Maxillary hypoplasia is a commonly seen dentofacial anomaly in patients with cleft lip and palate after surgical repair of the cleft anomaly. To facilitate large horizontal movements of the maxilla, distraction osteogenesis is used to slowly stretch the soft tissue envelope with the skeletal advancement preventing tissue recoil and skeletal relapse. Internal distraction devices have the advantage of reducing the amount of physical and psychological stress placed on patients, families, and caregivers. The technique has been successful in producing stable results for large advancements of the facial skeleton when compared with conventional Le Fort I advancement and fixation of the maxilla.
Key points
- •
Distraction osteogenesis should be considered in advancement of the maxilla greater than 10 mm.
- •
Internal distraction is a safe and efficacious modality for the correction of midface hypoplasia after cleft lip and palate repair.
- •
Internal distraction devices have the advantage of reducing the amount of physical and psychological stress placed on patients, families, and caregivers.
- •
Internal distraction can facilitate larger movements of the maxilla than traditional advancement and fixation without significant relapse or nonunion.
- •
New innovation in internal distraction devices has addressed previous disadvantages of internal distraction, such as limitations on distraction distance and inability to adjust distraction vector.
Introduction
Maxillary hypoplasia is a common dentofacial deformity in patients with cleft lip and palate (CLP). During growth and at the time of facial maturity, patients commonly develop class III malocclusion, a concave facial profile with a retruded midface, and a narrow maxillary arch. Class III malocclusion in patients with CLP may result in impairment of the patient’s speech, mastication, lip function, swallowing, breathing, and facial esthetics. Approximately 48% to 65% of patients with a cleft require orthognathic surgery at skeletal maturity, although the reported percentage is variable and ranges from 14% to 75%. ,
Before the successful clinical application of craniofacial distraction, maxillary advancement (Le Fort I) with fixation was the mainstay surgical treatment of lower midface retrusion. Currently, conventional orthognathic surgery with fixation, Le Fort I distraction, or a combination of the two are the surgical modalities commonly used for the treatment of maxillary hypoplasia in patients with a cleft. The use of craniofacial skeleton distraction osteogenesis (DO) has significantly expanded since the initial clinical report by McCarthy and coworkers, who successfully elongated the hypoplastic mandible of a patient with hemifacial microsomia. A plethora of clinical and basic science reports have validated McCarthy and coworkers innovative work on craniofacial DO and long-term studies have confirmed the ability to obtain a successful and a stable maxillary advancement through maxillary distraction.
Maxillary advancement with fixation versus maxillary distraction
Le Fort I maxillary advancement with plate fixation is the preferred single-step treatment of maxillary hypoplasia. When deciding between traditional Le Fort I advancement and fixation and Le Fort I distraction for correction of class III occlusion, the magnitude of anterior/posterior (AP) maxillary movement must be considered, especially in patients with CLP. Patients with CLP present a unique challenge to the orthodontist and orthognathic surgeon. The surgical repair of the CLP produces dense scar tissue formation in the surgically treated areas, which contributes to a tight soft tissue envelope against which the maxilla is advanced. In addition, the presence of prior midface surgery, such as Le Fort I or III advancement and surgically assisted rapid palatal expansion, increases the difficulty advancing the maxilla. Additionally, any pharyngeal surgery for velopharyngeal insufficiency (sphincter pharyngoplasty and pharyngeal flap) performed in patients with a cleft invariably results in scar tissue formation at the posterior aspect of the palate. This has been demonstrated to increase the difficulty in reliably advancing the maxilla more than 6 to 7 mm. One of the advantages of maxillary DO is in its ability to slowly stretch the soft tissue envelope during skeletal advancement. The most frequent use of maxillary DO at the Le Fort I level is the sagittal (anterior) advancement of the maxilla to overcome these restrictive forces. This gradual expansion of the soft tissues and soft tissue histogenesis allows for a greater stability of the skeletal advancement and a superior esthetic result.
There is a known incidence of maxillary AP relapse following conventional Le Fort I advancement and fixation. Maxillary advancement greater than 10 mm has been demonstrated to have a higher rate of relapse especially in patients with CLP. Multiple reports in this patient population have confirmed a direct association between the degree of AP maxillary advancement and the degree of midfacial relapse, with a wide reported incidence of 10% to 50%. , , , The higher rate of AP maxillary relapse in patients with CLP is multifactorial and has been attributed to: excessive scar tissue, limited blood supply, more complex maxillomandibular deformity, and poor bone quality.
At our institution we reviewed our experience treating patients with or without CLP who underwent Le Fort I maxillary advancement. Our data revealed that the average maxillary advancement for all patients without distraction was 6.3 mm with a corresponding AP relapse of 1.8 mm, indicating a 28.6% relapse. A history of cleft and the magnitude of maxillary advancement were directly correlated with increased skeletal relapse, whereas bone graft at the osteotomy site demonstrated a protective effect on relapse. Our results revealed that patients with cleft have an average of 1.25 mm greater AP relapse when compared with patients without cleft. Our findings also demonstrated that each additional millimeter in maxillary advancement was associated with an additional 0.298 mm of relapse. The degree of relapse was not associated with cleft phenotype (unilateral CLP, bilateral CLP, and isolated cleft palate). Other studies have echoed our findings, specifically Cheung and colleagues, who demonstrated AP plane relapse rate of 22% and 22.5% in patients with a unilateral and bilateral cleft.
In the era preceding DO, patients with class III malocclusion secondary to maxillary hypoplasia necessitating a maxillary advancement of more than 10 mm frequently underwent a bimaxillary surgery (Le Fort I with advancement and bilateral sagittal split osteotomy with mandibular setback). This manipulation of the maxilla and mandible worked to “split the difference” in the negative overjet, therefore avoiding a large maxillary advancement and its associated high rate of relapse. When this approach is followed, maxillary advancement is limited to less than 10 mm of AP advancement and the remaining difference, if any, is addressed via mandibular setback. Alternatives to splitting the difference (two jaw surgeries) include maxillary advancement via DO. This is usually performed in patients with a cleft requiring AP maxillary advancement greater than 10 mm. Maxillary distraction in these situations has been associated with a far lower relapse rate.
External versus internal (semiburied) distraction device
Currently, two main surgical approaches exist for maxillary DO: internal distraction using subcutaneously placed distraction devices, and external (halo) distraction device with cranial fixation. , The rigid external distraction (RED) device was the first external distractor used for midface DO and is still used today to translate the maxilla and midface. The RED device requires concurrent use of a cranial halo that is secured to the skull with pins ( Fig. 1 A). The halo is attached to a midline vertical bar, which has mobile horizontal bars that can move along (up and down) the length of the vertical bar to provide anchorage for the wires that are attached to the distractor plates or orthodontic anchors ( Fig. 1 A,B). ,
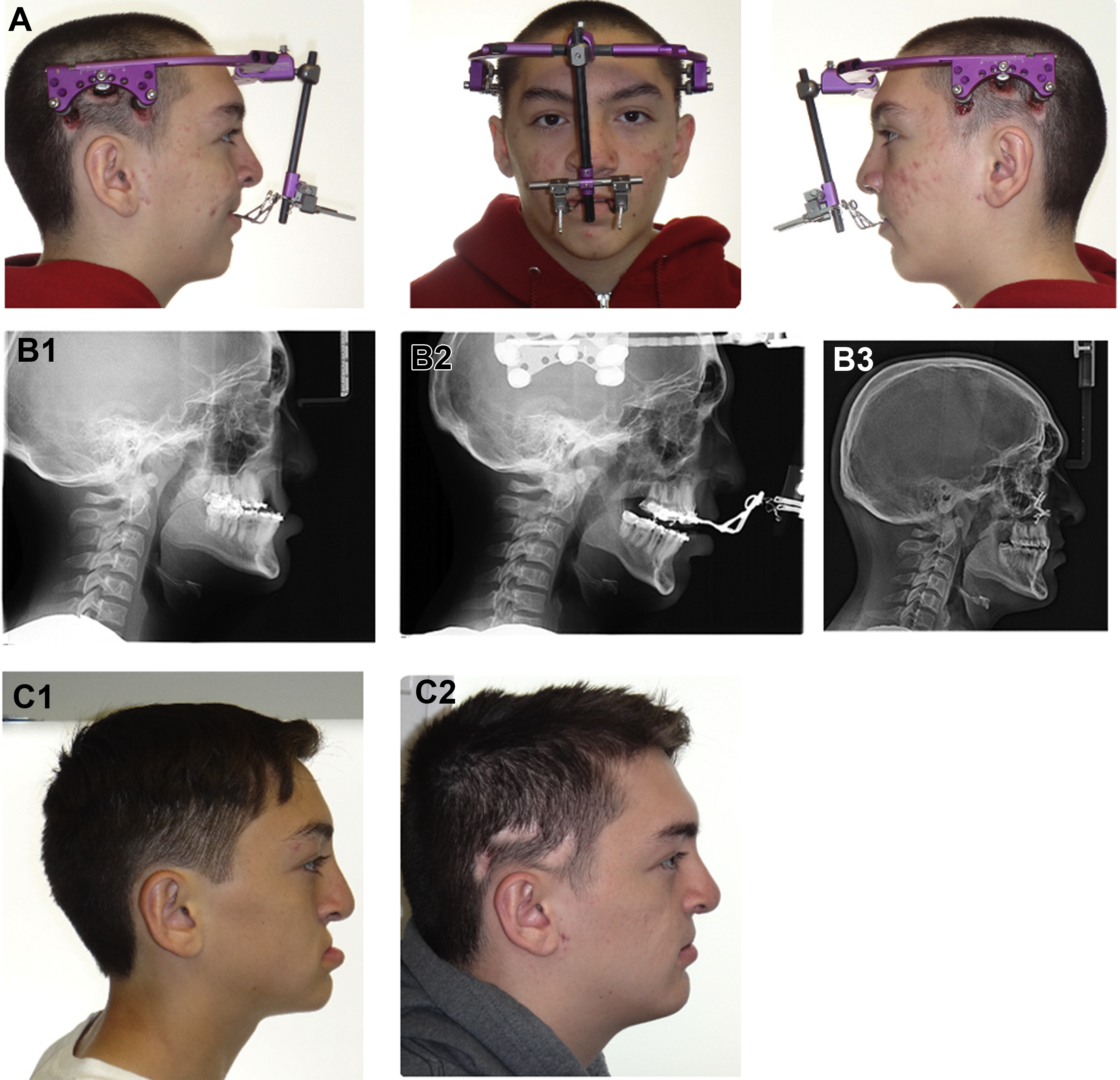
The main advantage of using a RED device is the ability to change the vector along multiple vectors of distraction during the activation phase and (theoretically) unlimited distraction length. Additional advantages include the ease of use and relative ease of device removal after completion of consolidation. Despite the previously mentioned advantages, the RED device has several risks, such as site infection, device dislodgement, intracranial pin migration, pin site alopecia ( Fig. 1 C), and susceptibility to trauma. Moreover, wearing a RED device for 8 to 12 weeks is cumbersome and it is difficult to wear in school or in public. These limitations led to the development of internal (semiburied) maxillary distraction devices.
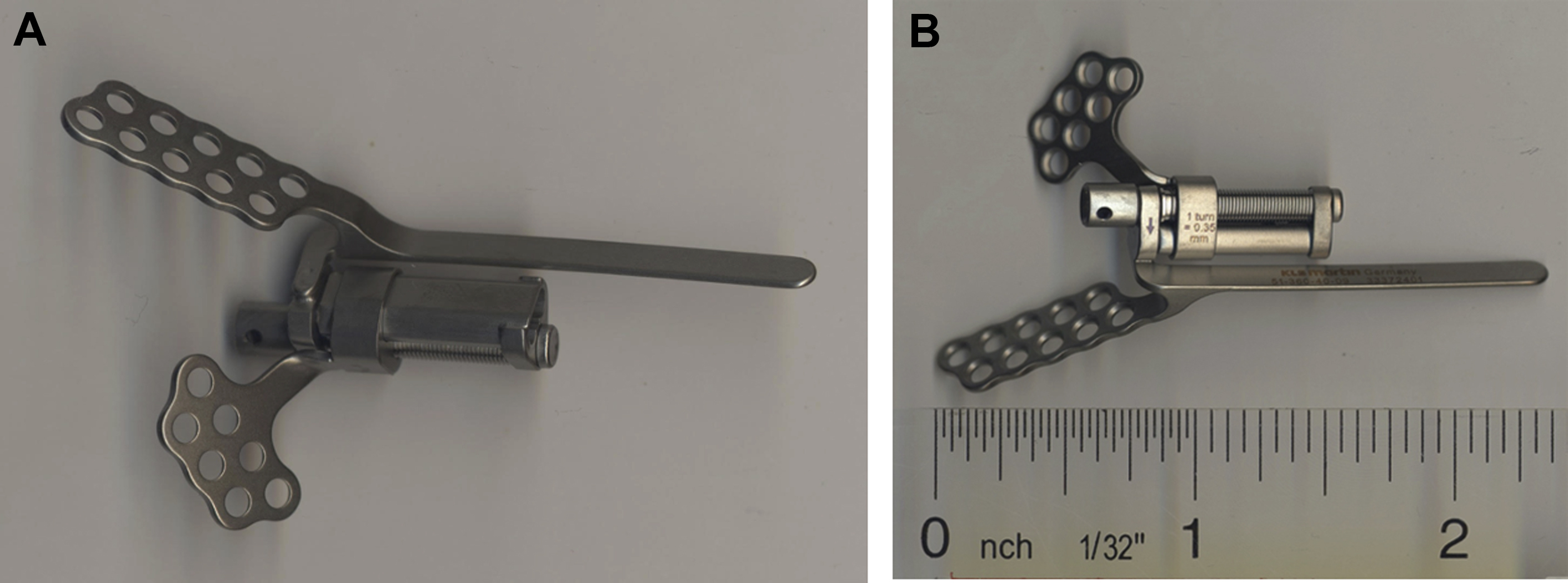
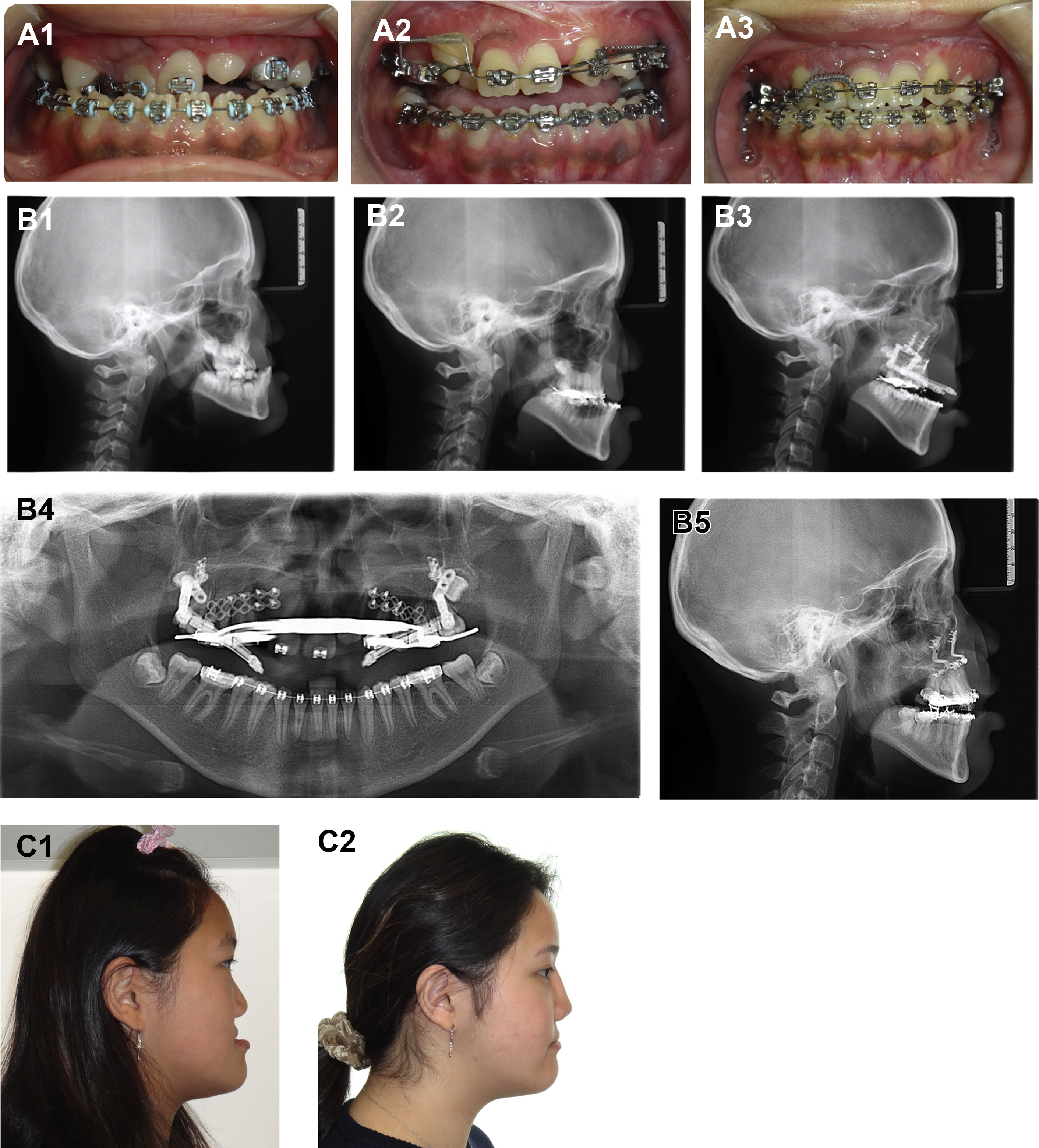
In 1995, Cohen and colleagues , reported on the use of DO to advance the maxilla using internal devices in humans. Internal distraction devices have the advantage of reducing the amount of physical and psychological stress placed on patients, families, and caregivers. These internal distractors are more socially acceptable and allow earlier return to work and easier socialization. Internal distractors were initially limited by the size of the lengthening screws to advance the maxilla and the stability of the devices as they are lengthened. The advent of the telescoping lengthening screws has compensated for this problem ( Fig. 2 ). Some of the challenges of the internal distractor devices include: difficulty in placing the right and left devices within symmetric and parallel vectors of distraction, inability to adjust the unidirectional vector of distraction during the activation phase, discomfort related to the stretch of the buccal tissues by the distractor rods, and the need for a second operation for hardware removal after the consolidation phase is complete. Although the most frequently cited drawback of internal distractors is the inability to adjust the vector of distraction during activation, vector control with midface distractors is successfully achieved via simultaneous placement of microimplant anchored class III relationship elastics. Additionally, as a result of this limitation, internal distraction for our institution often functions to advance the maxilla to a location that makes the final advancement and rigid fixation during a secondary surgery more feasible and stable rather than provide the entire movement required to achieve occlusion. Despite the previously described limitations we have had success achieving significant advancement and correction of class III occlusion using internal distraction devices ( Fig. 3 ).
Patient evaluation
All patients should be evaluated by a multidisciplinary team consisting of a speech pathologist, social worker, dietician, anesthesiologist, orthodontist, and a surgeon. Compliance and the ability of the patients and parents to tolerate a complex distraction protocol should be thoroughly assessed before initiation of treatment. Any degree of velopharyngeal incompetence (VPI) is evaluated and accurately documented before operation. With the speech pathologist’s input, patients with VPI are informed that their VPI will either remain unaffected or, most likely, get worse after completion of distraction. Interval speech evaluation after completion of distraction functions to evaluate the “new baseline” speech function.
Preoperative and postoperative nutritional consultation is also important for discussing dietary strategies for maintaining optimum and balanced caloric intake during the distraction process for ideal wound healing. All patients are informed of the need to adhere to a soft diet throughout the distraction process.
Evaluation by an experienced anesthesiologist helps to identify potential difficulties during administration of anesthesia. Nasotracheal intubation is particularly challenging in patients with choanal stenosis/atresia, turbinate hypertrophy, or septal deviation. The presence of previous pharyngeal flap or sphincter pharyngoplasty can add to the difficulty of nasotracheal intubation.
Orthodontic considerations and surgical planning
Early and active involvement of the orthodontist, frequent and serial evaluation, and close communication between the orthodontist and surgeon are crucial to executing a successful treatment plan. Predistraction orthodontics, orthodontic manipulation during the activation and consolidation phases, and postdistraction orthodontic management are all phases to be considered when planning maxillary distraction (see Fig. 3 A1–A3). ,
The goal of Le Fort I distraction is the restoration of class I occlusion. The final position of the maxilla required to restore occlusion is determined by the orthodontic and surgical team. A treatment plan for orthodontic preparation with the goals of leveling, aligning, and coordinating the maxillary and mandibular arches is crafted by the orthodontic team executed with close clinical follow-up. Determining the final position of the maxilla and final occlusion is done with a combination of physical examination, dental models, photographs, three-dimensional computed tomographic imaging, and cephalometric analysis. Continuity of the maxillary arch should be ensured before performing maxillary distraction. Alveolar clefts, when present, should be reconstructed with bone graft and the continuity of the maxillary arch confirmed clinically and radiographically before maxillary distraction. The presence of an alveolar cleft or unidentified fracture through the grafted site can lead to an unstable maxilla (two-piece maxilla with separation at the cleft site) during osteotomy and device activation.
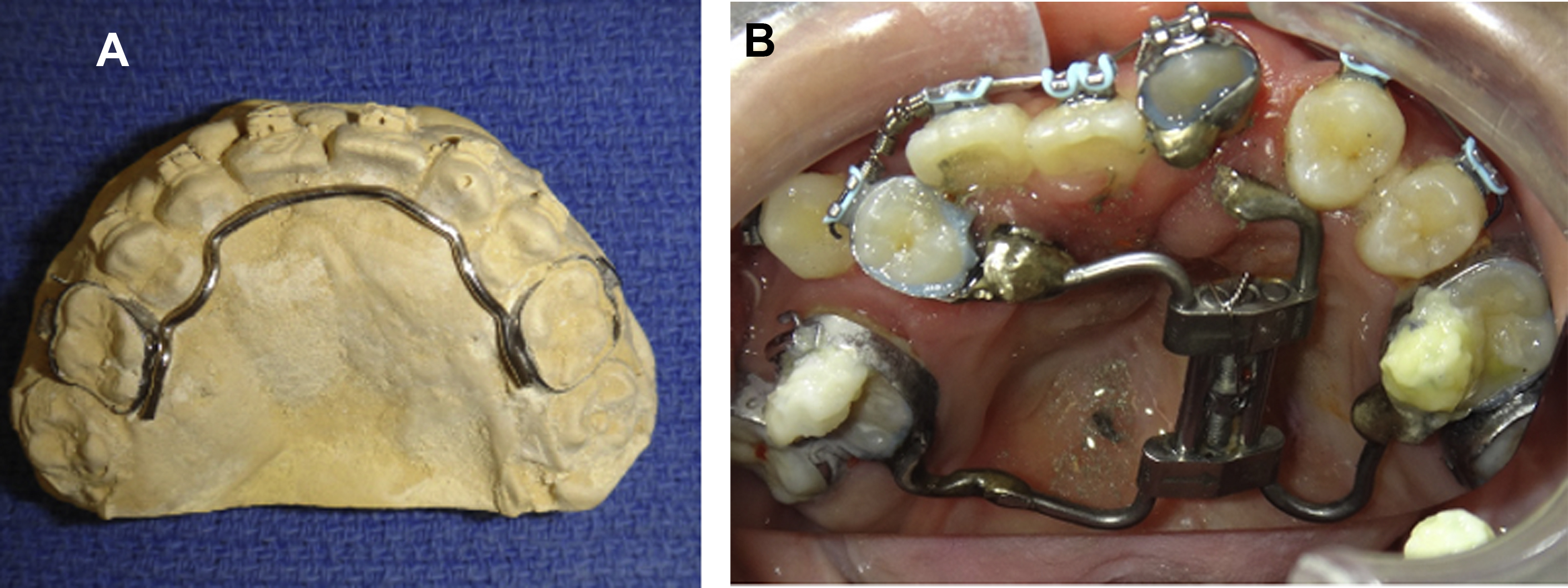
When using internal distractors, the importance of advancing the maxilla as a single piece cannot be overemphasized. It should also be remembered that the maxilla is wider posteriorly and application of internal distractors and subsequent activation invariably leads to collapse and compression of the two unstable maxillary segments as the two segments advance anteriorly and medially. A transpalatal support bar or palatal expander should be used during maxillary distraction because it helps reduce the chance of bone separation at the site of the cleft and can also keep the two maxillary segments stable in the event of unwanted bone separation at the alveolar cleft site ( Fig. 4 ). Even if fracture across the grafted alveolus does not occur during surgery, fracture can occur during activation because the bone stock at the site of the grafted alveolus may not be strong enough to withstand the distraction forces.