The author describes 13 years of experience in the application of a new and simple method of facial cutaneous detachment using specially designed bifaceted rigid steel wands called Dilson Luz Vascular Dilation Wands. This technique, termed progressive tunnelizations , involves stretching the blood vessels to the point of rupture by inserting progressively larger wands. At the point of rupture, a spontaneous coagulation within the vascular extremities occurs. With this new technique, the author has obtained improved cutaneous detachment; reduced postoperative swelling, edema, and ecchymosis; prophylaxis of facial nerve damage; and/or late postoperative hematoma formation.
Key points
- •
Bleeding and facial nerve lesions are the greatest obstacles to a safe postoperative recovery in patients who undergo face and neck lift surgery.
- •
Hematoma complications are directly proportionate to the volume of blood accumulated and the time elapsed between the hematoma formation and its drainage.
- •
Complications typically occur from simple ecchymosis to cutaneous necrosis caused by excessive cauterization or tension on the closure.
- •
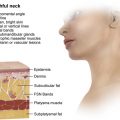
The Tunnelization in the subcutaneous plane technique emphasizes great attention to the liberation of the ligaments of the mandible, preserving the vascularity and the innervation in the ligament area. This is also performed in the middle third of the face.
- •
Patients who undergo face and neck lifting with detachment through progressive ‘tunnelizations’ show better recovery than those who undergo conventional rhytidoplasty, since they suffer less skin, vascular and nerve trauma performing cutaneous detachment with few cauterizations.
Editor Commentary: I met Dilson while teaching in Brazil and was fascinated by his enthusiasm for a technique that seemed interesting and useful. Basically Dilson designed a series of dilators to perform blunt tunneling of the neck and face which allowed repositioning of soft tissues without extensive undermining with the added benefit of reducing the risk of hematoma formation. By squeezing the vessels in the flap, there is virtually no bleeding, explained in his section on physiology, and when I added this to my routing necklift technique, I enjoyed infrequent accumulations of blood and seroma fluid in the neck. I also found this step valuable in decreasing the risk of skin loss in smokers as I did not detach the neck flap, leaving important fasciocutaneous perforators to nourish a flap whose circulation may be compromised.
Introduction
Face-lifting surgery is progressing through clinical research and documentation of results as well as sequelae, complications, and longevity ( [CR] ). The round-lifting technique described by Pitanguy and colleagues and based on a directional study of the vector for the lifting of sagging skin, as well as the necessary skin incision, reflects the search for efficiency in facial surgery. The changes in incisions have shown vast progress, securely preventing the elevation of the sideburn with the peninsula technique idealized by Pontes. Mitz and Peyronie established the anatomic basis for the superficial musculoaponeurotic system (SMAS) treatment, additionally defining that the SMAS adherences to the parotid fascia form a fixed tissue and that anterior to the parotid the SMAS is mobile. Hakme claims (and the author agrees) that the treatment of the SMAS (with imbrication or with SMASectomy) only maintains the results if the movable SMAS is sutured to a fixed base. There are instructions about how to avoid nerve lesions and precise anatomic descriptions for interventions in the premasseteric space (Mendelson and colleagues ), collaborate in the prevention of complications. Vasconez and colleagues defined the basis for video-endoscopic facial surgery, and Badin and colleagues are credited with the surgery with vector modifications and wire traction. In addition, the critiques and evaluations of complications from the use of a barbed suture, mentioned by Paul, reflect the masters’ concerns in guiding the future generations with safety.
Despite so much research and technological innovations, the bleeding problems caused by surgery, as well as the attempts to minimize its complications, persist. The facial nerve lesions continue equally frequently, even in experienced hands and with the use of preventive procedures.
Based on the author’s experience and on extensive bibliographic research, he ascertains that bleeding and facial nerve lesions are the greatest obstacles to a safe postoperative recovery in patients that undergo face- and neck-lift surgery.
In order to have more dense and uniform skin flaps (because the subcutaneous vascular plexus is mostly responsible for skin irrigation ), reduce bleeding during surgery, avoid immediate or late postoperative hematoma formation, and minimize the risks of facial nerve lesions, the author would like to present his technique, which is a pioneering effort in face and neck lifting: detachment with progressive tunnelizations using the Dilson Luz Vascular Dilation Wands (Mad Colant, Jaboatão, Pernambuco) ( Fig. 1 ). This technique can be applied in other surgeries, such as lipo-abdominoplasty, prosthesis inclusion in calves and breasts, inclusions of expanders, breast reconstructive surgery, and gluteal muscle lifts. This technique was used and reproduced with success.
In surgeries performed through classic techniques, the manual drainage of the collected blood from the hemifaces already sutured are common, and cases of the removal of stitches to check the hemostasis at the end of the surgery are not rare. It is common knowledge among surgeons that the return of patients to surgical centers to check for hematomas happens with a certain frequency. These patients are not always exempt from complications, which are directly proportionate to the volume of blood accumulated and the time elapsed between the hematoma formation and its drainage. Usually, complications occur from a simple ecchymosis to cutaneous necrosis, accompanied or not with neurologic lesions caused by cauterization or section of nerves.
In the author’s technique, special attention is given to the ease of doing the detachment of the neck and of the middle third of the face (which is divided into superficial and profound), safely guiding the liberation of the zygomatic ligaments through the profound detachment supraperiostal tunnelized and progressive superficial detachment for the elevation of the malar fat pad. The author emphasizes the care for the liberation of the ligaments of the mandible, prolonging the detachment of the middle third superficial, tunnelizing progressively in the subcutaneous plane for these ligaments, observing the vascularization, the innervation, and the ligament area ( Figs. 2 and 3 ) (becomes Fig. 2 A, B) , which was so well demonstrated by Furnas.
In 2003, the author presented his technique for the first time. In 2005, the author published his technique in Aesthetic Plastic Surgery . In 2006, the author published it in an Brazilian Society of Plastic Surgery – Region São Paulo (SBCP) São Paulo book; in 2010, he edited his book on the technique.
Technique Fundamentals
The physiology is explained by the vascular intima section that provokes the platelet migration to the injured area, following the immediate coagulation within the vascular extremities, because these were submitted to a progressive stretching with large dilators in its lights before the section, obtaining trapped clots in the extremities of the sectioned vessels, which block the blood flow (see Fig. 3 ).
Physiology
The observation that, in emergencies, patients who underwent amputation of their hands by pull out presented minimum blood loss ( Fig. 4 A ) and that patients who suffered identical amputation but caused by sharp objects suffered from severe anemia (see Fig. 4 B) raised the question of how to prevent hemorrhaging during the detachment of the face. The author transferred this idea to perform the neck-face detachment (see Fig. 4 C).
Introduction
Face-lifting surgery is progressing through clinical research and documentation of results as well as sequelae, complications, and longevity ( [CR] ). The round-lifting technique described by Pitanguy and colleagues and based on a directional study of the vector for the lifting of sagging skin, as well as the necessary skin incision, reflects the search for efficiency in facial surgery. The changes in incisions have shown vast progress, securely preventing the elevation of the sideburn with the peninsula technique idealized by Pontes. Mitz and Peyronie established the anatomic basis for the superficial musculoaponeurotic system (SMAS) treatment, additionally defining that the SMAS adherences to the parotid fascia form a fixed tissue and that anterior to the parotid the SMAS is mobile. Hakme claims (and the author agrees) that the treatment of the SMAS (with imbrication or with SMASectomy) only maintains the results if the movable SMAS is sutured to a fixed base. There are instructions about how to avoid nerve lesions and precise anatomic descriptions for interventions in the premasseteric space (Mendelson and colleagues ), collaborate in the prevention of complications. Vasconez and colleagues defined the basis for video-endoscopic facial surgery, and Badin and colleagues are credited with the surgery with vector modifications and wire traction. In addition, the critiques and evaluations of complications from the use of a barbed suture, mentioned by Paul, reflect the masters’ concerns in guiding the future generations with safety.
Despite so much research and technological innovations, the bleeding problems caused by surgery, as well as the attempts to minimize its complications, persist. The facial nerve lesions continue equally frequently, even in experienced hands and with the use of preventive procedures.
Based on the author’s experience and on extensive bibliographic research, he ascertains that bleeding and facial nerve lesions are the greatest obstacles to a safe postoperative recovery in patients that undergo face- and neck-lift surgery.
In order to have more dense and uniform skin flaps (because the subcutaneous vascular plexus is mostly responsible for skin irrigation ), reduce bleeding during surgery, avoid immediate or late postoperative hematoma formation, and minimize the risks of facial nerve lesions, the author would like to present his technique, which is a pioneering effort in face and neck lifting: detachment with progressive tunnelizations using the Dilson Luz Vascular Dilation Wands (Mad Colant, Jaboatão, Pernambuco) ( Fig. 1 ). This technique can be applied in other surgeries, such as lipo-abdominoplasty, prosthesis inclusion in calves and breasts, inclusions of expanders, breast reconstructive surgery, and gluteal muscle lifts. This technique was used and reproduced with success.