This article reviews the broad range of effective options for the nonexcisional rejuvenation of the neck. It discusses the relevant noninvasive anatomy of the neck, classification of the procedural options for the aesthetic cervical physician, and specific anatomic management strategies for each category of cosmetic cervical therapy. This article is a guideline and reference for physicians performing excisional and nonexcisional procedures of the neck. The list of noninvasive, light-energy, radiofrequency, ultrasound energy and suspension technologies is extensive and the author has included those that are most relevant, commonly used, and/or highly efficacious. Promising up-and-coming treatments are introduced and discussed.
Key points
- •
This paper describes nonexcisional techniques for neck rejuvenation.
- •
External and subcutaneous and subdermal laser, RF, light, ultrasound and injectable treatments are reviewed.
Editor Commentary : Steve and I have been involved in several emerging technologies and have had the pleasure to discuss alternative and additive modalities with him frequently. In this chapter, Steve takes us on the journey of minimally invasive and non-invasive energy based techniques to rejuvenate the aging neck. He frequently combines these techniques with open aggressive procedures. Realizing that minimally invasive techniques can provide measureable skin tightening has provided yet another opportunity to answer our patients’ desires for procedures with a quicker recovery. Of course these can be stand alone procedures or performed along with or following more aggressive surgical maneuvers. The patient with minimal submental and or jowl laxity after a face and necklift looks to us to provide a solution. For sure, we enjoy surgery more than our patients and therein lies their quest for an easy answer without surgical expense and downtime.
Introduction
Western civilization is experiencing a “boom in boomers,” an aging population, with population decline. The aging population in Western Europe, North America, and Asia has disposable income and the mantra of “youth and vitality” has this generation increasingly presenting for aesthetic treatments, specifically noninvasive or nonexcisional procedures. The neck aesthetic subunit often ages early and more noticeably than other head and neck regions and is one of the most common motivations for patients to present to aesthetic physicians for rejuvenation options. The neck undergoes extrinsic and intrinsic aging changes in all anatomic layers and the aesthetic physician must be well equipped to deal with aging cervical concerns, both surgically and nonsurgically. For the surgeon, being skilled in nonsurgical cervical rejuvenation is critical, as many patients may opt for nonexcisional cervical enhancements, alone, or in combination with other facial cosmetic surgical procedures. For the cervical surgeon, a familiarity and expertise with nonsurgical management of the neck, as “stand-alone” therapy or as postoperative “protect your investment” treatments, may help extend and prolong the achievements achieved surgically.
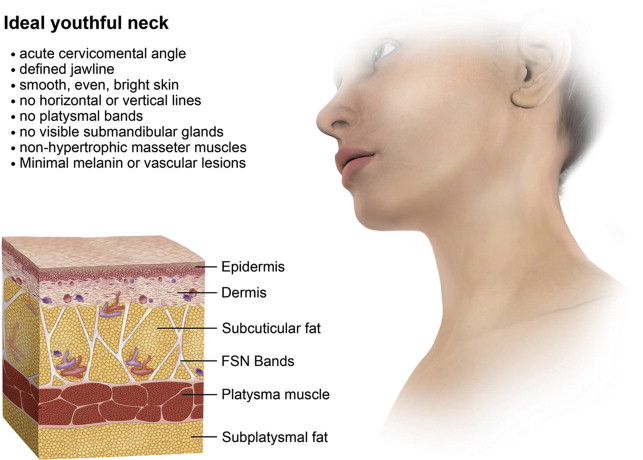
A youthful neck is most often characterized by an acute cervicomental angle and a firm, well-defined jawline ( Fig. 1 ). The skin in a youthful neck is smooth and devoid of horizontal or vertical neck lines; has no platysmal bands; no visible submandibular glands; small, nonhypertrophic masseter muscles; and skin that is bright and even in color, with minimal melanin or vascular lesions.
For the nonexcisional cervical physician, aesthetic rejuvenation of the neck with a multimodal, nonexcisional, minimally invasive approach will be a very common and popular component of the facial aesthetic practice. For all aesthetic physicians, familiarity with the aging tissue changes of the neck, its anatomy and the possible minimally invasive, nonexcisional interventions, including laser, light, radio frequency, high-intensity focused ultrasound (HIFU) energy-based therapy, both transepidermal and subdermal approaches, injectable soft tissue fillers, neuromodulators, and ablative and nonablative technologies for skin rejuvenation, as well as suture-based suspensory techniques, all used alone or in combination, will be a valuable asset to the global aesthetic head and neck cosmetic physician.
This article brings together the “tried-and-true” nonexcisional neck rejuvenation methodologies, which have had long-term, peer-reviewed success in the literature, together with procedures and technologies that have emerged in the past few years that have proven to be successful and complementary. It is my hope that this information assists aesthetic physicians in enhancing their global approach to nonexcisional rejuvenation of the neck.
Introduction
Western civilization is experiencing a “boom in boomers,” an aging population, with population decline. The aging population in Western Europe, North America, and Asia has disposable income and the mantra of “youth and vitality” has this generation increasingly presenting for aesthetic treatments, specifically noninvasive or nonexcisional procedures. The neck aesthetic subunit often ages early and more noticeably than other head and neck regions and is one of the most common motivations for patients to present to aesthetic physicians for rejuvenation options. The neck undergoes extrinsic and intrinsic aging changes in all anatomic layers and the aesthetic physician must be well equipped to deal with aging cervical concerns, both surgically and nonsurgically. For the surgeon, being skilled in nonsurgical cervical rejuvenation is critical, as many patients may opt for nonexcisional cervical enhancements, alone, or in combination with other facial cosmetic surgical procedures. For the cervical surgeon, a familiarity and expertise with nonsurgical management of the neck, as “stand-alone” therapy or as postoperative “protect your investment” treatments, may help extend and prolong the achievements achieved surgically.
A youthful neck is most often characterized by an acute cervicomental angle and a firm, well-defined jawline ( Fig. 1 ). The skin in a youthful neck is smooth and devoid of horizontal or vertical neck lines; has no platysmal bands; no visible submandibular glands; small, nonhypertrophic masseter muscles; and skin that is bright and even in color, with minimal melanin or vascular lesions.
For the nonexcisional cervical physician, aesthetic rejuvenation of the neck with a multimodal, nonexcisional, minimally invasive approach will be a very common and popular component of the facial aesthetic practice. For all aesthetic physicians, familiarity with the aging tissue changes of the neck, its anatomy and the possible minimally invasive, nonexcisional interventions, including laser, light, radio frequency, high-intensity focused ultrasound (HIFU) energy-based therapy, both transepidermal and subdermal approaches, injectable soft tissue fillers, neuromodulators, and ablative and nonablative technologies for skin rejuvenation, as well as suture-based suspensory techniques, all used alone or in combination, will be a valuable asset to the global aesthetic head and neck cosmetic physician.
This article brings together the “tried-and-true” nonexcisional neck rejuvenation methodologies, which have had long-term, peer-reviewed success in the literature, together with procedures and technologies that have emerged in the past few years that have proven to be successful and complementary. It is my hope that this information assists aesthetic physicians in enhancing their global approach to nonexcisional rejuvenation of the neck.
Aesthetic cervical anatomy of the neck
This issue of Clinics in Plastic Surgery deals extensively with the surgical options and management of the aging neck. However, the noninvasive, minimally invasive and nonexcisional solutions for the neck are often what patients opt for and, many times, are techniques and strategies that can also enhance and/or extend surgical results, or can be applied following surgical neck procedures to provide smaller enhancements and maintenance of the outcome postoperatively.
The aesthetic anatomy of the neck can be divided into several layers, from superficial to deep, starting with the skin, subcutaneous tissue, superficial musculo-facial layer and deep subplatysmal structures ( Fig. 1 ). In this section, the relevant anatomy of the neck as it pertains to minimally invasive and noninvasive rejuvenation procedures is outlined and then cervical enhancement options for each layer follow.
The anatomic classification of the neck pertains to the aging structures as the patient sees them and to the anatomic options and targets that the aesthetic physician may elect to treat, which are outlined in Fig. 2 .
Cutaneous Cervical Layer
The cutaneous layer of the neck consists of a relatively thin epidermis and dermis. The skin of the neck is subject to multiple mimetic and cervical animations, and tensile and compressive loads. Bending the neck in the anterior-posterior direction, as well as side to side with active contraction of the underlying platysma, can lead to horizontal lines or “necklace lines.” The skin ages as a consequence of intrinsic (genetic) and extrinsic (applied) forces. The neck itself is often exposed to the sun and may not be protected by sunscreen and, thus, often presents with significant extrinsic photoaging. Cervical photoaging will result in increased epidermal thickness, degeneration of functional elements of the cervical dermis, such as useful collagen, elastin, and ground substances, with accumulation of whorls of elastotic collagen in the deep dermis ( Fig. 3 ). Aging laxity of the platysmal muscle may lead to visible central and/or lateral neck bands. The cumulative photoaging of the neck combined with intrinsic aging and mimetic changes results in a typical aging cutaneous cervical envelope, characterized by thin “crepe” skin, diffuse dyschromia and telangiectasia, with multiple vertical lines in the midline, affectionately termed “iguana neck,” as well as horizontal lines, centrally and laterally, attributed to platysma and cervical motion (see Fig. 3 ).
The aesthetic physician needs to be especially skilled in the rejuvenation of the cutaneous layer of the neck. Surgeons performing excisional neck surgery can often fail to deliver optimal neck rejuvenation results by not being familiar with, or equipped to deal with, superficial aging changes of the neck. The superficial cutaneous aging changes to the neck do not respond optimally to pure tensile repositioning characterized by neck lift surgery, but rather, respond to multimodal, noninvasive treatments designed to improve the more superficial color, tone, and texture of the skin. Similarly, nonsurgical aesthetic physicians need to familiarize themselves with the various nonexcisional treatment modalities used to rejuvenate the cutaneous layers of the aging neck.
Subcutaneous Cervical Layer
Deep to the cutaneous, epidermal-dermal layer of the neck is subcutaneous or adipose tissue. There can be a wide variation in aging presentations of the cervical subcutaneous layer. Some patients have aging cervical phenotypes that have little subcutaneous fat between the deep dermis and the underlying platysma, whereas other patients have extensive amounts of subcutaneous fat between the dermis and the platysma. Modest-to-large amounts of subcutaneous fat will create an obtuse angle to the cervicomental angle and detract from what is considered a youthful neck. An ideal neck consists of a vertical cylinder, the trachea and muscles that connect as a right angle to the floor of the mouth and submandibular tissue, forming a 90° angle (see Fig. 1 ).
Subcutaneous fat of the neck is generally less fibrous than adipose tissue of the trunk or thighs and is a single layer with interlobular fascial components connecting the platysma layer on its deep surface to the dermis. It is imperative that the aesthetic physician be able to diagnose subcutaneous fat, which is preplatysmal, from subplatysmal fat, which will also compromise the acute cervicomental angle, but is more difficult to access and to treat without incisional or excisional surgery.
The Cervical Platysmal Layer
The platysma bands are wide, broad strap-shaped skeletal muscles extending from the clavicle to the dermal attachments along the mandibular border. The cervical platysma is invested by the superficial layer of the deep cervical fascia and will extend superiorly as the superficial-muscular aponeurotic system (SMAS). The platysma comes in a number of anatomic variants, including those with no central diastasis and those with a wide central diastasis that may present as medial platysmal bands. The platysma itself has been attributed the aesthetic function of a secondary depressor of the modiolus, synergetic to the primary depressor of the corner of the mouth, the depressor angularis oris (DAO), and in this fashion, the lateral platysmal bands can act as a depressor of the midface, commissure, mouth, and jawline.
The platysma itself, when hypertonic, can lead to distracting aesthetic contours, causing obliquity of the otherwise youthful, acute cervicomental angle (see Fig. 3 ). With aging and muscle flaccidity and atrophy, the platysma bands can contribute to cervical laxity, creating a loose, adynamic, and obtuse neck. The aesthetic physician should be prepared to treat the cervical platysma when it is aesthetically important to the an optimal rejuvenative outcome, and excisional physicians, in addition to surgical manipulation and excision transection techniques, must also be able to manage nonoperatively any dynamic preoperative and postoperative cervical aesthetic problems.
Subplatysmal Aesthetic Structures
The subplatysmal aesthetic structures that can be treated nonexcisionally or minimally invasively include the densely packed, subplatysmal, adipose tissue that is present in a significant proportion of cervical aesthetic patients, as well as the submandibular glands. The deeply compacted subplatysmal fat lies on top of the mylo-hyoid muscle and may contribute to a “double chin” or obtuse cervicomental angles, and the aesthetic physician needs to be able to diagnose, either by clinical examination or ultrasound techniques, when the submental fat is due to preplatysmal or subplatysmal pathology. Suctioning subplatysmal fat may require a small incisional localization of the platysma to place the cannula in the subplatysmal plane, or open subplatysma lipectomy.
The other deep platysmal structures that occasionally require aesthetic management and nonexcisional treatment are the submandibular glands. The submandibular glands measure approximately 3 × 5 cm and are secondary salivary glands that rest in the lateral floor of the mouth and they can occasionally be visible as lumps or soft tissue shadows in the lateral neck. These glands can be particularly visible postoperatively after tightening or suction reduction procedures of the anterior and lateral neck. Both the excisional and nonexcisional cervical aesthetic physician needs to be able to address prominent submandibular glands (see Fig. 3 ).
Anatomic, nonexcisional management of the neck
Cutaneous Layer
Chromaphore-based pathologies
Melanin-dyschromia
Melanin discoloration, or dyschromia, of the neck is common, given its sun-exposed location on the head and neck region. Commonly patients will neglect to apply sunscreen or sunblock on their cervical region, yet cover the backs of their hands and their face. Over years of sun exposure, the typical photoaging appears. Melanin and dyschromia lesions can range from isolated solar lentigines or diffuse dyschromia and melisma. Diffuse brown discoloration is a very common presentation of the aging neck. Quite frequently, the dyschromia is associated with other signs of photoaging, including thickening and hyperkeratosis of the epidermis layer, thinning dermis with decreased elasticity, decreased functional elastin and collagen, and elastotic whorls of disorganized collagen in the deep reticular dermis associated with fine or deep cervical rhytides (see Figs. 2 and 3 ). The cervical skin will often look vertically fissured or, even further, cobblestoned Fitzpatrick VIII, IX, or X type of rhytids can appear (see Figs. 2 and 3 ). The dyschromia, with or without photoaging is best treated with modalities that are either specific to the discoloration or nonspecific and ablative in nature. Historically, chemical peels of the neck, like complete laser ablative resurfacing, were fraught with potential for wound-healing complications, as the adnexal tissue in the cervical dermis is limited, with few sebaceous glands, pilosebaceous units, eccrine, or apocrine glands to reepithelialize completely ablated skin . Hence, the use of moderate strength office or home-based topical chemical correction of cervical dyschromia has become popular, with very mild chemical peels or “bleaching agents.” The bleaching regimens generally consist of combinations of retinoic acids 0.05% to 0.1%, or tazarotene 0.025% to 0.01%, alone or combined with hydroquinone 4%, 6%, or 8%, 4% Kogic acids, and occasionally mild hydrocortisone-compounded substances. Prescriptive skin bleaching programs include the popular Tri-Luma. Other skin care regimens, such as Obagi, SkinCeuticals, Physician Choice of Arizona, Skin Medica, and others, have been quite popular in gradually bleaching dyschromia of the neck using home-based programs. Office-based treatments include stronger chemical peels, although the risk of delayed reepithelialization and hypopigmentation or hyperpigmentation is greater when stronger preparations of glycolic, glycolic acid, trichloroacetic acid, or stronger topical chemical ablatives are deployed.
Over the past 15 years, chromophore-based lasers and light-based sources have become the mainstay of skin color correction and are arguably the gold standard of dyschromia-associated aging of the neck. Chromophore-based lasers and light-based systems have wavelengths of light that are specifically attracted to intra-epidermal, epidermal-dermal, and superficial dermal melanin, through a process called selective photothermolysis. Typically, wavelengths in the range of 500 to 800 nm will have some increased affinity for and selective absorption of superficial cervical melanin-based concerns. Some of the monochromatic focal wavelengths for the improvement of superficial epidermal-dermal melanin include the 532-nm wavelength Potassium titanyl phosphate (KTP) lasers, 694.5 nm Q-switched Ruby, and the 755 long-pulsed or Q-switched Alexandrite lasers, which have all been deployed in specific correction of dyschromia of the neck. Pulsed dye lasers in the 585-nm wavelength have also been deployed to treat not only vascular lesions but pigmented lesions of the neck. However, the one most popular light-based rejuvenation of the neck for dyschromia and vascular chromophores has become intense pulsed light, or IPL. IPL, broad-band flash lamps, or xenon flash lamps consist of visible wavelengths of light from 500 nm to 1200 nm all released during the same pulse. Specific cutoff filters are deployed in a variety of methods, with or without direct water cooling, interpositional gel, or air cooling in a multitude of intense pulsed light systems available on the market to treat very effectively melanin and vascular discoloration of the cervical skin. Generally, for cervical rejuvenation in skin types I, II, and III, with dyschromia, cutoff filters in the 515-nm to 580-nm range have been very successful. For skin types 4 and 5, long wavelength cutoff filters in the 590-nm to 640-nm ranges, lower energies, and longer pulse configurations have allowed the treatment of darker discoloration in patients with more advanced Fitzpatrick skin type. Using gentle energy with broad melanin absorption coefficients and overlapping 20% or so, each pulse can provide safe, effective clearance for even the most severe cervical dyschromia over several sessions.
Intense pulsed light treatments of the neck usually require 1 treatment every 3 to 4 weeks for a total of 3 to 5 treatments. It can be quite common to cause striping in the neck following early IPL therapy in patients with extensive photoaging, which is caused by a combination of aggressive settings and not overlapping the light guide sufficiently during each treatment, which results in aggressive fading of the treated neck adjacent to untreated skin that does not fade in color. Gentle settings, multiple sessions, and overlapping or crisscrossing can avoid this problem. It is important that the IPL settings are gentle moderate in fluence, as IPL may induce a permanent hypopigmentation or discoloration of the skin. Monochromatic treatment of the neck with focal monochromatic laser systems can cause a reticulated hypo-pigmented appearance to the cervical skin.
It is common in dyschromia and photoaging of the skin to have a relative white and protected area of skin color immediately under the chin and submentum superior to the hyoid cartilage. This “white patch” represents the shaded area naturally created by the projected pogonion of the mandible. It is important to try to blend the “white under chin” into the more dyschromic and photoaged, lateral, and inferior aspects of the neck. It is also important to blend the discoloration of the central and lateral neck into the posterior triangle and trapezius border. Additionally, carrying the treatment over the clavicle onto the precordial region will help minimize risk of demarcation between a treated neck and an untreated décolleté. Often, combining complete cervical dyschromia correction with décolleté will provide a natural blend between the rejuvenated neck, the chest, and the face (see Fig. 3 ).
The recent addition of fractional nonablative, fractional ablative lasers, and ablative fractional radiofrequency devices has also provided an opportunity to improve dyschromia and photoaging, as well as fine lines and texture of the neck. Although intense pulsed light and other monochromatic melanin-based wavelengths of light are very effective for brown and red “color correction,” they have little effect on fine rhytides and wrinkles and the use of ablative fractional carbon dioxide lasers, and, to a lesser extent, ablative fractional and nonfractional erbium lasers can have the simultaneous benefit of decreasing the dyschromia and improving fine lines, rhytides, and laxity. More recently, fractional radiofrequency devices, such as the Fractora (Invasix, Yokneam, Israel), have become available, which can provide variable depth and variable density needle-based tips for fractional ablative improvement of the dyschromia of the neck, as well as the textural improvements that can be equivalent to those achieved with carbon dioxide. At the same time, the Fractora delivers a nonablative, non-necrotic tightening of the cervical region. The Fractora delivers radiofrequency energy and a positive charge along each of the pins in the needle array, resulting in an ablative crater and a zone of nonablative, but irreversible, thermal coagulation. Following the ablative injury, the radiofrequency (RF) energy then flows from the tip of the pin to the negative side electrode, creating a rich woven network of nonablative RF dermal heating, tightening, and remodeling ( Figs. 4–6 ).
Complications of the management of melanin and dyschromia of the neck include scars from overzealous laser and light-based settings, hypopigmentation from aggressive settings that result in a complete or near-complete clearance of melanocytes, as well as demarcation from treated and untreated areas. Quite often, clinically, dyschromia occurs together with vascular discoloration, such as in Poikiloderma of Civatte, which is covered in the next section.
Vascular or hemoglobin-based cervical rejuvenation
In addition to dyschromia and melanin-based lesions, it is quite common to get superficial vascular proliferation as a part of extrinsic photoaging or intrinsic genetic aging of the neck. The vascular proliferation derived from photoaging responds very nicely to the intense pulsed light with the same cutoff filter spectrum mentioned in the dyschromia section. Occasionally, deep dermal and subdermal, proliferative vascular lesions occur in the neck and monochromatic long-pulse or variable pulsed wavelengths, such as long-pulsed neodymium-YAG or short-pulse and long-pulse, pulsed dye lasers are required. The combination of reticulated hyperpigmentation and vascular proliferation in the upper papillary and mid-dermis condition, called “Poikiloderma of Civatte,” is more common in the lateral part of the neck than centrally. This “red neck syndrome” is often treated effectively with intense pulsed light, and peer-reviewed studies showing the successful use of a pulsed dye laser for this condition have been reported. One of the complications of the treatment of vascular proliferation in the cervical region with monochromatic high-fluence, short-pulse duration lasers is only variable clearance of the reticulated hypopigmentation, leading to a partially white, “spotted leopard” look to the skin. Intense pulsed light used gently over several sessions is often the best modality to blend most evenly the vascular as well as the melanin discoloration in the neck.
Epidermal and dermal nonchromophore-based lesions
There are many nonchromophore-based aging pathologies of the cervical skin that must be addressed to achieve the optimal outcome for youthful neck rejuvenation. Procedures such as simple shave excision, chemical or thermal ablation of intra-epidermal papillomas, skin tags, compound moles, seborrheic keratosis, actinic keratosis, and a host of other pathologies can significantly improve the appearance of the neck (see Fig. 6 ). Superficial and deep dermal-epidermal rhytides can now be treated “off face” safely and effectively with fractional ablative lasers, CO2, Erbium, and fractional radiofrequency ablative systems ( Fig. 7 ).
Dermal and Subdermal Tightening Devices and Technologies
There has been a rapid evolution in our ability to provide moderate, nonexcisional skin tightening and wrinkle-reduction therapy with transepidermal energy devices. These new “energy-assisted” nonexcisional skin tightening procedures have become very important drivers of consumer interest, so it is critical that the aesthetic physician have a nonsurgical approach to cervical skin tightening. The first generation of the noninvasive skin-tightening technologies involved nonfractionated longer wavelength near infra-red laser devices, such as the 1320-nm Cooltouch (Roseville, CA), the 1440-nm Smoothbeam (Syneron Candela, Yokneam, Israel), the long-pulsed Nd:YAG, and the 1320 to 1440 nm synchronously pulsed Affirm MPX (Cynosure, Westford, MA). The launch of externally applied RF devices provides the aesthetic physician with one of the most efficient “bulk heaters” of the dermis.
Monopolar, stamping RF is typified by Thermage (Solta Medical, Hayward, CA), a very successful device with modest to good skin-tightening effects, proven in large multicentered trials. Monopolar thermage protocols for treatment of the neck often includes 2 to 3 passes and 2 to 3 treatment sessions separated by several weeks. Combined optical-bipolar RF devices emerged, such as the Refirm and Polaris (Syneron), showing noticeable improvements using multiple-pass, multiple-session treatment protocols. These mono-polar and bipolar RF or optical-RF combination devices, are “stamping” or “static” in nature and often suffer from inadequate dermal stimulation by a combination of very high peak dermal energy (and hence stimulation) but a very short pulse duration, exposing dermal tissue to a relatively short thermal stimulation that would be required for the production of new collagen, elastin, and ground substances. These stamping devices generally deploy protocols with multiple passes and multiple treatments to overcome the ultrashort pulse duration but high temperature model of collagen production stimulation.
More recently, a whole class of transepidermal RF heating devices have emerged that are not short-pulse duration “static” or stamping in nature, but rather, are continuous wave RF systems that are constantly moved along the surface of the skin along a thin layer of ultrasound or some interface gel. The advantage of these “moving” or “dynamic” RF systems is the ability to heat this tissue to a lower temperature but for a much longer period than pulsed mode stamping technologies and, depending on the “moving” device, the therapeutic thermal end point, usually 42°C to 43°C can be maintained, for a very long time. Some of the early “moving RF systems” include the Accent (Alma lasers, Buffalo Grove, IL), Tripolar (Polagen), the diamond polar and Octapolar (Venus Freeze [Venus Concept, Toronto, Canada]), the Excelis (BLT Industries Inc, Framingham, MA), and the 14 and 36 moving bipolar thermally controlled and modulated RF device, called the FORMA (Invasix). The FORMA is a very high tech, thermally modulated enhanced moving RF heating device that has built within the hand piece sensors that measure high and low dermal impedance, epidermal temperature, and electrode contact 10 times every millisecond, and automatically adjusts RF energy depending on the sensory feedback. The FORMA will automatically cut the RF energy off when the therapeutic skin temperature is reached, the impedance drops too quickly (temperature is rising too quickly), or the electrodes lose contact with the epidermal surface. Once the epidermis cools to 0.1°C below the target temperature, the RF energy is turned on again and heating resumes. The FORMA can read, modulate, and automate the high and low temperature extremes, keeping the skin at a very uniform and consistent thermal end point, usually 42° to 43° for prolonged periods of time by this process of thermal modulation and eliminating the “hot spots” that can cause patient discomfort and burns. This thermomodulation process is called ACE, or acquire, control, and extend . The FORMA acquires the dermal-epidermal impedance, contact, and temperature information and will modulate the RF on and off, allowing the patient to experience a long, uniform, and comfortable period at the thermal end point ( Fig. 8 ). As the thermal control is so exquisite, the patient rarely feels a thermal “hot spot” above 42° to 43° and the device burns can be greatly minimized and diminished. Clinical and histologic studies using ACE RF devices have shown good contraction and 14% more new collagen, and 35% collagen synthesis up-regulation.








