Nerve substitution is an important tool in facial reanimation. The goal is to reinnervate the distal facial nerve and musculature using an alternative cranial nerve in order to achieve facial movement, symmetry, and tone. Multiple donor nerves have been used for nerve transfer procedures, the most common being hypoglossal, masseteric, and cross-facial nerve graft. Each donor nerve has its advantages and disadvantages. Multiinnervation uses the use of multiple donor nerves in order to leverage the benefits while balancing the pitfalls of each nerve. The nerve transfer depends on the type of nerve injury, time since injury, and patient factors.
Key points
- •
This article reviews the different types of nerve substitution, their indications, and the pros and cons of each.
- •
The goal of nerve substitution is to restore dynamic and mimetic facial motion as well as resting facial tone and symmetry.
- •
Multiinnervation allows donor nerves to complement one another and avoid pitfalls inherent to individual donor nerves.
Video content accompanies this article at http://www.facialplastic.theclinics.com .
Introduction
Nerve substitution is the preferred treatment of facial nerve injury when primary neurorrhaphy or cable grafting is not feasible. Nerve transfers are indicated when the proximal end of the facial nerve cannot be grafted but the distal nerve branches and facial muscles are viable. The ideal timing of neurotization surgery is within 2 years of facial nerve injury, as this has shown the most predictable results.
Multiple cranial nerves have been used for nerve substitution; however, none can guarantee complete facial nerve recovery or restoration of normal facial function. The unpredictability of facial nerve outcomes lies in the complex nature of peripheral nerve regeneration and reinnervation. The ideal donor nerve depends on the type of nerve injury, time since injury, and patient factors. Nerve transfers can be used for direct motor neurotization, babysitter and double innervation techniques, and innervation of neuromuscular transplants. The most common nerve substitution procedures are discussed in this article.
Nerve substitution for treatment of facial paralysis
Hypoglossal-Facial Nerve Transfer
The hypoglossal-facial nerve transfer was first introduced in 1901 by Korte and became widely popularized by Conley and Baker. Initially, hypoglossal-facial nerve transfer involved complete transection of hypoglossal with end-to-end coaptation to the distal facial nerve. However, this resulted in unacceptable outcomes including functional deficits of speech, mastication, and swallowing, as well as hemifacial mass activation and synkinesis.
The procedure has since undergone multiple modifications to minimize morbidity. In 1991, May and colleagues reported a technique of partial sacrifice of the hypoglossal nerve and end-to-side coaptation using an interposition graft. This technique maintained functional results while decreasing mass movement, synkinesis, and deficits of speech and mastication. Cusimano reported longitudinal splitting of the hypoglossal nerve to preserve continuity to the tongue. Slattery and colleagues described transposition of the intratemporal facial nerve with end-to-side coaptation, eliminating the need for an interposition graft.
Surgical technique
The senior author uses the technique of end-to-side coaptation with transposition of the intratemporal facial nerve. The procedure is performed through modified Blair parotidectomy incision. The main trunk of the facial nerve is identified using standard landmarks, and with assistance from an otology colleague, the facial nerve is transected at the geniculate ganglion and transposed inferiorly. The hypoglossal nerve is identified deep to the posterior belly of the digastric muscle and followed distally to the branching of the descendens hypoglossi. An incision is made in the hypoglossal nerve through 40% to 50% of its diameter, and the facial nerve is coapted end-to-side to the hypoglossal nerve. If extra length from the mastoid drill-out is not attainable, a cable graft using the greater auricular nerve may be used, although the senior author prefers direct coaptation by mobilizing the hypoglossal nerve superiorly with transection of the ansa if needed and performing direct coaptation very high proximally on the hypoglossal nerve at the level of transverse process of the second cervical spine. This avoids axonal loss from additional coaptation sites.
Advantages
- •
Large motor nerve with similar caliber to facial nerve
- •
Close proximity to facial nerve
- •
Restores facial tone
- •
Able to achieve voluntary smile with neuromuscular retraining
Disadvantages
- •
Unable to restore spontaneous mimetic function
- •
Neuromuscular retraining is necessary to simulate smile
- •
Potential for hemitongue atrophy, speech and mastication deficits, mass activation, and synkinesis with sacrifice of more than 50% of hypoglossal nerve
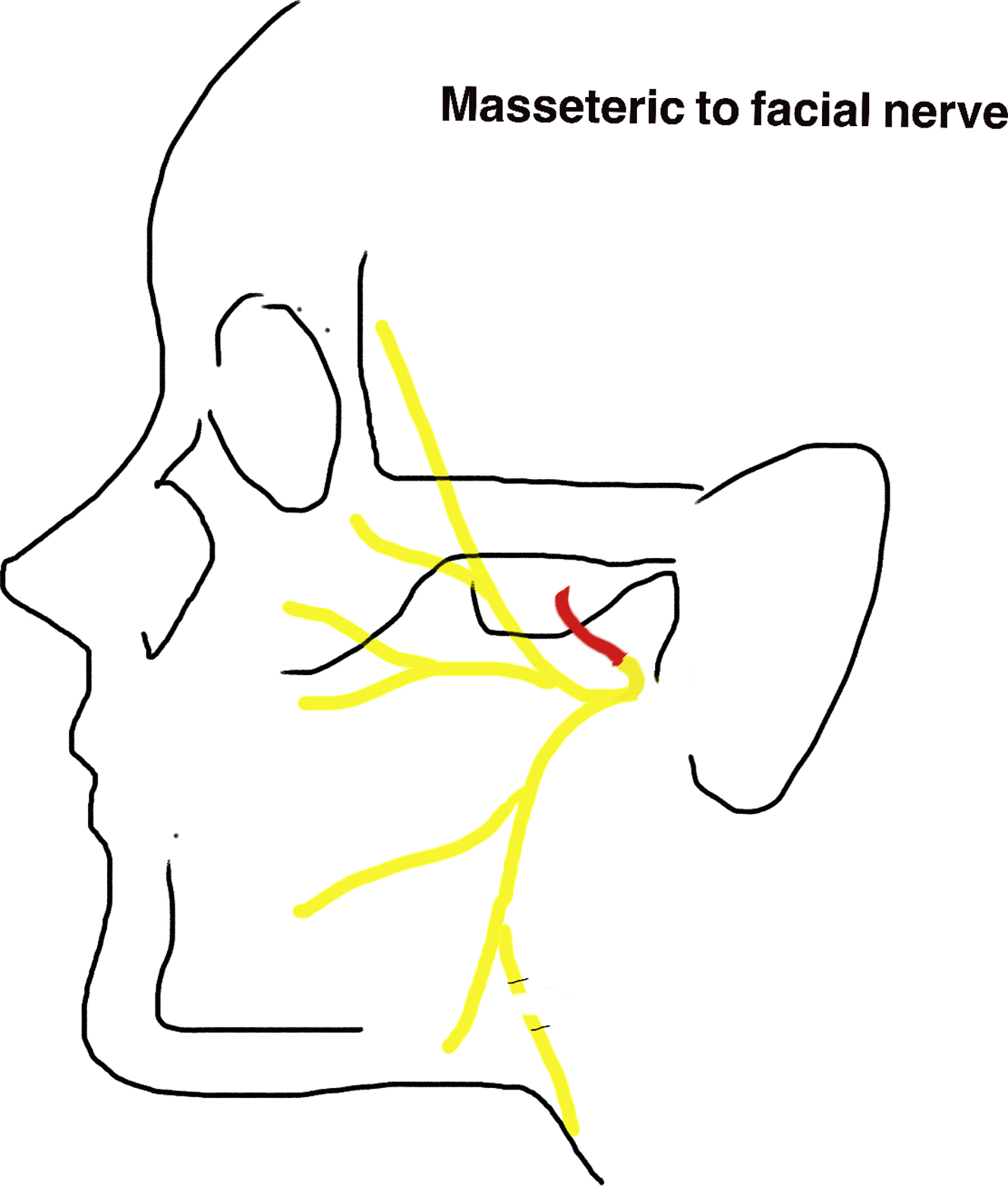
Masseteric-Facial Nerve Transfer
In 1978, Spira introduced masseteric-facial nerve transfer for facial reanimation ( Fig. 1 ). This procedure became a popular donor nerve due to its proximity, ease of dissection, length and caliber, minimal donor morbidity, and rapid functional recovery. The masseteric nerve has more than 1500 axons, which is a sufficient number to power the main trunk and produce reliable and powerful oral commissure excursion. The masseteric nerve has also demonstrated significantly faster clinical recovery compared with the hypoglossal.
The main critiques of this donor nerve are inability to recover mimetic function and poor facial tone in repose. , The absence of resting facial tone is most notable during speech, when the patient is unable to activate their masseter. Restoration of resting tone is important from both an aesthetic and a functional standpoint. Aesthetically, facial symmetry is only obtained with masseteric activation, whereas at rest there is obvious asymmetry between the 2 sides. From a functional standpoint, loss of facial tone has significant consequences for the eye and midface. Loss of orbicularis oculi tone and gravitational pull of the midface can cause paralytic ectropion, which can result in inadequate eyelid closure, exposure keratopathy, corneal ulceration, and blindness if not treated. Difficulties in mastication and speech are consequences of loss of buccinator tone. To address these shortfalls, the authors integrate static procedures with masseteric nerve transfer.
Surgical technique
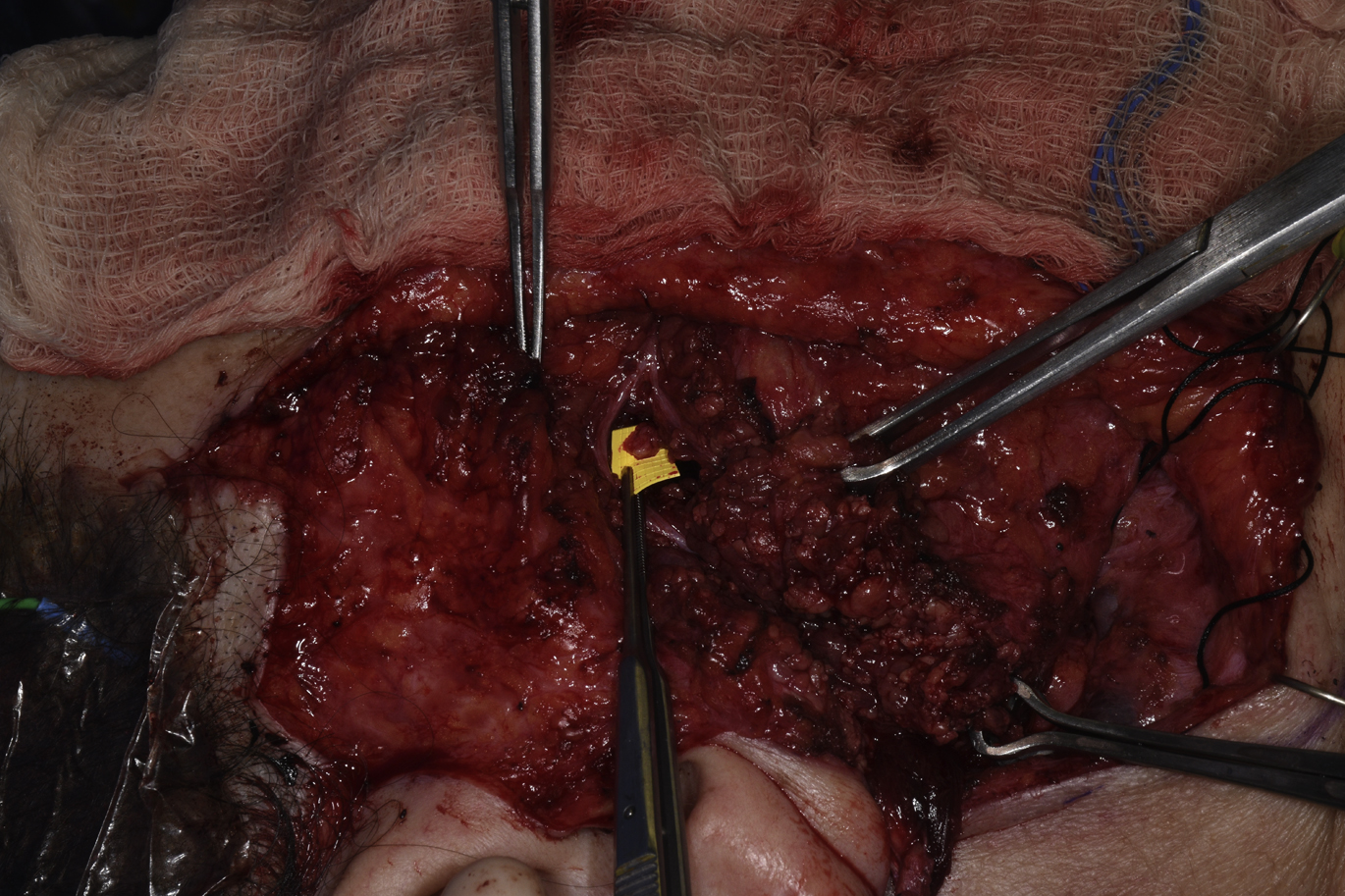
Through a preauricular incision, a cheek flap is elevated just over the parotidomasseteric fascia anterior to the anterior border of the masseter muscle. The parotid fascia is incised to identify buccal branches that are dissected retrograde. Facial nerve branches superior and inferior to the point of entry are identified and protected. Dissection can begin at a point 1 cm below the zygomatic arch and 3 cm anterior to the tragus. Another approach to localize the nerve is the subzygomatic triangle, which is formed by the zygomatic arch, frontal branch of the facial nerve, and a perpendicular line through the temporomandibular joint. The nerve travels along the deep part of the masseter muscle about 1.0 to 1.5 cm deep to the parotidomasseteric fascia. The nerve is traced distally and can be followed after it branches, including these branches in order to obtain as much length as possible ( Fig. 2 ). The dissection is often bloody, which can make identification of the nerve difficult. Ways to identify the nerve if one is having difficulty is to use microcottonoids moistened with 1:1000 epinephrine to limit bleeding or to use nerve stimulator when in close proximity. Once the nerve is transected, it is coapted end-to-end to the main trunk or lower division of the facial nerve. Vein grafts are used to ensheath neurorraphies.
Advantages
- •
Large motor nerve with more than 1500 axons
- •
Close proximity to facial nerve facilitates direct coaptation
- •
Faster clinical recovery compared with hypoglossal nerve
- •
Minimal donor morbidity
Disadvantages
- •
Unable to restore spontaneous mimetic function
- •
Does not restore resting facial muscle tone
- •
Neuromuscular retraining is necessary to simulate smile
Masseteric-Facial, Cable Nerve Graft
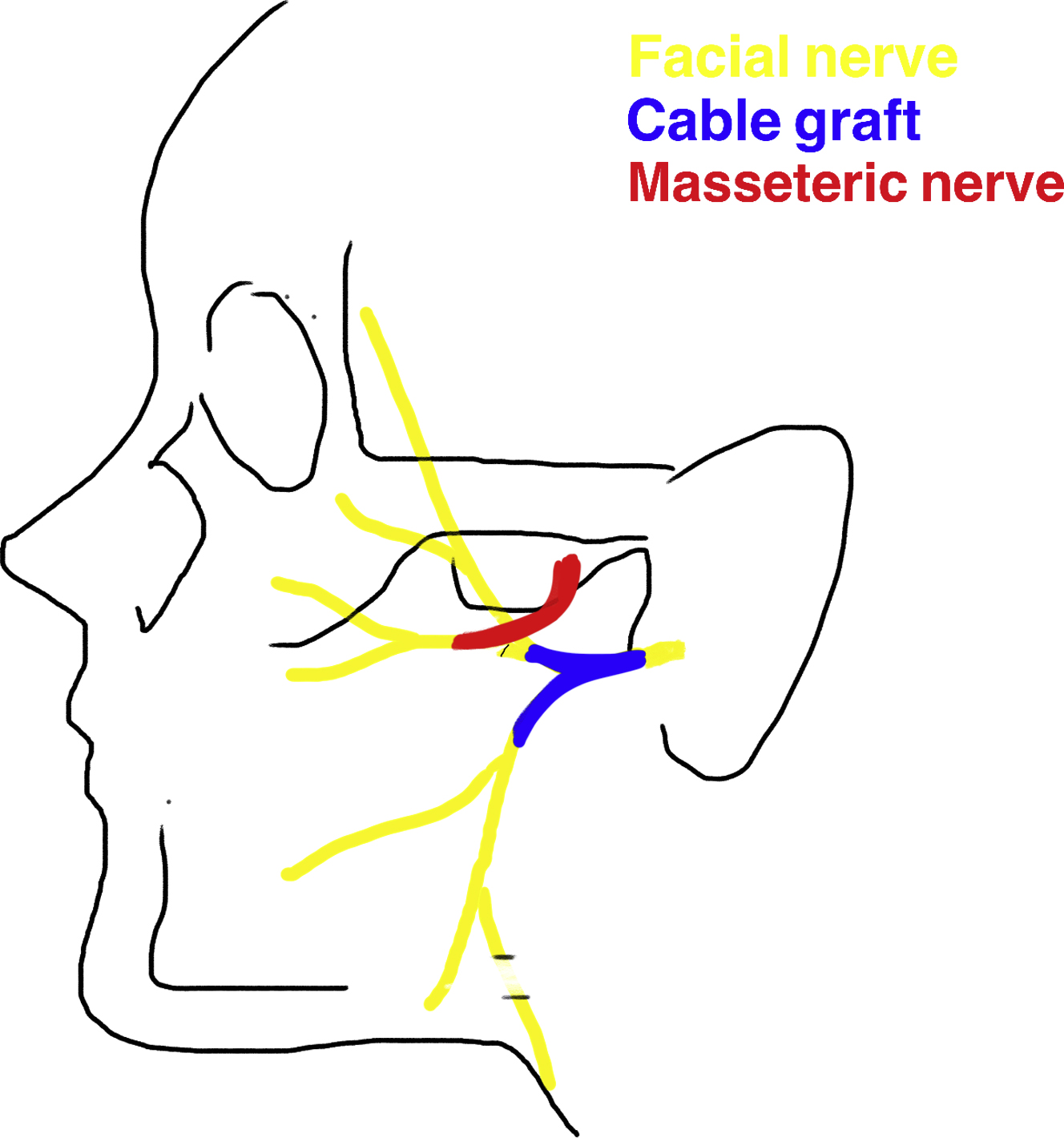
Nerve substitution can also be used as an adjunct to facial nerve repair. Cable grafting of the facial nerve is performed when primary neurorrhaphy is not feasible. Expected recovery after cable grafting is about 6 to 12 months; however, this may vary depending on the preoperative facial nerve function. Owusu and colleagues reported favorable outcomes with combining masseteric nerve transfer with facial nerve cable grafting ( Fig. 3 ). They demonstrated fast return of oral commissure movement and decreased synkinesis. The addition of masseteric nerve transfer to cable grafting augments results through powering strong oral commissure excursion and providing neural input while awaiting nerve regeneration through the cable graft.
Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Modified Selective Neurectomy
Modified Selective Neurectomy
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Dual Nerve Transfer for Facial Reanimation
Dual Nerve Transfer for Facial Reanimation
 Treating Nasal Valve Collapse in Facial Paralysis
Treating Nasal Valve Collapse in Facial Paralysis
 Facial Reanimation and Reconstruction of the Radical Parotidectomy
Facial Reanimation and Reconstruction of the Radical Parotidectomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


