Isolated surgery of the neck without a facelift is increasingly in demand and a satisfying option for patients concerned with the aging appearance of the neck. It seems to be requested frequently in men and women and in patients who are satisfied with nonsurgical rejuvenation of the midface or who want to avoid preauricular scars of a facelift operation. Currently, neck surgery probably represents what upper facelift surgery meant to the earlier generation before nonsurgical alternatives were available to treat the midface. A variety of procedures are available from neck liposuction to submentalplasty or a neck lift.
Key points
- •
The neck can be treated independently from the face.
- •
Procedures range from liposuction to Submentalplasty, to a necklift.
- •
The neck lift can be extended to include treatment of the jowls.
Editor Commentary : Alan begins with several quotes that tell denote the importance of the aging neck. He takes us through his algorhythm which may include panfacial rejuvenation based upon the clinical findings. He is willing to perform isolated neck rejuvenation as indicated, but frequently more is required. He also will approach the subject of ancillary procedures such as chin augmentation and partial resection of the submaxillary glands which can have a subtle yet important effect on the final result. This approach cleverly allows the patient to guide the surgeon after being armed with the pertinent information.
Introduction/Overview
“I often do what so many women my age do when in front of a mirror: I gently pull the skin of my neck back and stare wistfully at a younger version of myself.”
“Oh, the necks. There are chicken necks. There are turkey gobbler necks. There are elephant necks. There are necks with waddles and necks with creases that are on the verge of becoming waddles. There are scrawny necks, wrinkled necks, mottled necks. There are necks that are an amazing combination of all of the above. According to my dermatologist, the neck starts at forty-three and that’s that.”
“You can put makeup on your face and concealer under your eyes and dye on your hair, you can shoot collagen and Botulinum Toxin and fillers into your wrinkles and creases, but short of surgery, there’s not a damn thing you can do about a neck. The neck is a dead giveaway. Our faces are lies and our necks are the truth.”
“This is about my neck. And I know what you are thinking: Why not go to a plastic surgeon? I’ll tell you why not. If you go to a plastic surgeon and say, I’d like you just to fix my neck, he will tell you flat out that he can’t do it without giving you a face-lift too. And he’s not lying. He’s not trying to con you into spending more money, The fact is, it’s all one big ball of wax. If you tighten up the neck, you’ve also got to tighten up the face.”
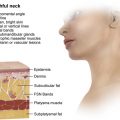
The neck, the region from the jawline to the collarbone and, to some degree, the jowls or what patients may refer to as their chin, is undeniably a common concern for patients. The aforementioned quotes by bestselling author Nora Ephron accurately depict the following about the neck: (1) From the late 30s onward, people invariably pull up on the excess skin, attempting to picture a less-aged version of themselves. (2) It is a telltale, inevitable sign of aging. (3) Unlike the face, there are limited nonsurgical treatments that are beneficial. However, in contrast to Ephron’s last quote, the neck can be isolated from the face and treated independently. This article focuses on the surgical management of the aging neck.
Ellenbogen has described the ideal appearance of a youthful neck. With advancing age, these features inevitably change. Several factors contribute to the senescence of the neck, which have to be analyzed and potentially addressed, including the quality and the quantity of the skin, the subcutaneous and subplatysmal adipose tissue, the status of the platysma muscle (and possibly the digestive muscles), the bony architecture of the mandible, and the submandibular glands. The skin quality is particularly important because no amount of pulling, despite what patients may think, will improve damaged skin. Indeed the swelling of surgery often makes damaged skin look temporarily improved; as that wanes, patients want more surgical tightening in a vain attempt to improve what is actually damaged skin. Furthermore, the relationship with neck aging to the jowls/jawline and the midface should be evaluated, including how full the midface is. Box 1 describes regions related that may or may not be concomitantly addressed at the time of neck surgery.
- •
Submandibular glands
- •
Jowls
- •
Marionette lines
- •
Hypertrophic earlobes
- •
Microgenia
- •
Buccal lipodystrophy
- •
Larynx a
- •
Masseter muscle hypertrophy
- •
Parotid gland enlargement
a Potentially addressed in conjunction with neck surgery.
The consultation begins with a clear understanding of the patients’ concerns (eg, their goals, their dislikes, their tolerance for incisions, how long a recovery period they are willing to accept, and so forth) and reconciling their issues with the surgeon’s physical findings and their anatomy. Periodically, it is prudent to appropriately suggest concomitant related procedures, such as chin enhancement, buccal fat pad removal, or reduction in the salivary gland size, all of which can have a direct impact on the appearance of the neck after surgery. Naturally, the traditional concept of a facelift, which includes the area from cheek to collarbone, is a frequent component of the discussion. With regard to the midface area, patients can be under the misconception that it is necessary to include the midface in the surgical procedure for a neck lift or they may prefer nonsurgical methods (lasers, neurotoxins, or fillers) to improve the face itself. However, for neck laxity, surgical rejuvenation is the only reliable option. In the author’s experience, patients are interested in neck surgery alone because (1) that is all that concerns them, (2) their midface is adequately addressed with nonsurgical treatments, or (3) they prefer not to have the preauricular scar associated with facelift surgery. It is quite clear physiologically and in the judgment of patients that the neck ages differently than the face. Whether or not patients have had facial rejuvenation surgery previously, the neck is usually a significant appearance concern. Consequently, the ability to isolate and surgically treat the neck alone is now an increasingly popular option for patients seeking surgical intervention.
Patients often want to have a preview of the surgical outcome. To experience this, they commonly pull back neck tissue manually in opposing directions with their fingers (the “finger-pull” test). Although helpful in certain circumstances, this can also be misleading, especially if surgery does not entirely eliminate the platysma bands despite how it appears when pulling back on the skin. A more realistic preview may be achieved by looking at themselves in a mirror while lying on their back.
Preoperative planning
Preoperative planning is ultimately a matter of reconciling the patients’ goals with their anatomy. The author explains to patients what their physical findings are and advise them of the role of surgery (addressing skin, fat, and muscle in the neck), the role of nonsurgical procedures (addressing the quality of the skin itself), and the value of topical products. Then the author creates and explains an algorithm to them ( Table 1 ) based on the treatable components of the aging neck and discusses the impact that surgery can be expected to have. The algorithm is essentially that patients with a younger, fattier neck are treated with liposuction ( Fig. 1 ), patients with an early aging neck are treated with a submentalplasty ( Fig. 2 ) (submental incision, liposuction, platysma surgery, and no skin excision), and more advanced patients are treated with a neck lift (liposuction, submentalplasty, and then flap elevation and skin excision) ( Figs. 3 and 4 ). Essentially, each of the 3 common surgical alternatives is cumulative, with each incorporating the earlier technique as they advance from liposuction to a submentalplasty and finally to a neck lift. Despite that algorithm, patients may prefer to downstage their choice of operation to less-invasive options because of a variety of personal concerns. But they should be firmly aware that less-invasive procedures do not yield the same result, understanding that a downstaged, less-invasive procedure can achieve a suitable, albeit less complete, outcome if it coincides with their goals ( Figs. 5 and 6 ).
| Fat | ∗ Muscle | Skin | Treatment |
|---|---|---|---|
| + | No laxity | Adequate | Liposuction |
| + | + | Adequate | Submentalplasty |
| +/– | + | + | Neck lift a |
∗ Visible or lax medial border platysma bands (submentalplasty) muscle treatments include resection, plication (Eiffel Tower), or incising.