterior length and bitemporal width. Additional but less common craniofacial findings include choanal atresia, complete or submucous cleft palate, and absent parotid glands. Extracranial features can also include cryptorchidism, renal abnormalities, congenital heart disease, and extremity malformation. The summation of these multiple deformities commonly produces significant functional and aesthetic concerns, as well as psychological/social challenges in affected patients.
General principles on the management of Treacher Collins syndrome
Early management of TCS should be directed toward functional aspects of care, most importantly airway assessment and (when needed) intervention. The degree and type of airway obstruction (choanal atresia, glossoptosis, lower airway obstruction) should be identified through complete endoscopic airway analysis. When indicated, polysomnography can quantify the extent of airway obstruction and provide a baseline of function. Management of airway deficiency depends on the severity of obstruction; in the most severe cases, intubation or tracheostomy may be required at an early age.
Early intervention priorities for patients with TCS include feeding, growth, and ocular evaluation. In patients with severe retrognathia, oral feeding can be a challenge and gastrostomy tube placement may be necessary. Specific education is sometimes needed to aid patients in feeding, especially among patients with cleft palate. Ocular evaluation must be performed to assess the degree of eye involvement. Tarsorrhaphy may be required to prevent permanent corneal damage.
Following, and sometimes concurrent with, early management, children with TCS should undergo multidisciplinary craniofacial assessment to address their functional and aesthetic challenges. Surgical evaluation is an early priority in patients with severe expressions of TCS associated with significant functional compromise.
Mandibular distraction
Overview
Surgical evaluation of the mandible should be an early area of focus, because the marked mandibular retrusion secondary to loss of posterior facial height and clockwise rotation of the mandible can lead to glossoptosis and upper airway obstruction. The narrow pharynx commonly found in many patients with TCS compounds upper airway obstruction caused by the retropositioned tongue. Prior studies have documented the sites of airway obstruction in TCS and have found that the entire upper airway respiratory tract from nasopharyngeal to laryngeal level may be affected. These studies have found a strong correlation between craniofacial morphology and airway findings, highlighting the importance of both endoscopic airway studies and computed-tomography imaging prior to any intervention. The goals of surgical management are centered on either achieving definitive airway control (ie, tracheostomy) or improving airway volume through the use of tongue-lip adhesion, mandibular advancement (orthognathic surgery), or mandibular distraction osteogenesis (MDO).
Mandibular Distraction Osteogenesis Indications and Timing in Patients with Treacher Collins Syndrome
The strict or relative indications for MDO remain a subject of debate. In the past, mandibular distraction was largely reserved for patients requiring decannulation , . While recent advancements in techniques for TCS have shown promise for intervention prior to tracheostomy or in patients with less severe deformities, MDO is still generally reserved for cannulated patients and/or those with moderate/severe OSA.
Although evaluation and planning for mandibular distraction should begin early, the procedure itself should be delayed until early childhood (age of mixed dentition) if the airway is stable and the OSA symptoms are limited such that they can be managed conservatively. Waiting as long as possible minimizes the risk of multiple distractions before the patient reaches skeletal maturity. Initial distraction around ages 8 to 10 years followed by definitive orthognathic corrective surgery in late adolescence is preferred, when possible. The exact timing of surgery should be guided by the sleep study and functional evaluations performed.
In addition to an assessment of functional and airway status, proper imaging assessment through computed tomography (CT) should be performed to determine the anatomic feasability of MDO.
The extent of bony loss and mandibular deformity all have implications to the patient’s candidacy for mandibular distraction. For example, a lack of condyle(s) or deficient TMJ anatomy is a contraindication for MDO, although there are strategies for overcoming these deficiencies in some patients (described later). Severe clockwise rotation of the mandible can also be difficult to definitely correct through distraction. If distraction is pursued in these cases, patients should be informed of increased risks of mandibular relapse.
Preoperative Virtual Surgical Planning
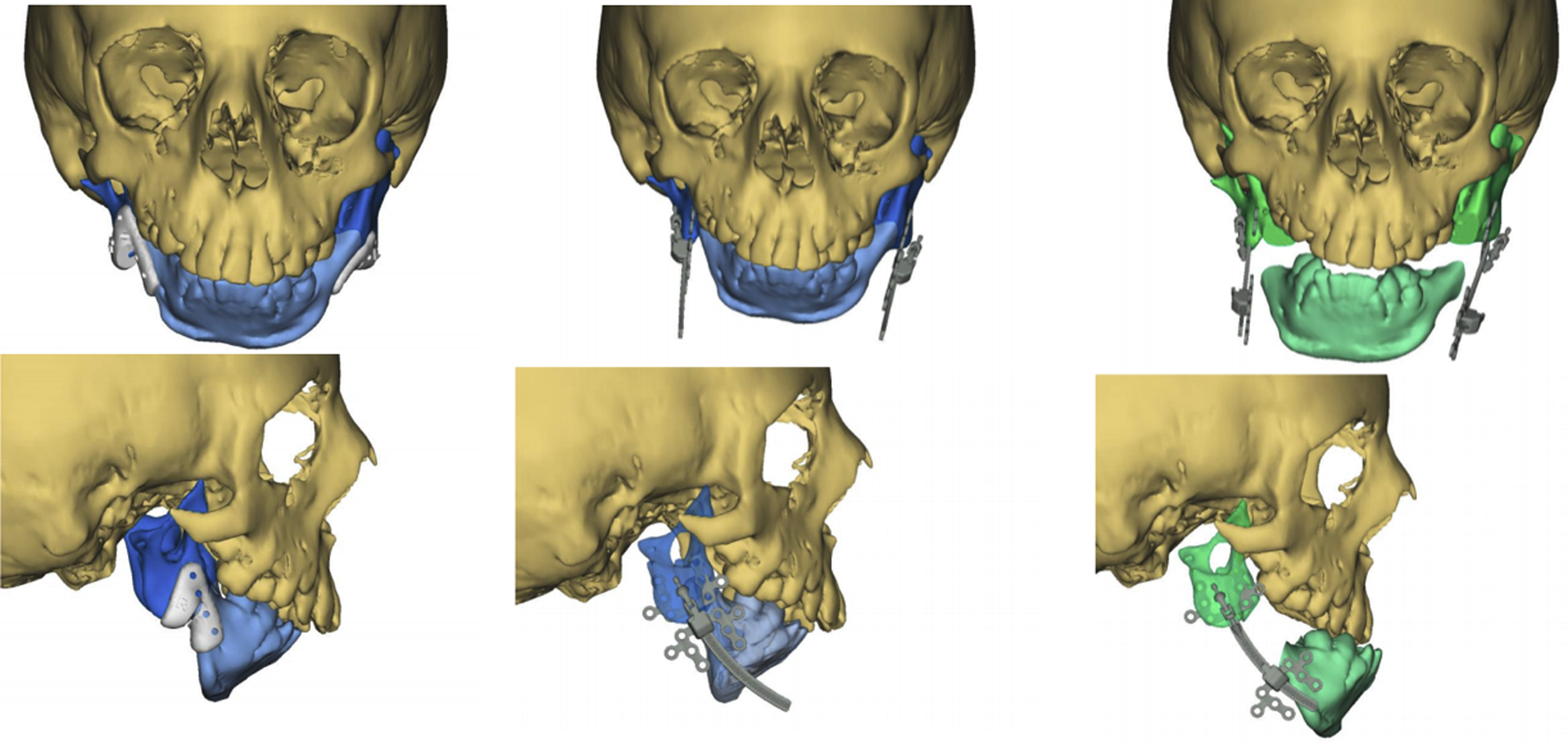
Before the introduction of virtual surgical planning (VSP) and three-dimensional (3D) printing technology to craniofacial surgery, several studies documented the associated detrimental effects of MDO on (1) injury to developing tooth buds, (2) deformational growth effects on the mandible, (3) facial soft tissue scarring, (4) inferior alveolar nerve damage, and (5) mandibular hypomotility caused by TMJ ankyloses. However, the more recent experience of MDO in patients with TCS has been favorable with the introduction of computer-assisted design and computer-assisted manufacturing, which enables surgeons to design osteotomy guides and simulate hardware placement virtually ( Fig. 3 ). In our experience, VSP osteotomy guides substantially decrease the risk of iatrogenic injury to the inferior alveolar nerve or tooth buds, and preoperative simulation also allows finer control of the distraction vector. VSP has also been shown to help craniofacial surgeons perform preplanned mandibular and curvilinear distraction with a high degree of accuracy across a variety of surgical approaches, and has been associated with improved outcomes among patients receiving other forms of mandibular reconstruction.
Given the benefits associated with VSP and the inherently challenging morphology seen in patients with TCS, the senior author routinely uses VSP before any TCS-related MDO in order to improve clinical outcomes. The senior author acquires a preoperative maxillofacial CT scan in all surgical patients with TCS and performs virtual simulation of the procedure with an industry partner that provide VSP services.
Technique
As previously discussed, MDO in patients with TCS is challenging, and prior reports have associated MDO with high rates of relapse and an inability to adequately maintain airway patency. , This problem is likely attributable to the significant deficiency of the TCS mandible in both mandibular height (ramus) and length (body), as well as the well-defined clockwise rotation of the deformity. Because of this rotational morphology, univector distraction lengthening or genioglossus advancement are often limited in their capacity to correct the deficiencies. Thus, treatment of patients with TCS may require more creative surgical approaches. Regardless of technique, MDO in patients with TCS should be performed with adequate understanding of the physiology and principles of distraction as well as the anatomic deformity affecting the jaw.
Although univector MDO is the most frequently used technique for patients with TCS, , the authors preferred approach is curvilinear distraction osteogenesis, which can address both the vertical and horizontal mandibular deficiencies. Although curvilinear distraction is advocated by the senior author, other distraction techniques may be indicated depending on the patient’s craniofacial morphology.
Curvilinear Distraction Osteogenesis
Many multiplanar distraction techniques have been developed to overcome the shortcomings associated with standard, univector MDO. At our institution, our preferred technique is curvilinear distraction to reconstruct the jaw deformity associated with TCS in growing patients. , First introduced by Schendel and coworkers in 2000, curvilinear distraction builds on the premise of a logarithmic growth pattern of the mandible. Curvilinear distraction regenerates mandibular bone stock in both the body and ramus, and corrects the clockwise dysmorphology along a natural curved path. This technique has been shown to be an effective treatment of neonatal OSA and TCS. ,
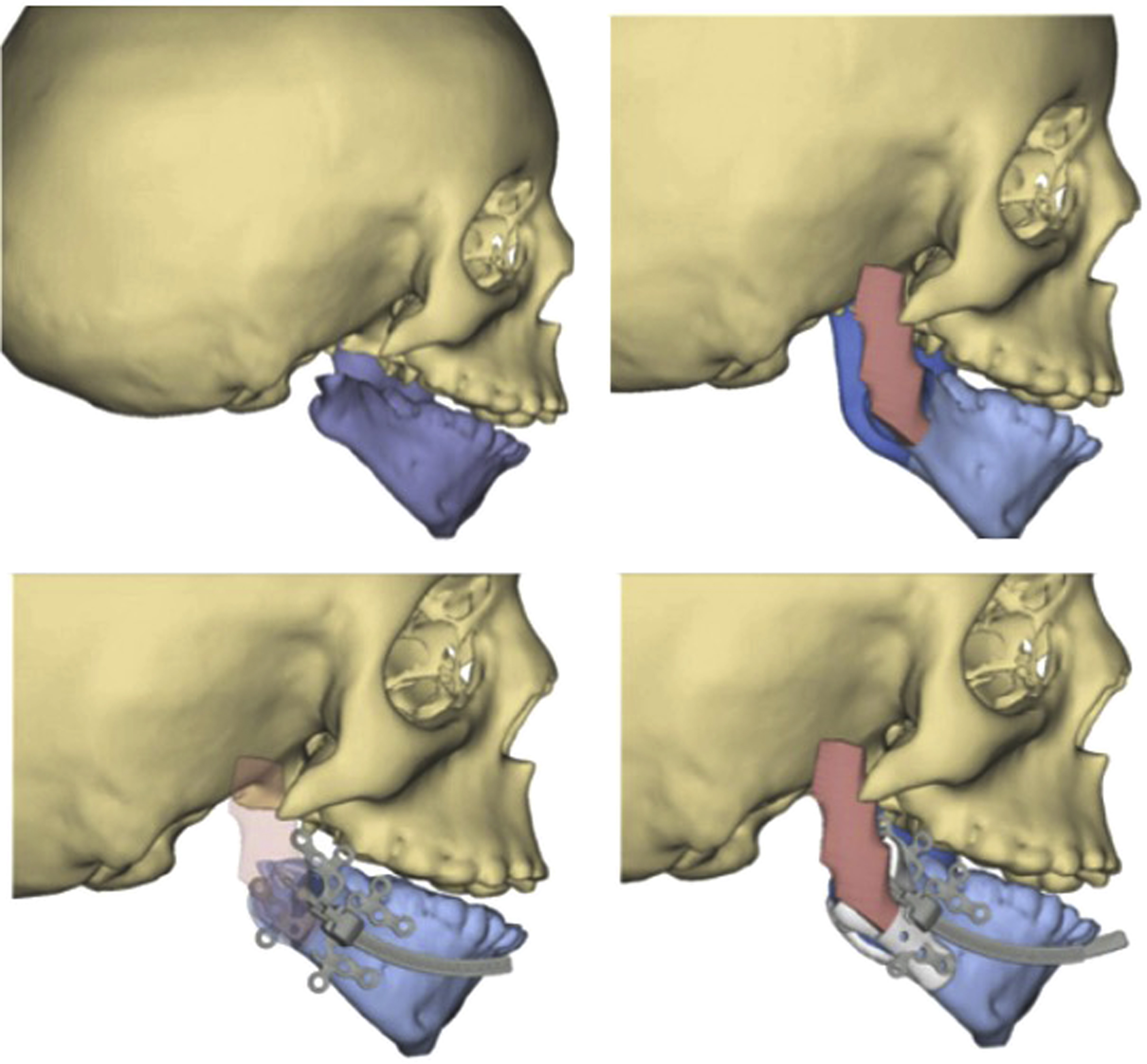
Our surgical approach is similar to that described by Kaban and colleagues. A standard extraoral approach is implemented, with an incision placed 2 cm inferior to the mandibular border, followed by sharp dissection through the platysma and elevation of a wide subperiosteal envelope. A wider subperiosteal dissection is typically required to accommodate the VSP cutting guide. An osteotomy line is drawn after securing the VSP guide ( Fig. 4 ) on the inferior aspect of the antegonial notch and angle and preplanned fixation screw pilot holes are made both proximal and distal to the osteotomy (at least 2 anteriorly and posteriorly). The guide can then be removed, and corticotomies and/or osteotomies performed. After execution of the osteotomy, the distraction device is placed. The curvilinear device can then be assembled and secured (see Fig. 4 ); mobility of the osteotomized segment should be ensured bilaterally. Distraction arms can be posteriorly attached through stab incisions that exit postauricularly.

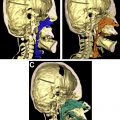
One challenge when performing distraction in patients with TCS is the lack of a natural skeletal condylar or TMJ. The senior author believes that a condyle or TMJ structure is necessary to perform MDO. One approach for overcoming this limitation is reconstructing the entire costochondral ramus and TMJ. Previously, we reported a procedure in a patient with hemifacial microsomia in which autologous bone graft was used to reconstruct the ramus-condyle unit simultaneously with curvilinear distraction. We used a scalp flap (taking care to avoid tissue needed for ear reconstruction) to create a neo-TMJ, and a costochondral rib graft to reconstruct the mandibular ramus and condyle ( Fig. 5 ). This approach created a proximal stop that allowed curvilinear distraction with good effect.
Distraction Protocol
Postoperatively, patients are kept in the hospital overnight for pain control and monitoring. Correct placement of the device is confirmed by plain film radiograph on postoperative day 1. The patient’s family are thoroughly educated during the period of distraction to ensure proper understanding of the device.
Distraction is performed according to protocols previously described by the senior author, with consideration of 3 distinct stages following the operation: latency, activation, and consolidation ( Table 1 ). The latency period typically lasts 5 to 7 days in young children or 1 to 2 days in infants, and allows for the formation of a preliminary callous at the site of the osteotomy. Following this period, active distraction is performed to slowly expand the bone space and allow for the formation of new bony matrix. We typically perform distraction at a rate of 0.5 to 1.0 mm in older children, and 1.0 to 2.0 mm in infants. Serial weekly radiographs and close biweekly or weekly follow-up is required during this time to ensure adequate family education and monitor active distraction ( Fig. 6 ). Completion of activation is achieved at the preplanned interval, at which time distraction arms can be removed. Class III occlusion is the target mandibular position in the growing face. The consolidation phase typically lasts 6 weeks or longer (twice the activation period is a useful reference), and allows for final bony ossification. After consolidation, the device is removed. Exposure of the mandible for device removal incorporates the same incision used during device placement. Scar revision is often performed at this time to optimize aesthetic appearance.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


