Abstract
Reconstruction of soft tissue craniofacial trauma represents a challenging and common problem. The soft tissue structures of the head and neck contain complex 3-dimensional geometry spanning across multiple subunits and structures. Each anatomic region requires careful attention in its repair to meet exacting aesthetic and functional demands. No other region of the body is as scrutinized during social interaction as the face, where even minute deformity is readily detectable at conversational distance. This chapter outlines the proper evaluation and treatment of soft tissue injury across the several subunits of the head and neck. Multiple cases are presented to demonstrate the variety of reconstructive options from simple closure to microsurgical techniques.
Keywords
soft tissue, trauma, primary reconstruction
Background
Reconstruction of soft tissue craniofacial trauma represents a challenging and common problem. The soft tissue structures of the head and neck contain complex 3-dimensional geometry spanning across multiple subunits and structures. Each anatomic region requires careful attention in its repair to meet exacting aesthetic and functional demands. No other region of the body is as scrutinized during social interaction as the face, where even minute deformity is readily detectable at conversational distance.
Craniofacial trauma is common at all ages, accounting for upwards of 7% of patients presenting to adult emergency rooms. Cases of isolated soft tissue craniofacial trauma greatly outnumber cases involving bony injury. Most injuries occur on the forward most projecting surfaces of the head, including the forehead, nose, lips, and chin. Injury types vary from contusions, lacerations to areas of skin, and soft tissue loss. Full-thickness lacerations are most commonly seen and are often small. Left-sided injuries predominate when the cause is an altercation.
The etiology and rates of injury vary significantly with age, sex, and occupation of the patient. In children less than 15 years old the most common cause of injury is falls, with a peak incidence between 1 and 6 years of age. Males are more likely to sustain injury compared to females in this age group. In adults 15–50 years of age, interpersonal violence with assault becomes the most common cause of trauma. Other common causes include motor vehicle collisions (MVCs), sports injuries, and occupational injuries. In this age group males were far more likely than females to present with craniofacial trauma. Over the age of 50 falls again become the main cause of injury, followed by assaults and MVCs.
Surgical Anatomy
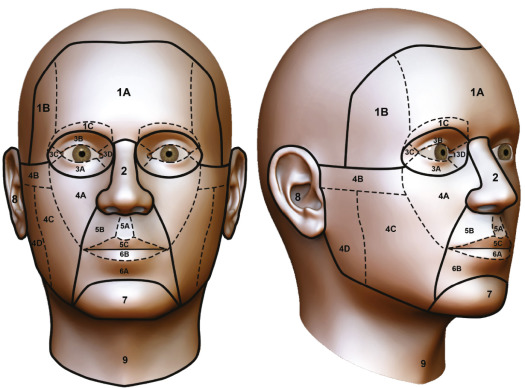
The surface topography of the face, represented by complex 3-dimensional variations in the size, position, proportions, and shape of facial surface contours, defines and characterizes facial appearance. Reconstruction relies on an understanding of subunit classification systems, which serve to describe the extent of injury, and guide surgical management ( Fig. 1.4.1 ). Although many of these classifications were originally developed for extirpative and congenital defects, they are also applicable to the posttraumatic deformity.
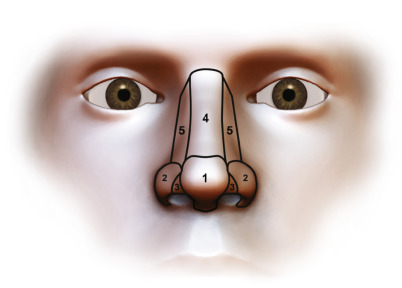
The nasal subunit classification, originally developed by Burget and Menick, is particularly well utilized clinically. It divides the nose into tip, soft triangles, alae, sidewalls, dorsal subunits ( Fig. 1.4.2 ). The underlying principle of nasal subunit reconstruction dictates that defects greater then 50% of a given subunit are best treated with excision of the remaining tissue and reconstruction of the entire subunit. This ensures that subunits or defined surfaces are reconstructed with similar homogenous tissues, while scars are hidden along boundaries or junctions of anatomical units.
Similar to the nose, it is helpful to think of reconstruction of the perioral region based on aesthetic subunits and anatomic layers ( Fig. 1.4.1 ). Although excision of the remaining subunit can minimize visibility of scars, compromise is often required. This is especially true in traumatic injuries where aggressive use of flaps may not always be an option due to the zone of injury and questionable tissue viability. It is important to understand the cross-sectional anatomy of the lips and the relationship of the orbicularis muscle, white roll, and location of the labial arteries, which run just deep to the muscle at the wet dry vermillion junction.
The case illustrated in Fig. 1.4.3 demonstrates the utility of the subunit principle. Initially the remaining lip is significantly splayed, making it difficult to assess the true defect. Repositioning the lateral lip segments to their natural position allows for proper assessment of the remaining subunits. A lip switch flap was chosen to reconstruct the lip defect and nasal sill. Note that the flap design maintains the integrity of the labiomental crease and leaves the chin intact. A full-thickness graft provides coverage for the columella and a composite graft from the right ear is used for the alar defect.

Knowledge of surface anatomy plays an important role in diagnosing damage to vital structures such as the facial nerve, trigeminal nerve, and Stenson’s (parotid) duct. This is demonstrated by the patient in Fig. 1.4.4 , who sustained a full-thickness laceration across the cheek with exposure of the mandible. The relative positions of the facial nerve branches and parotid duct are depicted. The frontal branch of the facial nerve has multiple branches that cross the central third to half of the zygomatic arch. Cephalad to the zygomatic arch these branches run in a plane just deep to the temporoparietal fascia. At the level of the zygomatic arch the temporal branch is found in a deeper plane directly adjacent to the periosteum. The zygomatic and buccal branches of the facial nerve exit the parotid and run in a plane deep to both the SMAS (superficial musculoaponeurotic) and parotid masseteric fascia. They then travel through the buccal space and go on to innervate the facial musculature on their undersurface. Significant arborization occurs between the terminal zygomatic and buccal branches, and because of this spontaneous recovery from injury is commonly seen. Exploration and attempted repair of these branches medial to the lateral canthus is not recommended due to their small size and chance for spontaneous recovery. The marginal mandibular branch of the facial nerve has been extensively studied and most often its course remains above the inferior border of the mandible. However, the nerve can travel from 1–3 cm below the inferior edge in some individuals, specifically in the region between the mandibular angle and the point the nerve crosses superficial to the facial vessels. After exiting the caudal parotid the nerve travels in a plane deep to the parotid masseteric fascia, crosses superficial to the facial vessels and then pierces the deep cervical fascia to innervate the lower lip depressors and mentalis.
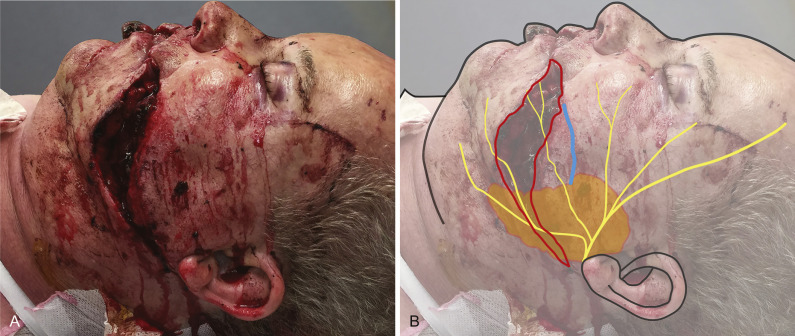
The parotid duct exits the anterior edge of the parotid gland roughly at the level of the tragus and initially runs on the anterior surface of the masseter muscle. At the anterior edge of the masseter it passes through the buccal fat pad and pierces the buccinator muscle to emerge into the oral cavity adjacent to the 2nd maxillary molar. It is approximately 7 cm in length. The superficial landmark for the path of the duct is a line drawn between the tragus and the midline of the lip ( Fig. 1.4.4 ). Any laceration deep to the SMAS in this region should prompt further investigation into parotid duct integrity.
Clinical Presentation
The initial presentation of patients with soft tissue facial trauma will vary significantly depending on mechanism and extent of injury. The Advanced Trauma Life Support (ATLS) protocol should be used to efficiently evaluate and stabilize all major trauma patients. Thorough history should first be obtained, including details relating to timing, mechanism, location of incident, and the degree of contamination. Any dangerous mechanisms of injury such as fall from elevation (3 feet, 5 stairs), high speed MVC, rollover or ejection should prompt further evaluation for possible brain and C-spine injury. The mechanism also provides useful information on the zone of injury and risk to underlying structures. For example, even small sharp lacerations may penetrate deeply and injure vital structures, and when found in critical areas must raise suspicion. In the case of ballistic trauma, information should be obtained on the gun as well as the projectile characteristics (velocity, shape, and mass) and the firing range.
In the case of an animal bite, attention should be paid to whether the attack was provoked or unprovoked, the immunization status of the animal, and if the animal has been detained, monitoring for developing signs of rabies. Due to the widely varying incidence and risk of rabies from animal bites, any concern in this regard should prompt a consult to the infectious disease service or public health medical officer.
Classifying traumatic wounds as either clean or dirty helps to determine need for prophylactic antibiotics and tetanus treatment. Clean traumatic wounds or lacerations are those without evidence of macroscopic contamination or signs of infection and do not require prophylactic antibiotic treatment. This is especially true in craniofacial trauma where the soft tissues are highly vascularized. Dirty traumatic wounds include those with macroscopic contamination, with devitalized tissue, caused by animal bites, or occurring in a contaminated environment. Prophylactic antibiotics should be used in most dirty wounds. Tetanus immunization status should be assessed in every patient as all wounds are potentially at risk. If vaccination history is unknown, less than three doses have been received or it has been more than 10 years since the last dose of tetanus vaccine, a booster should be given. If the wound is not considered clean, then tetanus immunoglobulin should also be given to these nonimmune patients.
Physical exam should be approached in a systematic way, from the top of the head down. Each site should be assessed for possible embedded foreign body, glass or particulate matter. The scalp is a common location of missed lacerations due to the obstruction of hair. Palpation over the entire scalp should be performed, examining for obvious lacerations or areas of dry blood and matted hair. Scalp lacerations have significant risk of prolonged bleeding due to the rich vascular supply and the lack of retraction due to the galea aponeurosis. Untreated scalp lacerations are a known cause of hemorrhagic shock and can be fatal.
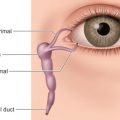
Examination of the periorbital region should focus on each structural region to avoid missing subtle injuries. Depth of laceration and involvement of the lid margin should be noted. Orbital fat observed in the wound is a sign of violation of the orbital septum and possible injury to underlying structures such as the globe and levator palpebrae superioris. If there is injury to one or more of the lids then associated injury to the globe must also be ruled out with suspected injury prompting an immediate consultation with ophthalmology. Assessment of the lacrimal system, levator palpebrae function, and medial and lateral canthal tendon integrity should also be assessed. Testing the integrity of the lacrimal system in traumatic injuries is usually done simply by probing of the lacrimal system and examining for defects. In children, lacrimal probing is usually not tolerated without sedation and so a Jones 1 test with fluorescein placed into the conjunctival fornices can be performed. If fluorescein is detected under the inferior nasal meatus, the drainage system is likely intact.
Exam of the traumatized nose must include inspection of both the external and internal structures. Integrity of the external skin, the cartilaginous and bony supporting structures, and the internal lining must be examined. Specific care should be taken to rule out a septal hematoma due to the devastating consequences of septal necrosis and secondary nasal collapse. This can occur after even minor trauma, especially in children where the softer cartilage is more easily deformed. Damage to the septal cartilage can occur within 24 hours and necrosis between 72–96 hours if not treated. On intranasal examination, a septal hematoma will appear as a bulging, boggy, ecchymotic mass often causing obstruction bilaterally, as seen in Fig. 1.4.5 .

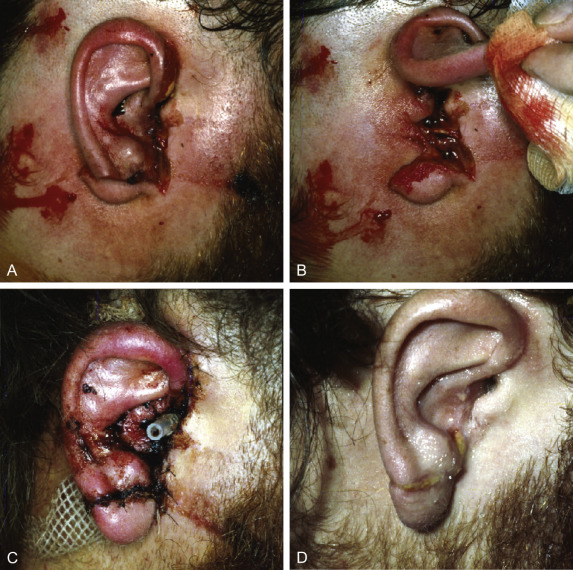
Examination of the ears should assess both the anterior and posterior surface for lacerations and signs of hematoma. Auricular hematoma seen in blunt trauma carries the risk of developing cauliflower ear if not identified and treated. Lacerations should be assessed for involvement of the underlying cartilage framework. If there is extension into the external auditory meatus, as seen in Fig. 1.4.6 , otoscopy should be performed to rule out damage to middle ear structures. Penetrating or ballistic injuries in this area can also cause damage to the facial nerve trunk, and its intratemporal course, therefore its integrity must be assessed.
Lacerations and injury to the lips should be evaluated for the extent of tissue loss and which subunits are affected. Intraoral examination should follow to assess for through-and-through lacerations, and associated injury to the buccal mucosa or tongue.
Lacerations overlying the path of the facial nerve (described previously) require careful examination to rule out damage to one or more of its branches. The location of the laceration is important clinically because damage to buccal or zygomatic branches medial to the lateral canthus are generally not repaired due to the small size and high rate of crossover between the facial nerve branches, leading to spontaneous recovery. Each facial nerve innervated muscle should be tested and compared to the uninjured side if possible. Any weakness should be documented with a systematic top-down approach. If nerve laceration is suspected on examination, early operative exploration is indicated. Early recognition is essential as locating the distal cut ends of the nerve is much easier within the first 2–6 days following injury before the distal nerve undergoes Wallerian degeneration and can no longer be stimulated. Sensation in all distributions of the trigeminal nerve should also be assessed and documented during the initial examinations.
The course of the parotid duct follows a line from the tragus to the upper lip cupid’s bow, with the duct entering the oral cavity adjacent to the maxillary second molar. Exploration should be performed to determine the extent and location of damage to the duct and gland. Cannulation of the duct intraorally with a lacrimal probe or angiocath (angiocath can be left in situ to stent the subsequent repair) can be helpful in diagnosing an injury on exam.
Penetrating neck injuries (PNI) are potentially life-threatening secondary to hypovolemic shock and airway loss. Hard clinical signs of major vascular injury include severe active bleeding, rapidly expanding hematoma, hypovolemic shock not responsive to fluid resuscitation, and diminished radial pulse. In the case of a hemodynamically unstable patient, resuscitation following the ATLS protocol and emergent surgical exploration should be carried out. Some centers will attempt Foley catheter balloon tamponade before operative exploration, and if successful, follow with angiography. In the case of a hemodynamically stable patient with PNI, monitoring for at least 24 hours and possible CT angiography should be carried out.
Radiological Evaluation
Radiological investigation in facial trauma usually focuses on the underlying bony skeleton with high-resolution CT being the primary modality. Soft tissue structures can also be assessed on these scans, revealing depth of injury, involved structures, the presence of radiopaque foreign bodies or hematoma. If an infused scan is performed, the presence of active extravasation can also be assessed. In the case of soft tissue injuries with secondary infection and abscess, CT provides useful information of size and location which can guide surgical management.
CT imaging may not be sufficient if there is concern for retained foreign body with low radio density such as wood or plastic. MRI can detect these materials, however access to this modality is often limited. Ultrasound is readily available and it has increasingly been used in the detection of radiolucent materials. Most often, detailed physical examination and exploration of the wound with magnification are all that is required.
Sialography can be used in the diagnosis of parotid duct injuries, however it is rarely performed as most injuries are readily diagnosed on examination and exploration. If a duct injury is suspected in a small but penetrating injury, sialography may be useful in avoiding an operative exploration that would put adjacent facial nerve branches at risk.
Classification of Soft Tissue Injuries
Contusion and Hematoma
Blunt soft tissue injuries can result in diffuse damage to the subcutaneous tissues without overt damage to the skin. This mechanism can result in fat necrosis with eventual depression and contour irregularity. Contusions resulting in significant hematoma can exaggerate this effect due to the elevated pressure placed on the soft tissues. Hematomas are best drained immediately before they coagulate, otherwise a small stab incision or delayed drainage will be required.
Abrasive Injuries
Abrasive wounds are diffuse injuries caused by motion across an irregular surface. Typically, these are superficial injuries without exposure of the underlying subcutaneous tissue. Depending on the mechanism and abrasive surface there could be significant embedded dirt, foreign body, and loose devitalized skin which should be removed with scrubbing and debridement. This should be performed before healing of the tissue entraps the particles leading to traumatic tattooing. The Versajet hydrosurgery system has been successfully used for this purpose, and may facilitate the process by providing a finely tunable debridement. Healing of partial-thickness wounds of this type will occur within 2 weeks with proper wound care, including gentle cleansing and light, greasy dressings. Deep partial-thickness wounds need careful consideration of their healing potential as prolonged healing will greatly increase the risk of scarring. If healing is not expected to occur within 3 weeks, consideration should be given to definitive debridement and grafting.
Lacerations
Lacerations can range from simple clean-line cuts caused by sharp mechanisms, to stellate bursts from blunt force or ballistic mechanisms, causing tearing of skin. The trauma mechanism will affect the zone of injury, with blunt or tearing forces resulting in diffuse damage to the skin and soft tissues with the possibility of an underlying hematoma. Although clearly devitalized tissue should be removed, the generous blood supply to facial soft tissues allows for conservative debridement. All irreplaceable tissues, such as those of the lip, should be given a chance to declare themselves as they may survive on even small vascular pedicles. When tissues have undergone diffuse damage, and viability is questionable, the objective should be to close the wound in as simple a manner as possible to avoid additional stress on the tissues. To achieve this the smallest number of sutures possible should be used and tissue rearrangement should be avoided during the initial closure.
In simple lacerations without diffuse damage, revision of the wound edges during the initial closure can be considered to potentially avoid the need for secondary revision. This is applicable in hyper-beveled lacerations that would result in overriding edges, or lacerations with ragged edges or multiple parallel cuts. Trapdoor scars occur in curvilinear and U-shaped lacerations and result in raised areas secondary to circumferential contraction. Immediate or early Z-plasty to break up the contracting forces can be considered.
Avulsive Injuries
Partial soft tissue avulsions of facial tissues have the advantage of the generous blood supply of the head and neck region. Avulsed tissue maintained on small pedicles can survive, however closure must not impair tissue vascularity. The treatment of venous congestion in partial avulsion injuries with medicinal leeches has been shown to be effective. Brisk arterial inflow into the part should be confirmed prior to leeching. If arterial inflow is compromised, arterial microvascular repair should be considered.
Avulsive injuries that result in exposure of critical structures require immediate resurfacing with vascularized tissues. Reasonable options include local flaps, galea frontalis flap, or temporalis muscle flap.
The patient in Fig. 1.4.7 presented as a cyclist involved in an MVC. He sustained a Manson Type II naso-orbito-ethmoid fracture, nasal bone fracture, and avulsive injury resulting in a glabellar defect. Coverage of the bony structures and fixation hardware was achieved using a galeal frontalis flap pedicled on the right supratrochlear vessels with application of a full-thickness skin graft.

Related posts:
 Assessment of the Patient With Traumatic Facial Injury
Assessment of the Patient With Traumatic Facial Injury
 Frontal Bone and Frontal Sinus Injuries
Frontal Bone and Frontal Sinus Injuries
 Le Fort Fractures
Le Fort Fractures
 Secondary Reconstruction of Facial Soft Tissue Injury and Defects
Secondary Reconstruction of Facial Soft Tissue Injury and Defects
 Geriatric and Edentulous Maxillary and Mandibular Fractures
Geriatric and Edentulous Maxillary and Mandibular Fractures
 Secondary Microvascular Reconstruction of the Traumatic Facial Injury
Secondary Microvascular Reconstruction of the Traumatic Facial Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


