Psoriasis
Lauren Fried
Gabriela A. Cobos
David Cohen
BACKGROUND
Psoriasis is a chronic immune-mediated inflammatory disorder characterized by hyperproliferation of keratinocytes leading to epidermal hyperplasia, scaling, and inflammation. The prevalence of psoriasis is 2% to 4% in Western countries. The disease can occur at any point in life, although an increase in prevalence is seen with age. Most common peaks of onset occur between ages 30 to 39 years or 50 to 69 years.1
PRESENTATION
Patients typically present in their third or sixth decade of life with usually asymptomatic or intermittently pruritic red, scaling patches on areas pertaining to the subtypes described later.
DIAGNOSIS
Clinical Diagnosis
The diagnosis of psoriasis is generally clinical with biopsies infrequently required. Well-demarcated, erythematous plaques with silvery scale are distributed on extensor joints; periumbilical, scalp, or intertriginous areas; or flexural areas. Alternatively, numerous small round to oval erythematous plaques with overlying scale may be generally distributed, sparing the face, in the setting of a preceding Streptococcal infection. Additional clinical presentations include generalized erythema or pustules (see section “Subtypes”).
Histopathology
Histological examination of psoriasis demonstrates regular acanthosis, elongation of rete ridges. There is parakeratosis, hypogranulosis, and suprapapillary thinning. Superficial capillaries are dilated and have a mild perivascular lymphocytic infiltrate.2
Subtypes
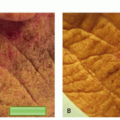
The clinical spectrum of psoriasis is wide. Chronic plaque psoriasis, which is the most common variant, is characterized by well-demarcated, erythematous plaques with silvery scale. Distribution is highly variable, but
the most commonly affected sites are scalp (75%-90% of patients), knees, elbows, sacrum, periumbilical, perianal, retroauricular, and intertriginous regions.3
the most commonly affected sites are scalp (75%-90% of patients), knees, elbows, sacrum, periumbilical, perianal, retroauricular, and intertriginous regions.3
Guttate psoriasis presents acutely with numerous, small, scaly papules. It is most commonly seen in children and adolescents and is often preceded by a Streptococcal infection.
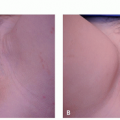
Inverse psoriasis presents with shiny, pink, thin plaques in flexural areas. These plaques often lack scale. Of note, localized infection (bacteria, candida, dermatophyte) in these areas can be a trigger for inverse psoriasis.
Erythrodermic psoriasis presents with generalized erythema with scaling and sparing of the face. Its onset can be acute or gradual.
Pustular variants of psoriasis present with erythema and pustules, which may be generalized or localized; systemic symptoms of fever and malaise may be present.
Acrodermatitis continua of Hallopeau is a rare variant of psoriasis, which presents with pustules at the distal fingers and toes. Pustules can also form in the nail bed and lead to destruction and/or loss of nail plate.
Nail psoriasis has been reported in 80% to 90% of patients with plaque psoriasis and can present with thickening, yellowing, pitting, or crumbling of the nail plate.4 Patients with nail changes have an increased risk of psoriatic arthritis.
Differential Diagnosis
Cutaneous T-cell lymphoma
Eczematous dermatitis
Lichen planus
Seborrheic dermatitis
Tinea corporis
Pityriasis rosea
Lichen simplex chronicus
Squamous cell carcinoma
Secondary syphilis
Reactive arthritis
PATHOGENESIS
The etiology of psoriasis is complex and involves an interplay between genetics, the immune system, and environment.5 Triggering events may include stress, infection, trauma, or certain medications. Once triggered, the disease process of psoriasis involves dysregulation and inappropriate activation of the cutaneous immune system. Increased activation of T cells and production of proinflammatory cytokines, including tumor necrosis factor (TNF)-α, interleukin (IL)-12, IL-17, IL-22, and IL-23, leads to hyperproliferation of keratinocytes, further T-cell activation, and vasodilation in the surrounding tissue.6,7 Accelerated cellular turnover prevents normal cellular maturation and lipid release, impairing cell-cell adhesion in the stratum corneum and leading to scaling. It is now well recognized that this inflammation is not limited to the skin and may also have profound systemic effects.
Risk Factors
Genetics are known to play a role in the development of psoriasis, with 40% of affected adults reported to have at least 1 first-degree relative with the condition.8 A number of loci have been linked to psoriasis (PSORS I-IX), with the HLA-Cw6 allele (PSORS-I) recognized as the major susceptibility gene for psoriasis.9 Psoriasis can also be triggered by environmental factors such as stress, infections (particularly bacterial), skin trauma, or certain drugs. For example, beta blockers, lithium, nonsteroidal anti-inflammatory drugs, angiotensin converting enzyme inhibitors, oral corticosteroids, and antimalarials have been reported to induce flares of or exacerbate existing psoriasis.10
Comorbidities
Psoriatic arthritis develops in up to 30% of patients with psoriasis.11 The skin precedes the joints in 85% to 90% of patients. The presence of psoriasis is an independent risk factor for a number of conditions including Crohn disease, congestive heart failure, metabolic syndrome, nonalcoholic fatty liver disease, and malignancy.12 Patients with severe psoriasis are at an increased risk of cardiovascular disease (myocardial infarction, pulmonary emboli, peripheral arterial disease, cerebrovascular accidents) and an associated approximate 6-year reduction in life expectancy.13
The associated increase in morbidity and mortality highlights the importance of a comprehensive history and physical and the need for an interdisciplinary approach in the evaluation and treatment of patients with psoriasis.
Quality of Life
In addition to dysesthetic symptoms and comorbid conditions, the perceptible nature of psoriasis can
have a dramatic impact on interactions with others, self-perception, and quality of life. Visible lesions lead to feelings of contagion, uncleanliness, and unattractiveness, impacting a patient’s perception of their acceptability to self and to others. This is reflected in commonly reported feelings of frustration, helplessness, embarrassment, and self-consciousness.14 The psychological burden of psoriasis has been reported to match those of significant chronic conditions such as congestive heart failure, myocardial infarction, and cancer.15 Furthermore, patients with psoriasis experience elevated rates of anxiety, depression, and suicidal ideation. Patients are less likely to be employed and more likely to miss days of work, with the vast majority citing psoriasis as the cause.16 It is important to consider that the impact of psoriasis on quality of life may not be correlated with clinical severity of disease. The psychosocial burden of psoriasis is substantial and should play a major role in guiding therapy. In addition, the symptomatic aspect of psoriasis is often underappreciated, with many patients experiencing pruritus or pain. This can lead to disruption of sleep and ability to participate in activities of routine daily living.
have a dramatic impact on interactions with others, self-perception, and quality of life. Visible lesions lead to feelings of contagion, uncleanliness, and unattractiveness, impacting a patient’s perception of their acceptability to self and to others. This is reflected in commonly reported feelings of frustration, helplessness, embarrassment, and self-consciousness.14 The psychological burden of psoriasis has been reported to match those of significant chronic conditions such as congestive heart failure, myocardial infarction, and cancer.15 Furthermore, patients with psoriasis experience elevated rates of anxiety, depression, and suicidal ideation. Patients are less likely to be employed and more likely to miss days of work, with the vast majority citing psoriasis as the cause.16 It is important to consider that the impact of psoriasis on quality of life may not be correlated with clinical severity of disease. The psychosocial burden of psoriasis is substantial and should play a major role in guiding therapy. In addition, the symptomatic aspect of psoriasis is often underappreciated, with many patients experiencing pruritus or pain. This can lead to disruption of sleep and ability to participate in activities of routine daily living.
TREATMENT
Treatment should be based on the extent of disease and degree of impact on the patient’s quality of life. Psoriatic arthritis may influence the choice of systemic therapy. Special consideration of side effects and contraindications should also be taken in women who are pregnant, nursing, or of childbearing potential
Further classification of severity of the disease can be made based on the following criteria:
Percentage of body surface area involved: If more than 5% of the body surface area is affected, the patient is generally considered to have moderate disease and may be offered systemic therapy.
Severity and dysesthetic qualities of individual lesions: Pain, pruritus, or particularly severe, recalcitrant plaques.
Involvement of critical areas: Consider lesions on areas such as hands or feet, which might interfere with occupation or activities of daily living, as well as those in cosmetically visible areas, which might have a greater psychosocial impact.
Logistical concerns: Likelihood of consistency and compliance with topical treatments; ability of patient to come to the office regularly for phototherapy treatments; accessibility to medication, including socioeconomic considerations, which may impact access.
How the individual patient is affected: Given that psoriasis can have such a profound impact on a patient’s quality of life, the patient’s desired level of control should be an important factor when choosing a treatment. Additionally, it should not be assumed that percent surface area or visibility of lesions directly correlates with functional and emotional impact and this needs to be clearly addressed with each patient.
Based on the above-mentioned considerations, the physician can classify his or her patient as requiring treatment for limited or extensive disease. Algorithm 14.1.1 provides options for treating psoriasis based on severity.
Limited Disease
First-line treatments for limited disease are mainly topical treatments, but they can also include intralesional injections and targeted phototherapy. Treatments for mild to moderate psoriasis are described in Table 14.1.1.
Medical
Topical Treatment. About 70% to 80% of patients have mild psoriasis, which can be controlled with topical treatment.15 These treatments generally have fewer side effects than systemic options but require patient compliance in regular application.
Intralesional Treatment. Intralesional treatment can be used in conjunction with topical treatment to inject steroid directly into plaques that are more prominent or recalcitrant.
Cosmetic/Laser Light Based
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


