Abstract
Patients with facial injuries often have multisystem involvement, and the initial assessment of the trauma patient should be consistent with the ATLS (Advanced Trauma Life Support) protocol. Although traumatic facial injuries are rarely life-threatening, the examiner must pay close attention to facial injuries that may cause airway compromise, severe hemorrhage, cervical spine injuries or central nervous system injuries. After the patient is determined to be hemodynamically stable, the secondary survey will focus on any facial lacerations, avulsions, contusions, bony disruptions, vision changes, malocclusion, and trismus. The goals of this chapter are to highlight (1) the common patterns of facial trauma and relevant soft tissue and skeletal anatomy, (2) the importance of organized, systematic approach to physical examination with the aid of radiological imaging, (3) the various considerations in the setting of concomitant multisystem injuries, and (4) the various surgical exposures of the craniofacial skeleton for definitive surgical treatment.
Keywords
maxillofacial trauma, facial, trauma, injury, assessment
Background
Incidence of Facial Trauma in the United States and Worldwide
The spectrum of facial trauma includes soft tissue and bone, and ranges from the simple to the complex. Epidemiology varies with local and global demographic factors and reflects a complex interplay of influences, including those related to the environment, economics, age, gender, and mechanism of injury. Any understanding of the incidence of facial trauma is further confounded by the presumptive underreporting and treatment of minor injuries. As a result, the plethora of data is often conflicting. Nonetheless, the incidence of facial fractures presenting to the emergency room is approximately 500,000 per year in the United States, with nasal fractures likely the most common, followed by mandible fractures. These commonly occur in males more than females, are most frequent in the second and third decades of life, and are most frequently the result of altercations, assaults, falls, work or home accidents, and motor vehicle or motorcycle collisions (MVCs). While many studies cite mandible fractures as being more common than nasal fractures, this has been attributed to a sampling bias favoring inpatient admissions or requirement for in-hospital treatment rather than capturing all emergency room presentations. Several older studies show higher rates of injury from MVCs, prior to the mandatory implementation of airbags and restraining devices. Despite this, MVCs remain the most important cause of facial trauma all over the world. Global trends also reflect an increase in the male/female injury ratio in countries where the social custom is for women to be more confined to the home. Associated soft tissue trauma is the most common concomitant injury, occurring in approximately 30% of facial fractures. Concomitant fractures of the skull, upper limbs, and associated areas are estimated to occur in around 25% of facial fractures; these include intracranial injuries in 12%–45.5%, and associated cervical spine injury with facial injury in up to 9.7%. One must therefore always exclude brain and cervical spine injuries in the patient with facial injuries as trauma is often a geographic injury to the head and neck. Missed injuries of the spine, extremities, and pelvis are also frequent (10%) and are easily missed.
Patterns of Facial Trauma and Causes
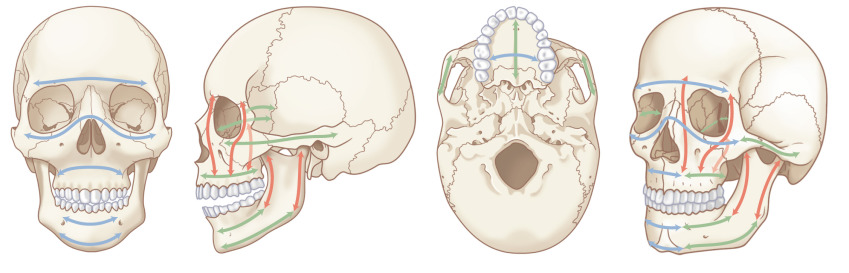
Patterns of facial injuries may be subdivided into soft tissue, bony skeleton, and/or dentoalveolar trauma. Descriptions can also be made based on location in facial thirds: the upper third (including the frontal bone, frontal sinuses, and orbital roofs), middle third (including the orbit, nose, malar region, and maxilla), and lower third (including the mandible and its dentition) ( Fig. 1.1.1 ). Blunt trauma can result in relatively predictable fracture patterns due to the presence of facial buttresses and resultant functional skeletal units ( Fig. 1.1.2 ). Injury to the upper third may reveal frontal sinus fractures, which require the determination of whether injury affects the inner table, outer table, or both, degree of displacement, and the presence of nasofrontal outflow tract obstruction. Midface fracture patterns may include the characteristic Le Fort fracture patterns, but are more frequently asymmetric and more extensive on the side of the force application, or orbitozygomaticomaxillary complex (OZMC), orbital, nasal and naso-orbito-ethmoid (NOE) fractures in isolation or in combination. Lower third facial fractures, i.e., those of the mandible, also demonstrate reproducible patterns. The most prevalent site of mandibular fracture reported in the literature is variable, though mandibular angle and condyle are the most frequently cited. Based on the mandibular “ring” concept, mandibular fractures have conventionally been thought to involve at least two sites, however, unifocal mandibular fractures commonly occur. Common multifocal patterns include mandibular body and contralateral angle/ramus/condyle, angle and contralateral parasymphysis, symphysis/parasymphysis, and bilateral condyle. True panfacial fractures involve all thirds of the face simultaneously and are less involved on the contralateral side, both in terms of fracture extent and comminution. These fracture patterns differ depending on mechanism, with most panfacial fractures usually resulting from MVCs and, less commonly, from gunshot wounds (GSWs). Sports injuries typically are isolated to the mandible or upper midface, and assaults are predictive of isolated mandible, midface or zygoma fractures. MVCs and GSWs each predict a higher severity of injury than assaults, falls, or sports injuries.

Patterns of facial trauma in the pediatric population differ from those in adults. Facial fractures are relatively less common in children due to parental supervision as well as intrinsic anatomical factors such as larger fat pads, decreased pneumatization of sinuses, increased skeletal flexibility secondary to more malleable bone stock, and compliant sutures. The large cranium partially shields the rest of the face from injury. Atypical craniofacial fracture patterns precede the Le Fort patterns seen in adulthood and as an incompletely pneumatized frontal sinus transmits energy directly from the site of impact to the supraorbital foramen and then to the orbit, superior NOE and anterior maxillary wall or zygoma. Younger patients are at higher risk of dentoalveolar trauma, including crown fractures (the most common injury), luxations, avulsions, subluxations, root fractures, and intrusions, with approximately one-third occurring in those younger than 10 years of age. These most often result from activities of daily living, play, MVCs, and sports.
The relative incidence of fracture patterns is debated; mandible fractures are often cited as the most common pediatric facial fracture, accounting for 20%–50% of all pediatric facial fractures. Anatomical distribution varies with age; isolated condylar fracture incidence decreases, while body and angle fractures increase. Others have reported that nasal fractures comprise up to 50% of pediatric facial fractures, but usually escape hospital registries. Nasal and maxillary fractures were the most common osseous injuries among infants in the US National Trauma Databank, while mandible fractures were more common in older teenagers, with mandible fractures being the overall most common facial fracture. Nasal fractures are likely often underreported, with many treated as an outpatient or not treated and thus not reported. One review found 54% of fractures to occur in the skull, one-third in the upper and middle thirds of the face, and the remainder in the lower third. Another group stratified patients by dental maturity – primary, mixed, and permanent dentition – and concluded orbital fracture was the most common fracture type for all age groups combined. This group showed activities of daily living as the most common cause of injury in 0- to 5-year-olds, MVCs, sports, and play in ages 6–11, and violence, sports, and MVCs as the most common causes of injury in 12- to 18-year-olds.
Similarly, fracture patterns, demographics, and mechanisms of injury differ significantly between geriatric and nongeriatric adult craniofacial trauma patients. Falls are more frequent causes of fractures in geriatric patients whereas assaults, MVCs, and pedestrians struck were significantly more frequent causes in the nongeriatric adult population. Mandible fractures and panfacial fractures are more common in the nongeriatric population while higher incidences of orbital floor, maxillary, and condylar fractures are more common in geriatric patients and are dependent on geriatric age status, rather than mechanism of injury alone. The most common cause of soft tissue injury has been shown to be falls and therefore older people seem excessively prone to this injury.
Penetrating soft tissue trauma, including that resulting from bites, stab wounds, gunshot, and other ballistic injuries, can result in injury configurations and fracture patterns that fall outside the usual predictable blunt trauma patterns. Distribution of soft tissue injury is frequently concentrated in a “T-shaped” area that includes the forehead, nose, lips, and chin as well as commonly affecting the lateral brows, malar eminences, forehead, and occiput. Patterns may be described by facial aesthetic units or in reference to bony landmarks. Depth and structures suspected to be injured are also important considerations, especially the globe, eyelids, canthi, lacrimal system, lips, nose, facial nerve, and parotid duct. Ballistic injuries including GSWs are further uniquely characterized by blast vasospasm. These may be further complicated by a combination of blunt, penetrating, and burn injuries.
These patterns of injury and interplay with epidemiology, mechanism, and patient demographics emphasize the importance of a meticulous history and a sequential and directed physical examination as central to the evaluation of a patient with facial trauma. This process collects information that predicts the injury pattern, which is further documented by examination and radiographs to serve as a basis for diagnosis and management.
Surgical Anatomy
Facial Soft Tissue Anatomy
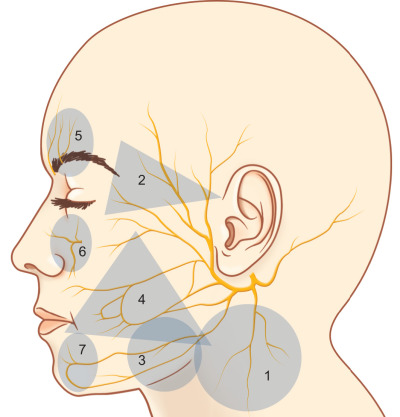
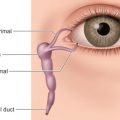
Knowledge of the functional anatomy of the face is fundamental to the understanding of facial trauma management. Important soft tissue considerations are the exact locations of the unique structures of the face and their relations to aesthetic units, layers of the face, and surface landmarks of deep structures such as the lacrimal system, Stenson’s duct, and neurovascular networks, including facial nerve “danger zones” ( Fig. 1.1.3 ). The eyelids, nose, ears, and lips are unique structures of the face. A detailed description of their component tissues is beyond the scope of this chapter but an appreciation of this detailed anatomy is vital for reapproximation, repair, and reconstruction following injury and is found in individual sections dealing with regional areas. Similarly, aesthetic facial subunits and the lines of skin tension (Langer’s lines) can help guide soft tissue repair strategy. The tenet from tumor surgery that loss of more than 50% of a subunit requires consideration of excision of the remainder of that subunit and reconstruction of it as a whole should be considered, but may not be as valid in youth or in cutaneous facial injury. The soft tissue planes of the face from superficial to deep are skin, subcutaneous fat, superficial musculoaponeurotic system (SMAS), containing mimetic muscles, deep fascia and fat compartments, and periosteum. The lacrimal system is the apparatus that produces tears and manages their transfer and drainage; it extends from the lacrimal gland in the lateral upper eyelid, over the corneal surface to the lacrimal canaliculi, through the lacrimal sac and the nasolacrimal duct to the inferior meatus of the nose. Injuries in the region of the eyelids, medial canthus, and upper lateral posterior nasal region should raise suspicion of potential injury to these structures. Stenson’s duct is the conduit for saliva from the parotid gland to the mouth, emerging at a papilla adjacent to the second maxillary molar. An evaluation of Stenson’s duct integrity is important in deep lacerations of the central cheek (especially those that occur near a reference line from the tragus to the lateral oral commissure). Sialocele, fistulae, and infection follow duct or gland injury. The trigeminal nerve branches that supply sensory innervation to the face may be injured as they exit bony foramina approximately in line with the mid-pupil, the supraorbital foramen/notch, infraorbital foramen, and mental foramen for the three principal sensory branches of V 1 , V 2 , and V 3 respectively. The blood supply to the face is exceedingly robust and focal injury of single vessels rarely results in clinically significant tissue ischemia in otherwise virgin tissue due to efficient and profuse collateral supply. Injury to the facial artery and its branches such as the labial arteries of the lips, the superficial temporal artery, angular vessels and its other branches can cause significant bleeding and, if untreated, near exsanguination. Identification of foci of blood loss, along with ability to control epistaxis, are essential for control of bleeding from facial injuries as discussed further below. Facial nerve deficit can be one of the most devastating ramifications of an injury to the face. While the facial nerve can be injured anywhere along its course, there are “danger zones” where it is particularly vulnerable to injury; the temporal branch along Pitanguy’s line (from 0.5 cm below the tragus to 1.5 cm above the lateral eyebrow), the zygomatic and buccal branches around Zuker’s point (halfway point along a reference line from the helical root to the oral commissure), and the marginal mandibular branch overlying the inferior mandibular body border. Nerve injuries medial to the lateral canthus are less clinically significant due to arborization of the nerve, but any cut nerve seen should be repaired. For those more proximal branches, operative exploration and repair within 72 hours optimizes recovery of motor function.
Facial Skeletal Anatomy
The structural support of the facial skeleton may be organized by the description of the facial buttresses. Nasofrontal/nasomaxillary, zygomatic, and pterygomaxillary buttresses are the major structures of vertical support of the maxilla; mandibular, maxillary–palatal, zygomatic, and frontal buttress are responsible for anteroposterior projection; and the orbital buttress has both vertical and horizontal components (see Fig. 1.1.2 ). These are the supporting pillars of the facial skeleton; alignment and stabilization following injury literally provides the bony foundation for the restoration of facial form and support.
Adult and Primary Dentition and Nomenclature
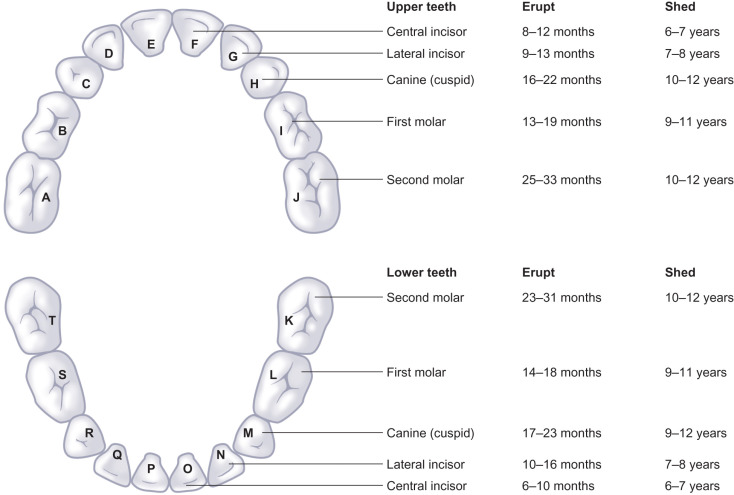
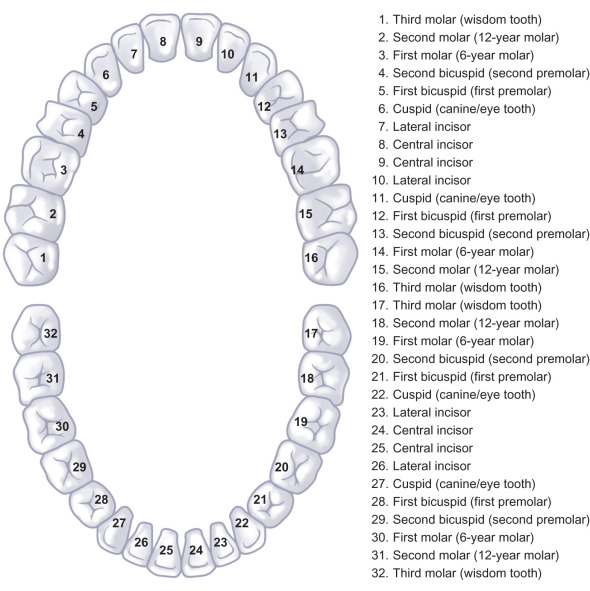
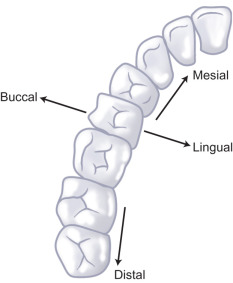
Assessment of dental trauma requires fluent knowledge of the nomenclature of dentition, both adult (permanent) and primary (deciduous) teeth. There are 20 primary teeth denoted by letters A to T proceeding from upper right second molar (A), to upper left second molar (J), then lower left second molar (K) to lower right second molar (T) ( Fig. 1.1.4 ). Similarly, permanent teeth are denoted by numbers 1–32 from upper right third molar (1) to upper left third molar (16) and then lower left third molar (17) to lower right third molar (32) ( Fig. 1.1.5 ). The mandibular first molar is the first permanent tooth to erupt, typically at 6 years, followed by incisors at age 6–9, then canines between 9 and 12 years, first premolars at 10–11, second premolars at 11–12, second molars at 11–13, and finally third molars around 17–21 years of age. There is specific anatomical terminology for orientation when referencing teeth, namely mesial (towards midline) and distal (away from midline) in reference to the dental arch, as well as lingual (towards tongue)/palatal (towards palate) versus buccal (towards cheek), labial (toward the lip) ( Fig. 1.1.6 ).
The practical application of the anatomy of the soft tissue, osseous, and dentoalveolar structures enables accurate diagnosis and nomenclature of facial injury, forms the basis for surgical exposure of the craniofacial skeleton, and as such is the cornerstone of fracture management. Incisions and exposures must be designed to respect aesthetic units, navigating the various layers of the face without injury to vital structures, preserving nerves and vessels to expose underlying fractures and skeletal buttresses.
Classification
There is no widely adopted classification of facial trauma that encompasses all of the soft tissue, dentoalveolar, and bony injuries. Rather, certain injury patterns do have well described and accepted classification systems, such as Le Fort fractures, NOE fractures, and dentoalveolar fractures, and each will be discussed below. Facial injuries are usually classified descriptively and largely by pattern. Soft tissue injuries may be classified by descriptions of their mechanism (sharp, crush, ballistic, blunt, burn), laceration and/or avulsion, location, orientation (vertical, transverse, oblique), and depth. In general, fractures can be classified by pattern: location, displacement, comminution, and whether they are open/closed to the skin. Most commonly, facial fractures are classified as being upper, middle or lower third (i.e., mandible) fractures or a combination; a true “panfacial” fracture has components involving upper, middle, and lower thirds simultaneously.
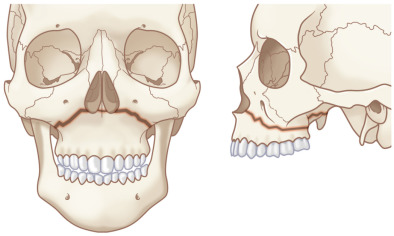
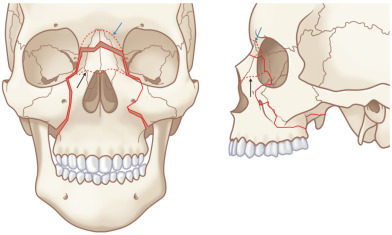
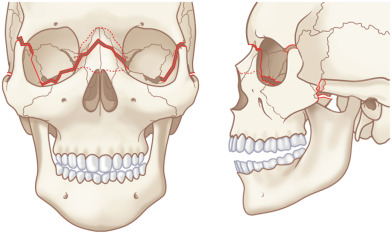
The Le Fort classification is a widely adopted and historical description of midface fracture patterns and fracture line locations in the maxilla with strong historical roots to original French cadaver experiments. The hallmark of Le Fort fractures is traumatic pterygomaxillary separation , which signifies fractures of the pterygoid plates. Le Fort Type I fractures involve the lateral and medial walls of the maxillary sinus, propagating posteriorly above the alveolar process from the pyriform aperture ( Fig. 1.1.7 ). Le Fort Type II fractures extend through the inferior orbital rim and orbital floor and the maxillary sinuses, and across the nose either high or low, forming a pyramidal shape of varying heights ( Fig. 1.1.8 ). Le Fort Type III fractures extend horizontally from the nasofrontal suture to the frontozygomatic suture, through the orbits, and transect the zygomatic arches ( Fig. 1.1.9 ). Le Fort I, II, and III fractures are conceptualized as a “floating palate,” “floating maxilla,” and “craniofacial dysfunction,” respectively. Most Le Fort fractures are usually bilateral, but asymmetric due to the asymmetric forces creating the fracture. It is thus common to have a higher-level fracture (i.e., Le Fort III) on the side of force application, and a lower-level fracture (i.e., Le Fort II) on the contralateral side. Lesser Le Fort segments usually exist within the overall Le Fort fracture pattern, reflecting comminution. Accurate bilateral description of the fracture pattern is critical for planning of the open reduction. The fracture pattern is defined by stating the highest level of Le Fort fracture on each side up to (and including) the frontal bone and the nature of the fragment that includes the maxillary dentition (i.e., dentoalveolar fracture, split palate). The Le Fort fracture pattern is thus precisely defined and guides the surgeon where open reduction should be performed.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


