Anchoring platysma muscle on fixed points of the face is not new. Revolutionary high superficial muscular aponeurotic system techniques and a thorough knowledge of the anatomy of the tympanomastoid fascia give us a stabile anatomic point to fixate platysma muscle. This structure combined with supraplatysmal or subplatysmal defatting, partial resection of the anterior belly of the digastric muscle, approximation of platysmal bands, or corset platysmaplasty and correction of prominent submandibular salivary glands help us to enhance the cervical area and restore ptotic neck deformities in a single procedure.
Key points
- •
Lorre’s fascia as anchor point provides strong support to the young hanging neck without the need for further subplatysmal dissection.
- •
An additional subplatysmal dissection and submental approach with liposuction and digastric manipulation addresses problems of heavier problematic necks.
- •
Facial contour is restored in a natural, long-lasting result.
Editor Commentary: Athanasias spent a six month aesthetic fellowship with me and frequently visited Bruce Connell as well. He shares his answers to my questions in a logical manner utilizing the strength of Lore’s fascia and the mastoid fascia to anchor the SMAS/platysma flap. These fixed structures limit anterior and inferior flap migration after anchoring. He describes his approach to the various layers of submandibular fat as well as the indication for partial resection of the anterior belly of the digastrics muscles. His European patient population includes many smokers and his admonition to avoiding aggressive flap dissection is important to remember.
Technique
Managing Aging Necks
The surgical necessity to individualize each patient’s needs to one specific technique enabling the surgeon to offer a satisfactory result in all varieties of an aging neck is meaningless. From our experience, there is no one-for-all technique to address every anatomic area found in existing or potential problems on the constantly shrinking neck cylinder. Skin flaccidity, supraplatysmal or subplatysmal excess fat, mandibular border definition, visible active or static platysma muscle bands, and submaxillary gland protrusion form a certain reconstructive ladder that guides our surgical steps. Our neck lift procedure is a combined chain of these steps with a sense of priority. Our responses to the questions asked are as follows:
What incisions do you typically use in the thin neck and the heavy neck in both young and older patients?
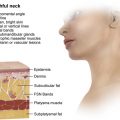
Skin-incision length is roughly guided by the degree of skin laxity. Limited skin incisions (or short scar lifts) are best suited for young candidates with mild excess skin and more soft tissue loss of support. Usually the midface is not yet affected, so no high superficial muscular aponeurotic system technique or extended excision is required. Lateral surgical excision of SMAS or plication is enough to correct the descending face and neck. We think that using the mastoid and Lorre’s fascia as anchor points provides strong support to the young hanging neck without the need for further subplatysmal dissection. If supraplatysmal fat is problematic, it can be suctioned using a flat cannula with a special effort not to skeletonize the submandibular area and, therefore, reveal an enlarged submandibular gland or a prominent anterior digastric belly ( Fig. 1 ).
A submental approach is being introduced in our surgical protocol when a pinch test indicates the presence of a substantial amount of subplatysmal fat that requires open cervical lipectomy. A 3- to 4-cm incision is then placed about 1 cm inferiorly to the submental crease to provide better healing conditions, an inconspicuous scar, and to avoid the double-chin deformity. If the neck skin is loose, then we extend the incision behind the earlobe, leaving a 3-mm cuff of skin below the junction to the cheek ( Figs. 2 and 3 ). The incision is carried backward following the earlobe-postauricular skin junction and, at the level of the tragus (or sometimes 5 or 10 mm higher), is turned toward the hairline with a cutting angle parallel to the hair follicles, with a special effort to preserve them. Through this incision, we can remove large amounts of flaccid skin, avoid unpleasant folds, and respect the natural relaxing lines of the neck. In this way, we avoid the danger of creating a pulled look, which is a disfiguring disadvantage of various U-shaped incisions ( Fig. 4 ).
What is your approach to defatting the heavy neck? Which fatty layers do you resect (ie, subcutaneous, interplatysmal, subplatysmal fat)?
A limited superficial liposuction is performed in the submental area before our face procedures. The purpose is not a precise preplatysmal fat removal rather than an atraumatic dissection on the supraplatysmal plane of the neck. The skin flap is raised using the 4-handed technique under direct vision aided by transillumination, and the dissection proceeds to the avascular plane about 1 cm medial to the anterior border of the sternocleidomastoid muscle. Then the surgical plane is divided, and the superficial part is connected to the previous liposuction plane where fat is trimmed with scissors while the deep plane travels on the superficial cervical fascia under the platysma muscle ( Fig. 5 ).
If subplatysmal fat is bulgy, we elevate the anterior part of the platysma muscle using 2 Alice clamps; we tangentially excise the trapezoid deep fat until we reach the level of anterior belly of the digastric muscle. We seldom need partial resection of the anterior belly of digastric muscle because the over-resection of fat creates a characteristic deepening of the frontal part of the neck, which gives the impression of a gunshot deformity.
How does the presence of visible platysma muscle bands alter your approach? Do you undermine, plicate, transect, and partially resect platysmal muscle bands?
To address thin soft bands in a young neck, a lateral fixation to Lore’s and mastoid fascia anchoring points is usually enough, providing a good satisfaction rate to our patients ( Figs. 6–13 ).
When we have to deal with multiple or hard bands, we think it is highly important to evaluate the platysma muscles diastasis in the midline. We usually suture it using 4.0 polydioxanone sutures by performing invagination of the medial aspect of platysma muscle and a back cut in the area above the cricoid. When dealing with multiple bands on fatty necks, a boomerang incision of the platysma is appropriate, which connects the lower part of platysma muscle with the previously elevated flap in front of the sternocleidomastoid muscle. This maneuver provides better definition and less contracture of the neck. We begin with small bites from the mastoid fascia up to the proximal third of the mandible in order to avoid any damage to the marginal mandibular branch, using 4.0 nylon sutures. This surgical manipulation achieves the goal of improving and supporting the definition of the mandible. A corset platysmaplasty may be combined with all of the aforementioned procedures depending on the extent of the problem in the initial phase ( Figs. 14 and 15 ).