Abstract
Fractures of the edentulous jaws are commonly seen and present unique challenges to the treating surgeon. Treatment of these injuries has evolved over the years as the experience with rigid fixation techniques has improved. Rigid fixation principles applied to the management of edentulous jaw fractures have improved our surgical outcomes and improved care for the patient.
Keywords
fracture, edentulous mandible, edentulous maxilla, rigid fixation
Through medical advances, the world’s population is living longer and the geriatric age group is increasing. Edentulism is often associated with the geriatric population. Edentulism is defined as the condition of being without natural teeth. The edentulous population statistics are difficult to interpret fully and are related to multiple factors, including socioeconomic status. The rate of edentulism appears to be declining in the United States, however there are regions with high rates of edentulism, sometimes greater than 20% of the population. There is an estimated 12.2 million edentulous population in the United States in the 2009–2012 survey.
The edentulous population is subject to the same mechanisms of trauma as the rest of the population. Motor vehicle collisions, assaults, and falls account for the majority of maxillofacial trauma seen in the geriatric population.
Diagnosis
A thorough physical exam should be performed on all maxillofacial trauma patients. Indicators of bony trauma and fracture are similar between edentulous and dentate patients.
- 1.
Facial deformity
- 2.
Ecchymosis
- 3.
Mobility of segments and pain
- 4.
V3 paresthesia in the mandible
- 5.
V2 paresthesia in the maxilla
- 6.
Malocclusion if dentures are in place


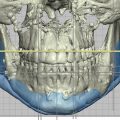
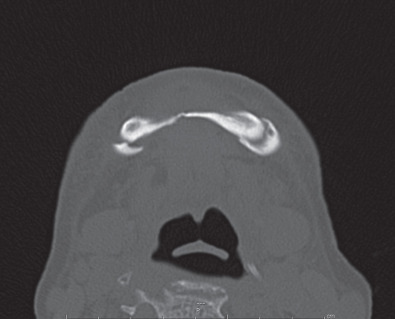
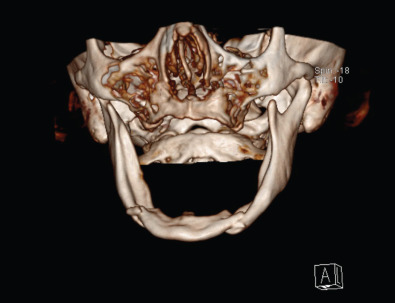
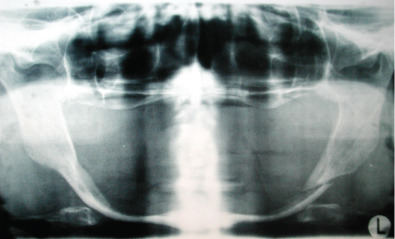
If maxillofacial trauma is suspected, radiographs will most likely be performed. Plain films of the maxillofacial region such as the mandible series, Waters view and submental vertex view are almost always now being replaced by the computed tomography (CT) scan. CT scans of the maxillofacial region give much better detail in a 3-dimensional aspect to assist the provider in diagnosing the injury and formulating a treatment plan. Occasionally, patients seen in the outpatient office will have an orthopantomogram (panorex) as a screening film for mandibular trauma. The orthopantomogram should have another radiograph in a second plane such as an AP film or CT scan to fully assess the injury. A CT scan is the optimal study to assess maxillary and upper face trauma. Additionally, the CT scan can be carried through the skull to assess bony and soft tissue injuries to the central nervous system and cervical spine ( Figs. 1.21.3–1.21.6 ).

The basis for treatment of maxillofacial trauma for hundreds of years has been to “put the teeth together and the bones will follow.” This is the rationale for the classic closed reduction of mandible and maxillary fractures with intermaxillary fixation. The teeth will heal in the correct occlusion and the bony fractures will remodel over time to correct any residual bony deformity. Edentulous patients by definition do not have any natural teeth which causes a problem with the basics of treatment.
There are multiple options to treat edentulous fractures of the jaws. One option is to maintain a dental soft diet. This option is best for minimally displaced fractures or a patient who is medically unfit for surgery. There is the obvious potential for the patient to go on to a nonunion or malunion, both of which would be considered complications in the management of the patient. The atrophic edentulous mandible fracture patient has a high complication rate of nonunion at approximately 20%.
Mandible Fractures
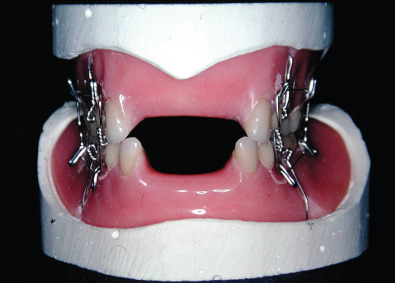
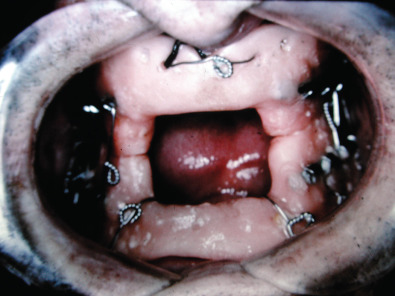
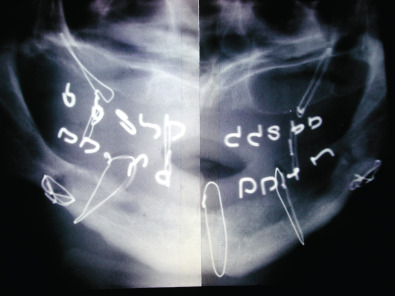
Historically, edentulous mandible fractures were treated by closed reduction. This required altering the patient’s denture and fixating the dental prostheses to the patient’s jaws and using postoperative maxillomandibular fixation (MMF). Alternatively, dental splints could be fabricated and secured to the patient and postoperative maxillomandibular fixation could be used. The dental splints could be one- or two-piece constructs. The one-piece constructed dental prosthesis is known as the Gunning splint. Treating edentulous mandible fractures with dental prostheses required additional knowledge not available to all surgeons managing facial fractures. A dental laboratory facility needed to be available in order to fabricate the acrylic prostheses after dental models had been obtained. This could be cumbersome, time-consuming and delay patient care. Additionally, the patient’s postoperative course was very difficult because of the dental appliances fixated to their jaws and the postoperative MMF. External fixators have also been used to stabilize edentulous mandible fractures as there are no teeth present. Precise anatomical reduction is often difficult with external fixators, especially in the atrophic mandible fracture with reduced bone stock. Management of edentulous mandible fractures by closed reduction techniques was difficult for the patient and had a high complication rate of nonunion ( Figs. 1.21.7–1.21.11 ).


Open reduction techniques then evolved in management of edentulous mandible fractures. Osteosynthesis was accomplished using stainless steel wire, K wires, and finally miniplates. Often, postoperative MMF was still required as the fixation was not strong enough to withstand the forces of mastication or the pull of muscles attached to the mandible. The open reduction techniques using wire, K wires, and miniplates still had an unacceptably high complication rate.
Contemporary management of edentulous mandible fractures is best accomplished with open reduction and internal fixation of the fracture with a stable plate, usually a locking reconstruction plate. This permits anatomical reduction of the fracture with fixation that can withstand the forces of mastication and no postoperative MMF. The treatment does not require use of dental prostheses, dental consultation or dental laboratory use and is well tolerated by the patient as there is no postoperative MMF. Patients can enjoy the immediate function of chewing and speaking normally. This treatment of edentulous mandible fractures follows the recommendations of the AO/ASIF, a group of surgeons committed to advancing the care of musculoskeletal injuries, and their principles have been employed successfully all over the world ( Figs. 1.21.12 and 1.21.13 )


The principles of the AO/ASIF group are well accepted and used all over the world. Treatment of edentulous mandible fractures is best accomplished using load-bearing osteosynthesis. Another name for this type of fixation is stabilization by splinting. This requires the plate to withstand the forces of mastication and allow immediate function for the patient. Typically, this requires a reconstruction plate with at least three screws on either side of the fracture. Locking reconstruction plates have been shown to provide adequate stability and have the benefit of a lower incidence of screw loosening.
The open reduction and internal fixation of edentulous mandible fractures can be accomplished via a transoral approach. However, the transoral approach is quite difficult and requires multiple sets of trained hands to assist the surgeon. In the severely atrophic mandible the inferior alveolar nerve and inferior alveolar artery can sit on the crest of the ridge of the mandibular bone because of previous bone absorption and are at risk for damage with intraoral incisions. We have found the extraoral approach permits excellent access to align the fractures and place the reconstruction plates, which often are large. The extraoral approach is our preferred method to treat the edentulous mandible fracture patient. Transcutaneous incisions allow adequate access to place longer reconstruction plates. These patients often have neck skin creases which mask the scar of an extraoral incision to heal with an excellent cosmetic result. Often, temporary stabilization with smaller plates of edentulous mandible fractures is helpful as there are no teeth to provide occlusion. These smaller plates provide temporary fracture reduction and stabilization while the reconstruction plate is being bent and applied to the mandible. Bending templates are used to assist the surgeon in appropriate contouring of the reconstruction plate. The reconstruction plate is placed at the inferior border of the mandible to avoid damage to the inferior alveolar nerve. The temporary plates are removed after the reconstruction plate is in place with all screws applied. The principle of at least 3–4 screws on either side of the fracture provides adequate stability for immediate function. Often, the edentulous mandible fractures bilaterally or in more than one place due to the weak nature of the bone, especially in atrophic mandibles. The reconstruction plate is often taller than the native mandible in cases of severe mandibular atrophy. The bilateral edentulous mandible fracture often requires a single long reconstruction plate adapted from angle to angle to fulfill the requirements for stable fixation. The bone at the fracture sites of atrophic edentulous mandible sites is very often of poor quality. There is dense cortical bone with very little cancellous bone or marrow. Surgeons will often overgraft the fracture with autogenous cancellous bone at the fracture sites after the plate has been applied to augment healing at the fracture site. Additionally mandibular bone height can also be gained with this technique.. Many of these patients are poor surgical candidates for multiple general anesthetics so the open reduction, fixation, and autogenous grafting are performed as a single procedure under anesthetic ( Figs. 1.21.14–1.21.24 ).