Key points
• The deleterious effects of ionizing radiation are cumulative, necessitating the judicious use of ionizing radiation.
• Cone beam CT (CBCT) allows for image capture that displays excellent spatial resolution (image detail) of hard tissue at a relatively low dose of ionizing radiation.
• CBCT data sets can be integrated with task specific diagnostic software programs such as virtual surgical planning.
• A radiation reduction approaching 90% can be achieved with CBCT compared with traditional CT.
• With CBCT the patient is either standing upright or seated. This allows for a reproducible head posture to be established and duplicated when sequential scans of the facial complex are indicated.
• Injectable contrast media to highlight vascular tissue, enhance lymph node visibility or outline anatomic boundaries is not clinically feasible with CBCT at this time.
• MRI can distinguish blood vessels and nerves from surrounding soft tissue. This type of anatomical differentiation is far superior to that with other imaging modalities and constitutes the principal benefit of an MR study.
• Bony structures, which contain less water and consequently less available hydrogen protons for imaging, are not welldefined by MR. CT and CBCT remain the state of the art when evaluating these structures.
Introduction
The information gained from an imaging study is called the “diagnostic yield.” The higher the diagnostic yield, the more information the clinician receives about his or her patient. However, the information gained must be of clinical relevance to the surgeon. It must provide answers to diagnostic questions that allow the surgeon to better understand the anatomic relationships under consideration.
The invention of computed tomography (CT) in the 1970s gave birth to a new era in diagnostic imaging. No longer were clinicians restricted to projection radiology (PR), with its distortion, superimposition, and two-dimensional (2D) representation of the patient’s three-dimensional (3D) facial anatomy.
The worldwide acceptance and dependence on CT redefined the state of the art for preoperative diagnostic analysis and image-guided surgery. Ongoing development and refinement of sensors and software drove CT to become the de facto standard of care in maxillofacial imaging.
A decade later magnetic resonance imaging (MRI) supplemented the information gained from a CT examination by providing exceptional visualization of soft tissue. When indicated, the coupling of these two imaging systems provides unprecedented visualization of anatomic structures and pathologic conditions.
The dawn of the twenty-first century saw an additional imaging system, cone beam computed tomography (CBCT), establish its place as a 3D imaging alternative that compliments and, in some respects, surpasses CT.
This chapter outlines the advantages and limitations of CT and CBCT and places MRI in perspective so that the surgeon can appreciate, prescribe, evaluate, and integrate the information gained from an imaging study. Comparison of these advanced imaging modalities in terms of diagnostic yield and radiation burden to the patient are presented so the specialist can optimize every relevant diagnostic tool and achieve the most aesthetically superior surgical outcomes.
Clinically relevant radiation biology
Traditional projection imaging (lateral cephalometric, skull and panoramic studies) as well as CT and CBCT utilize ionizing radiation to create an image. MRI does not. MRI utilizes a combination of radiofrequency (RF) waves and magnetism to manipulate hydrogen protons within the body and generate an image. To date, there are no scientifically documented harmful biologic effects from the clinical utilization of MRI.
Ionizing radiation, also called x-rays, is a form of electromagnetic energy that has a wavelength of approximately a millionth of a millimeter. By comparison, television waves, also a form of electromagnetic radiation, have a wavelength of approximately two meters while radiowaves have a wavelength of 100 meters. The smaller the wavelength, the more powerful is the radiation. The infinitesimal wavelength associated with x-rays makes them powerful enough to harm living tissue.
Two distinct reactions caused by x-rays contribute to the damage/risk they inflict on our patients. One reaction, called direct effect of ionizing radiation, takes place when an x-ray collides directly with a macromolecule and fragments one of the molecular bonds. Altered structure and function of the macromolecule may result. Additionally, when the molecular damage involves reproductive tissue, the deleterious effects can be passed on to future generations. The second reaction, called indirect effect of ionizing radiation, occurs when an x-ray collides with a molecule of water and splits it into two reactive ions: H* and OH*. These ions may result in the formation of H 2 O 2 (hydrogen peroxide), which can result in damage to the intracellular environment.
While the body possesses the power to mend some of the damage caused by ionizing radiation, current theory states that complete healing never occurs. That fact, coupled with the principle that the deleterious effects of ionizing radiation are cumulative, necessitates judicious use of ionizing radiation. Minimizing the patient’s lifetime exposure to x-rays is a professional mandate.
Prescribing an imaging study
Based on the clinical examination, medical history and treatment objectives the surgeon decides what, if any, imaging study is essential for a given patient. This is a professional judgment founded on prevailing evidenced-based best practices. Once the decision to image has been made, strict adherence to the concept of As Low As Reasonably Achievable (ALARA) is essential. ALARA is often misinterpreted as a guideline on when a patient should be imaged. As stated above, the decision on when a patient should be imaged lies within the professional judgment of the surgeon. What ALARA dictates is that once the decision is made that imaging is indicated, the clinician prescribes an imaging study that will provide the required diagnostic yield and, at the same time, subject the patient to the lowest amount of ionizing radiation possible. Inherent in the concept of ALARA is that the clinician limit the field of view to the anatomic area under consideration. Another concept embraced by ALARA is that the patient has adequate shielding during the imaging procedure. Having x-ray machines properly calibrated, avoiding repeat examinations when possible, and utilizing imaging equipment with the lowest possible dose to the patient are all encompassed in ALARA.
Two-dimensional images: Applications to contemporary aesthetic surgery of the facial skeleton
Projection radiology has been used for over a century to provide relatively reliable diagnostic information. In PR, the patient is placed between the x-ray source and the imaging receptor. Selective absorption (attenuation) of the x-ray beam as it passes through the patient creates a pattern that reflects the various anatomic structures under examination. In general, the thicker and denser the anatomic structure being imaged, the more x-rays it will attenuate. Areas of high attenuation (bone and surgical fixation hardware) result in a relatively white (radiopaque) impression within the final image. Areas of low attenuation (soft tissue and the paranasal sinuses) result in a radiolucent (black) presentation.
Fig. 7.1 illustrates three common types of projection images that remain relevant to present-day facial surgery: lateral cephalometric, posterior-anterior (PA), and panoramic projections. In generic terms, the lateral cephalometric image demonstrates the relative osseous relationship of the mandible to the maxilla and the maxilla to the craniofacial base. The PA skull view gives an indication of relative facial height and symmetry from the frontal perspective while the panoramic projection presents a partial overview of the osseous structures within the oral and maxillofacial complex.
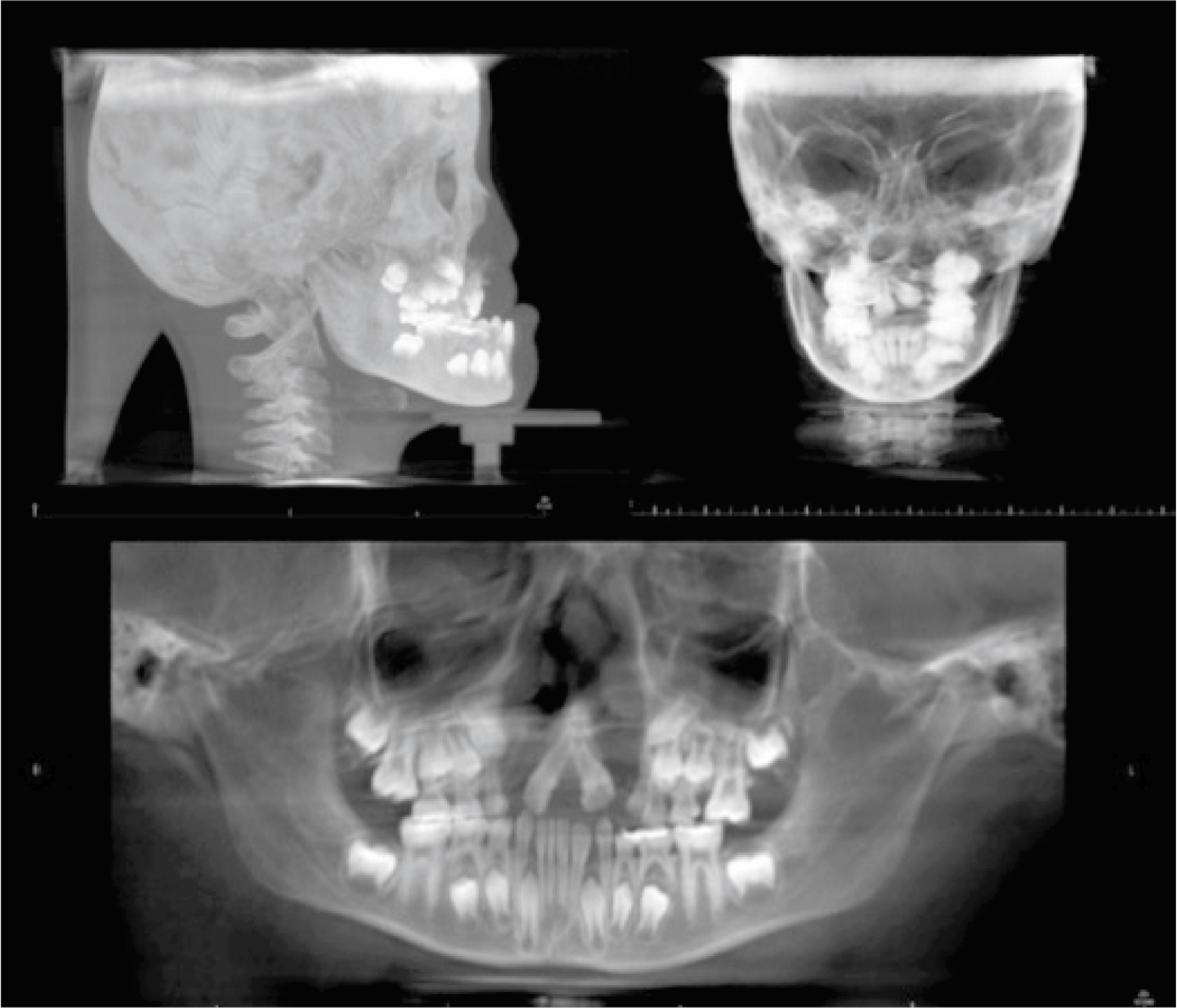
The lateral cephalometric image, like all PR studies, is compromised due to inherent magnification, distortion, and overlap of adjacent structures. It does, however, provide baseline osseous relationships relevant to treatment planning for aesthetic facial surgery and related orthognathic procedures. Image filtering allows for portrayal of the soft tissue profile. With its ease of acquisition, relatively low radiation dose and long history of clinical utilization, the lateral cephalometric projection remains a relevant image for initial patient evaluation and surgical follow-up. Conditions such as prognathia and anterior-posterior (AP) osseous deficiency of the maxilla can be generically categorized with the lateral cephalometric image.
The PA projection can be utilized to display relative osseous symmetry in the coronal plane. Hemifacial microsmia as well as mandibular asymmetry caused by unilateral temporomandibular joint (TMJ) condylar hyperplasia are clinical examples of situations where the PA projection can offer anatomic insight.
Panoramic radiology is a maxillofacial imaging system that utilizes a coordinated movement of the radiation source and an image receptor to create a relatively clear zone or layer of anatomy, including the jaws and surrounding structures. The panoramic image suffers from distortion and structural overlap, but its ease of acquisition, low radiation dose, and relative clarity make it an invaluable addition to the maxillofacial imaging armamentarium. Its anatomic coverage includes the osseous structures of the mandible, the maxilla inferior to the orbit, the external auditory meatus, and the zygomatic process of the temporal bone. It provides an osseous overview of the lower face. While panoramic radiology has diagnostic strengths in portraying the body of the maxilla and the mandible, it can be inherently misleading in the midmaxilla and TMJ regions due to overlapping of the cervical spine and the temporal bone, respectively.
Several previously used skull projections have been replaced by modern cross-sectional imaging. These include the Waters projection for portrayal of the maxillary sinus, the Caldwell Projection for evaluation of the orbits, the lateral jaw projection for imaging the body of the mandible, the AP projection for imaging the occipital bone, and the reverse Towne projection for evaluating the TMJ complex.
Despite its limitations, projection radiology is relatively low in radiation dose, technically straightforward, patient-friendly, and a financially attractive means of acquiring structural anatomic relationships. It can provide baseline osseous relationships relevant to the initial treatment planning of aesthetic facial surgery and related orthognathic procedures. Additionally, because PR does not suffer from the streaking artifact associated with tomographic imaging systems, these views are often well suited for postsurgical radiographic evaluation.
When a higher diagnostic yield is necessary, a tomographic (cross-sectional) imaging system can provide undistorted images without the drawback of anatomic superimposition.
The increased radiation dose to the patient (the radiation burden) from a cross-sectional imaging system requires a heightened risk-benefit analysis before the study is prescribed. Often termed “advanced imaging,” these cross-sectional systems include CT and the more recently developed CBCT. The clinical applications, advantages, and disadvantages of each of these advanced imaging modalities will now be considered. An evaluation of MRI, which does not use ionizing radiation, will follow.
Computed tomography
Invented in 1972 by Godfrey Hounsfield at EMI Institute in London, England, computed tomography (also known by the misnomer “CAT scan,” for computed axial tomography) has revolutionized diagnostic radiology. Like PR, CT uses ionizing radiation that is selectively absorbed as it traverses the body. The pattern formed by the x-ray beam after it exits the patient is captured by a series of detectors. How CT differs from PR is that as the x-ray source turns or revolves around the patient the detectors capture snapshots or profiles of the attenuated x-ray beam. The profiles are sent to a computer, which uses algorithms to generate slices of the internal anatomy captured in the area of interest (also called field of view ). Early clinical CT machines would generate a thin, fan-shaped x-ray beam that would revolve around a movable patient bed (the gantry). The gantry would incrementally move the patient as the x-ray beam would slice or knife its way through the anatomic area of interest. A set of ring-like detectors synchronized with the x-ray beam captured the attenuated radiation pattern as it left the patient and fed the data to a computer for image reconstruction and display.
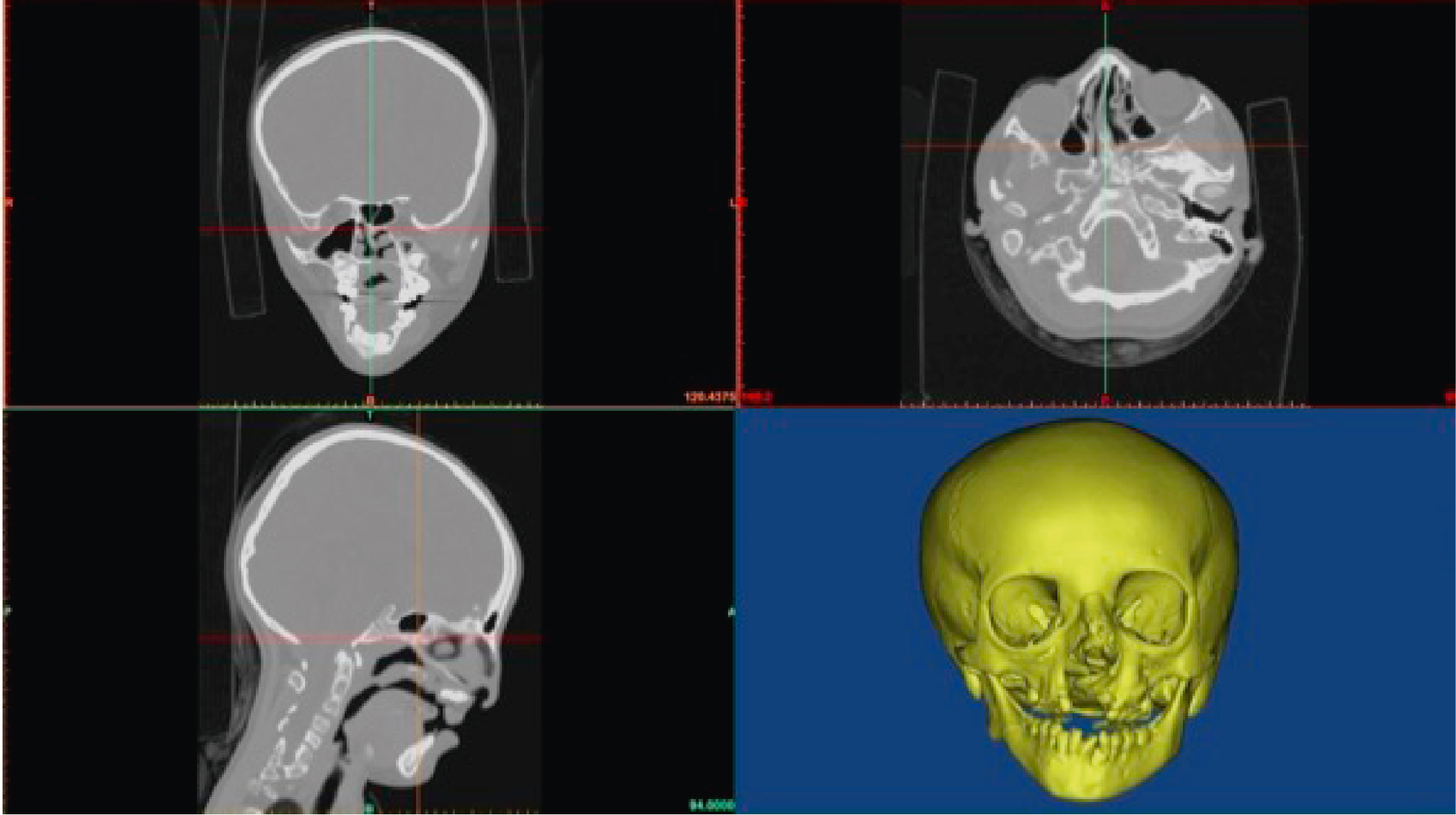
Contemporary CT scanners utilize multiple arrays of x-ray detectors and sophisticated helical-shaped radiation emission patterns, allowing for faster scans, more robust data collection, and undistorted image display in all anatomic orientations (axial, coronal, and sagittal) ( Fig. 7.2 ).