Alveolar distraction osteogenesis (ADO) has been used for the reconstruction of atrophic alveolus for decades. The advantage of this technique is that it augments the bone and soft tissues together, creating a better alveolar platform for subsequent surgeries and dental rehabilitation. It is especially useful in patients with large and/or complex alveolar clefts for which approximating the alveolar segments reduces the size of the bony cleft and associated fistula. Displacement of the transported segment is the most frequently encountered complication of ADO but can be managed by constructing case-specific distractors.
Key points
- •
Alveolar distraction is used for lengthening, widening, or augmenting the alveolus in patients with a wide or complex alveolar cleft.
- •
Alveolar distraction can approximate the alveolar segments to reduce the size of the bony deficiency and the fistula.
- •
A smaller alveolar cleft and smaller fistula leads to more predictable outcomes to bony reconstruction.
Introduction
Congenital or acquired alveolar bone defects often are encountered in the dental practice. The former generally are associated with craniofacial anomalies, such as cleft lip and palate. These bony deficiencies have stereotypical characteristics, such as maxillary halves with deficient bone, lack of nasal floor support, and a hypoplastic maxilla. Acquired alveolar defects may be caused by trauma, periodontal diseases, tooth extraction, congenital tooth agenesis, and tumor resection and can present in a more variable pattern. Alveolar defects can be primarily in the horizontal dimension and often are associated with vertical resorptions, which require bone augmentation. In modern dentistry, restoration of the missing teeth and atrophic alveolus in patients with or without cleft has shifted from large obturators and bulky removable prostheses to providing a bony platform for implant restorations and an esthetic soft tissue lining of the smile.
Several augmentation methods have been developed for increasing the volume of alveolar bone for patients without a cleft. Autologous or allogenic grafting is a common technique used to establish a bony platform for dental rehabilitation in patients with atrophic alveolus of various etiologies. Although successfully treated cases have been reported in the literature, there are limitations of these grafting procedures. For example, the bone grafted area may resorb due to poor stabilization, limited bone contact, soft tissue tension, and vascularization problems due to the large volume of the graft material. , As an alternative treatment to grafting, alveolar distraction osteogenesis (ADO) has been suggested to increase bone volume in patients with and without cleft. The common indications for the general population in dental practice and specific indications for the cleft lip and palate population are summarized from an orthodontist’s perspective.
Goals of alveolar distraction
ADO has become increasingly popular in orthodontics after rapid canine retraction with the distraction procedure was introduced by Liou and colleagues for shortening the treatment duration. Several types of distractors and distraction types have been introduced for different purposes, including lengthening, widening, and augmenting the alveolus. Indications and conditions include
- •
Rapid canine distalization
- •
Atrophic alveolus due to congenital missing or lost teeth and edentulous jaws ,
- •
Management of ankylosed teeth
- •
Alveolar/partial jaw deficiencies after tumor resections or trauma
- •
Approximation of cleft segments in patients with cleft lip and palate
The goals of ADO include
- •
To improve the shape of the alveolar arch in 3 dimensions (3-D)
- •
To expand the alveolar bone volume for subsequent orthodontic treatment
- •
To restore the vertical height of the alveolus before dental rehabilitation (implant placement and prosthetic restoration)
Multiple alveolar distraction procedures have been described to treat bony and soft tissue deficiencies of the jaws. These procedures are summarized as vertical, horizontal, and sagittal distraction techniques as well as alveolar distraction in patients with a cleft. A 3-D understanding of the bony and soft tissue deficiencies associated with the defect is critical to planning an effective treatment plan.
Vertical alveolar distraction
Vertical alveolar distraction (VAD) is used to treat local alveolar atrophy caused by traumatic tooth loss, previous failed grafting, or an ankylosed tooth. , VAD was first reported as a case series by Chin and Toth in 1996, in which different distraction methods were described. Included in this study was a patient who had suffered a traumatic injury and required bone and mucosa augmentation in the anterior mandible. The investigators distracted the atrophic edentulous bone vertically, which allowed them to insert implants for dental rehabilitation. Now, after 2 decades of use, the method is considered an excellent solution for bone and soft tissue regeneration in areas with significant bone atrophy.
A systematic review of VAD concluded that survival rate of the dental implants in cases utilizing vertical distraction was similar to those without any augmentation technique. Generated bone height can be up to 15 mm in certain cases. Although VAD has shown to be a useful tool for bone and soft tissue augmentation, overcorrection at a 10% to 20% rate is recommended, because a degree of relapse may occur during consolidation period. Additionally, although this technique has been reported in more than 300 cases in the literature, long-term data are lacking. Of the available studies that discuss long-term results, the alveolar marginal bone demonstrates approximately 15% to 20% resorption at 5-year follow-up.
Horizontal alveolar distraction
Horizontal alveolar distraction (HAD) is used for expanding the atrophic alveolar crest. This widening has been performed conventionally using different bone grafting procedures. Similar to conventional vertical augmentation techniques, these routine surgeries have resulted in severe bone resorption. Therefore, alveolar distraction technique has been suggested by dental practitioners who experienced bone resorption and difficulty inserting osseointegrated implants. Osseointegrated implants cannot be inserted successfully in patients exhibiting an alveolar ridge less than 5 mm and the narrow alveolus hinders the orthodontic tooth movement due to the insufficient bone coverage of the teeth. HAD has been used since 2004 and has been shown superior to conventional grafting due to less infection risk and minimal resorption postoperatively.
Both VAD and HAD are preferred in select cases due to the decreased overall treatment time compared with conventional staged bone grafting techniques. Sufficient bone generation by the distraction allows for stable implant restoration without the need for graft surgery. The relapse or resorption of the generated bone has been found to be limited. Long-term data and prospective randomized clinical trial assessment, however, are lacking.
Sagittal alveolar distraction
ADO in the sagittal plane has been commonly preferred in patients with cleft lip or palate for reducing the cleft gap and in patients who have undergone partial resection of the maxilla or mandible due to a tumor resection. Patients with cleft lip or palate may have deficiencies in any of the 3 planes that require vertical, horizontal, or sagittal distraction, and the geometry of bony deficiency must be correctly diagnosed in 3-D in order to formulate an effective treatment plan.
Alveolar distraction for patients with cleft
Nature of the Problem
In patients with a cleft, alveolar defects requiring VAD or HAD present unique challenges because an oral cleft commonly is associated with oronasal communication and a soft tissue deficiency. There is a wide variation in the extent of the cleft deformity from mild to severe and many alveolar defects easily can be managed using traditional surgical and orthodontic techniques. Complex alveolar defects associated with a large fistula, wide bony gap, rudimentary premaxilla, or a malformed cleft segment may benefit from more specialized interventions. Different techniques have been suggested for the reconstruction of these defects, such as buccal or tongue flaps as well as obturators to cover the remaining cleft defect. , Although secondary alveolar bone grafting is the gold standard for reconstruction n of the maxillary bony cleft, the presence of a hypoplastic maxilla, significant vertical discrepancy of the alveolar segments and minimum contact surface between the cleft segments, malposition of the segments in more than 1 dimension, and soft tissue deficiency are considered risk factors for grafting surgery. Additionally, cases of flared or deviated hypoplastic premaxilla with large cleft gaps also pose challenges for traditional grafting techniques due to blood supply and deficiency of the soft and hard tissues and often lead to grafting failures or unideal reconstructions. Moreover, previous surgeries and failed grafting procedures leave more scar and resorptive bone margins behind, making future procedures more challenging for clinicians. In such cases, ADO has been suggested as an alternative method to increase the success rate of the grafting procedure and increase the bone volume.
The orthodontic treatment of a patient with a cleft also is challenged by additional variables not related directly to diagnosis of cleft lip and palate. For example, the Decayed, Missing, and Filled Teeth (DMFT) index rate has been reported to be significantly higher than in noncleft controls, regardless of the sample origin. Furthermore, tooth anomalies, malpositions, and malformed roots frequently are observed in these patients. These anomalies and alveolar bone deficiencies can create challenges to orthodontic treatment, because the use of routine orthodontic anchorage systems may not be feasible. In these cases, alveolar distraction is recommended to obtain better surgical and orthodontic results.
Clinical Relevance
ADO has been implemented in select patients with a cleft due to the ability to decrease the size of the alveolar gap, which can increase the success rate of subsequent bone grafting. Liou and Chen suggested the use of alveolar distraction when the cleft gap is wider than a canine tooth. Because large cleft gaps and the presence of large oronasal fistulas are particularly challenging to repair, commonly requiring repetitive surgeries, ADO may be an important treatment options in this challenging subset of patients. There is no consensus on the treatment of oronasal fistulas located in the alveolar region in the literature. It was stated that the closure of the fistulas can be done at the time a bone graft is done, which provides stability and maxillary continuity. In cases of a large fistula located at the hard palate near the alveolus, the fistula can be reduced by the distraction, resulting in a smaller defect that can be closed more easily. Liou and Chen reported their 21 cases in which they performed alveolar distraction procedure for approximation of the cleft segments. They obtained an average of 12-mm distraction with a range of 10 mm to 20 mm, and their 5-year follow-up showed stable results.
Another advantage of alveolar distraction is providing vertical alignment of the cleft segments when needed. This can be achieved by either performing VAD following sagittal transposition as reported by Rachmiel and colleagues or by remodeling the soft callus after the distraction period. Because VAD can align the alveolar segments properly in the vertical plane, bone graft survival is improved through the formation of better contact surface between the alveolar segments.
ADO also expands the mucoperiosteal lining associated with the transported bone, decreasing soft tissue tension at the time of bone graft, and improving graft take. The restoration of a single-piece maxilla facilitates future orthognathic surgery. Furthermore, sagittal transposition of the lesser segment medially delivers osseous tissue to the deficient nasolabial area, providing better structural support of the soft tissues as well as an augmented bony foundation for orthodontic tooth movement, resulting in a more pleasant prosthetic restoration. Finally, improvement of the maxillary arch can be facilitated by this approach (from V shape to ovoid arch form) as well, if there is a lack of bone in the anterior region. Even though providing a curvilinear arch form is not easily established, case-specific devices and postdistraction orthodontics are utilized to obtain a good platform. Although ADO has been shown beneficial, randomized controlled trial studies that compare success rates of traditional alveolar grafting to ADO methods currently are lacking.
Presurgical Orthodontic Preparation
Presurgical orthodontics include aligning the teeth to establish a robust anchorage, creating a sufficient interdental space for the osteotomy site and making a case-specific appliance for the distraction. Maxillary teeth are aligned first, as much as the alveolus remodeling capacity allows. Next, a stainless steel rectangular arch wire should be engaged to the brackets. This arch should be as large as possible to provide stability for future alveolar transposition. This arch wire also can be used to expand the maxillary arch just after the activation period in the event that the transport segment collapses palatally. A transpalatal arch bar made of stainless steel can be used for guiding the transport segment direction and to prevent medial and palatal collapse. , , Erverdi and colleagues describe using metal crowns if the number of the teeth are not sufficient for the anchorage.
In certain complex cases, there may be multiple occlusal planes due to differing vertical positions of the alveolar segments. In these cases, the use of segmental arches is recommended in order to avoid excessive tooth movement; thus, aligning the teeth is done separately for each segment. Following the leveling, interdental space is enlarged orthodontically at the planned osteotomy site for avoiding any periodontal injuries and root damage. It has been suggested that a 3-mm gap should be released orthodontically between teeth and the osteotomy line. If the incisor tooth adjacent to the cleft is rotated or extremely retruded and enough bone coverage of the teeth on the cleft side exists, it can be derotated orthodontically to create an accessible surgical area.
Periodontal health is of great importance to ensure the success of soft tissue distraction. As in traditional grafting procedures, oral hygiene should be optimized preoperatively and postoperatively to avoid bone resorption. Another important aspect to consider is elimination of possible primary contacts of the transporting segment because of the overerupted or inclined teeth at the maxillary or mandibular arches on the planned route. To avoid this risk, a removable acrylic plate can be made for the mandibular arch to prevent premature contact of the tooth apices during activation and to establish a smooth platform for the transportation.
Distraction procedure
The age of 9 years to 10 years is the suggested age for alveolar distraction for cleft approximation in order to graft the area before canine eruption. In cases that require tertiary bone graft (after canine eruption), ADO can be performed at any time prior to the bone graft procedure. Alveolar distraction involves osteotomy, latent phase, transport (active distraction), and consolidation periods similar to distraction in other craniofacial areas.
The latency period in alveolar distraction should be between 4 days to 7 days. , , The length of this period is determined according to the extent of soft tissue healing. The rate of activation should be 0.5 mm or 1 mm per day, with a frequency up to twice a day. The distraction procedure is continued until the transport segment reaches the targeted area by closing the alveolar gap in cleft population or planned final tissue expansion in the noncleft population. Caution should be used, because the amount of distractor activation tends to be more than the estimated amount, and the actual increase in width might not be the same as the amount of activation. Therefore, an amount of activation exceeding the size of the alveolar cleft should be planned for, and the distractor device should have enough capacity to fulfill this increased need.
The distracted segment should be translated without inclination toward the greater segment (or premaxilla) to maximize surface apposition between the alveolar segments and to minimize displacement between the segments. In certain cases, early contact can occur due to bone irregularities or soft tissue prominences along the advancing surface. Under these circumstances, the transported segment may be tilted during activation to optimize reduction of the alveolar cleft. Therefore, the final position of the alveolar segment should be determined by: best reduction of the maxillary cleft an occlusion. If the alveolar gap is larger than 2 mm, a bone grafting procedure is suggested and if it is less than 2 mm, then gingivoperiosteoplasty may be considered. Gingivoperiosteoplasty is more efficacious when performed at the time of infancy. An important factor during the activation period is the soft tissue expansion of the mucosal lining during the distraction process. Otherwise, soft tissue dehiscence can occur, resulting in an open wound that could risk the success procedure.
When activation is completed, the distractor is converted to a passive mode as a consolidation device. After a consolidation between 3 months and 4 months, , alveolar bone graft is performed and postdistraction orthodontics is completed to move the teeth distally into the generated bone.
Types of distractors
The choice of distractor (custom-made or manufactured) depends on the clinical circumstances, including the type of bone defect, dentition, and experience of the clinicians. Alveolar distractors can be classified as tooth-borne, bone-borne, or hybrid based on the anchorage type. Liou and Chen, who reported the first alveolar distraction for approximating the cleft segments, used tooth-borne distractors, which were attached to the dentition only. Erverdi and colleagues also designed a tooth-borne distractor that they referred to as “archwise distraction” for the cleft approximation. Clinicians who use tooth-borne devices report that arch wire guidance can transport the alveolar segment to achieve an anatomic curvilinear movement along the dental arch. , , In contrast, Mitsugi and colleagues prefer bone-borne devices for sagittal distraction because tooth-borne devices impose a burden on the teeth and caused an unstable fixation, which is unfavorable for controlled bone transport. They reported 22 cleft cases that underwent ADO with fabricated bone-borne distractors and reported a degree of curvilinear transport was achieved through guidance of the arch wire. Rachmiel and colleagues also used bone-borne distractors for both sagittal and vertical distraction in a patient with severe cleft defect.
Rapid palatal expansion screws (hyrax-type) commonly are used for custom-made devices, which can reduce cost of care. This screw can be inserted parallel to the palatal surface or along the vestibular side of the teeth. Various designs using these expansion screws have been introduced according to the anchorage site and the planned route of the transport segment. , Zemann and colleagues reported 6 cases that underwent alveolar distraction and achieved curvilinear transport of the segment using an expansion screw at the buccal side and a transpalatal bar. Other clinicians prefer to combine tooth-borne devices and temporary anchorage devices (TADs). Both expansion screw devices and fabricated intraoral distractors should be oriented properly to avoid any protrusions through the buccal side or the palatal side, which can cause tongue irritation.
Case presentations
The following cases reports are successful applications of ADO using bone-borne or a combination of tooth-borne and bone-borne devices in patients with a cleft.
Case 1
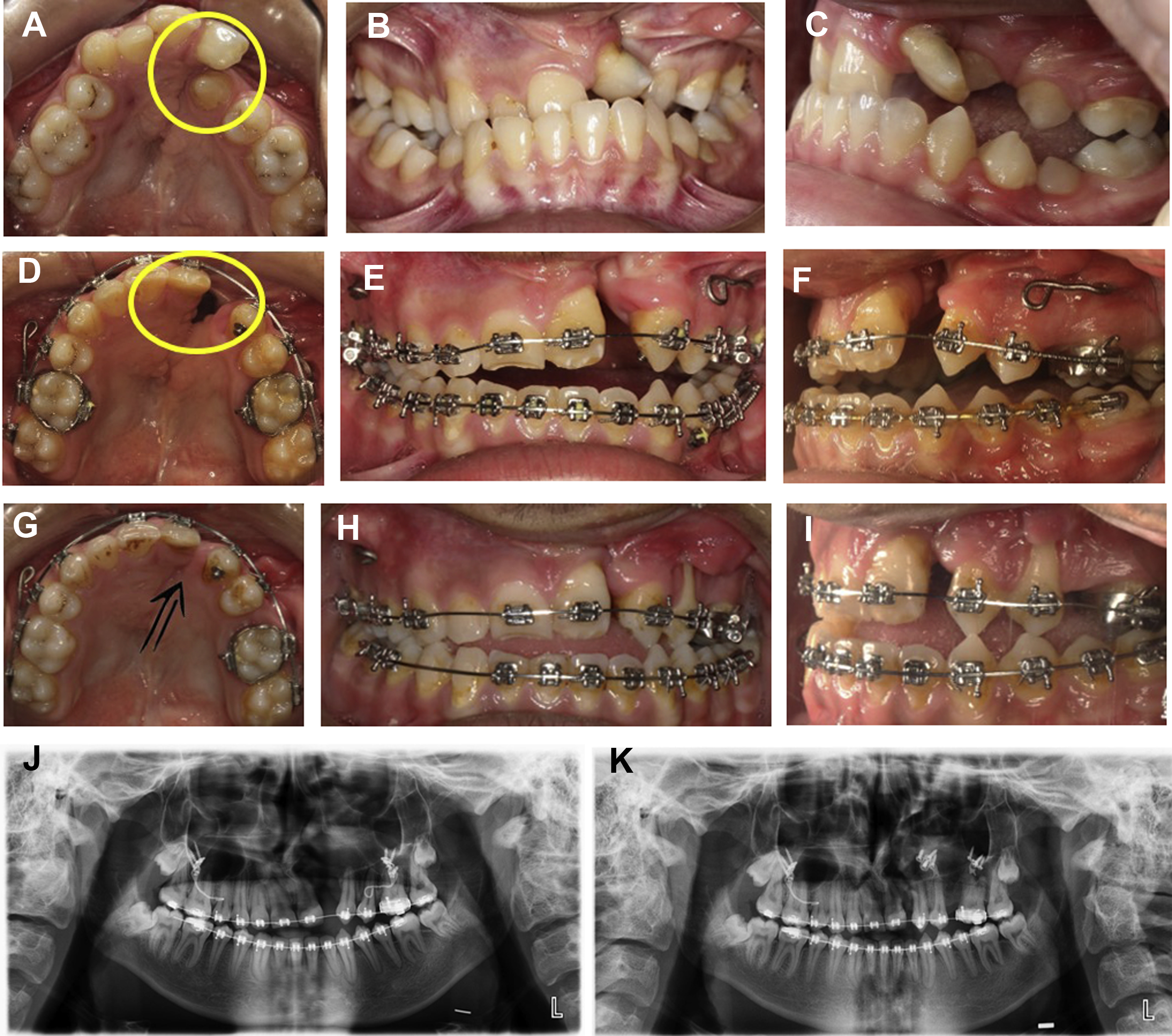
An 18-year-old man with unilateral cleft lip and palate presents with a large oronasal fistula and an alveolar cleft on the left side ( Fig. 1 A–C). Alveolar distraction was planned to reduce the alveolar cleft following presurgical orthodontics. After inserting brackets and arch wires, maxillary teeth were aligned and an extremely rotated left incisor tooth was derotated. The lesser segment was expanded by using arch wires ( Fig. 1 D–F). After 11 months of fixed orthodontic treatment, a fabricated alveolar distractor was applied to the lesser segment. The activation rate was 0.5 mm/d with twice-daily activation for a period of 3 weeks. The same distractor was used during the consolidation period of 4.5 months ( Fig. 1 G, H). Alveolar bone graft was performed after consolidation was completed. A gingival recession occurred at the maxillary first premolar ( Fig. 1 I). Postoperative panoramic radiograph showed narrowing of the alveolar cleft and new bone at the cleft site compared with the presurgical panoramic radiograph ( Fig. 1 J, K). Orthognathic surgery was planned for the maxillomandibular discrepancy.